Abstract
Orbital emphysema is usually a benign, self-limited condition. Intraorbital extension of the entrapped air in the absence of an orbital fracture is extremely rare. Although benign, a careful periodic monitoring of intraocular pressure, optic nerve examinations, and prompt management are warranted in order to prevent tension pneumoobitus secondary to increasing intraorbital pressure by the orbital air.
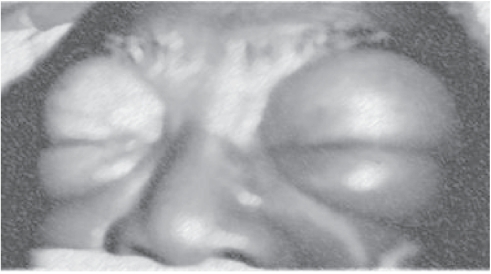
A 60-year-old man with advanced chronic obstructive pulmonary disease (COPD) presented with spontaneous pneumothorax and respiratory failure requiring chest tube placement, intubation, and mechanical ventilation. A large air leak through the chest tube indicated the presence of a bronchopleural fistula. Within hours, he developed massive subcutaneous emphysema involving the entire torso, neck, and face, especially the orbits (Figure ). Ophthalmologic examination showed orbital, conjunctival, and subconjunctival emphysema with mild increase in intraocular tension bilaterally. He was stabilized, underwent thoracotomy with stapling of bullae, and subsequently recovered.
Figure 1 Orbital emphysema: Bilateral massive orbital swellings due to massive orbital emphysema complicating bronchopleural fistula.
Orbital emphysema is generally a benign, self-limited condition, most commonly associated with trauma or surgery involving the sinuses or orbits (CitationCartwright et al 1992). Intraorbital extension of the entrapped air in the absence of an orbital fracture is extremely rare (CitationHunts et al 1994). In this case, orbital emphysema resulted from extension to the eyes of massive subcutaneous emphysema in the setting of a large bronchopleural fistula and positive-pressure mechanical ventilation.
Although uncommon, orbital emphysema may compromise retinal and optic nerve vascularization (CitationHunts et al 1994, CitationWood et al 1996). Visual loss may occur because of tension pneumoorbitus which results from increasing intraorbital pressure by the orbital air; therefore, rapid diagnosis and management are essential (CitationCartwright et al 1992, CitationWood et al 1996). Careful monitoring of intraocular pressure and decompression by needle aspiration or canthotomy with cantholysis, and orbitotomy may be necessary to avert these complications (CitationHunts et al 1994, CitationWood et al 1996). Intraocular pressure monitoring may be critical when orbital emphysema coexists with glaucoma.
References
- CartwrightMGinsburgRNelsonC1992Tension pneumoorbitusOphthal Plast Reconstr Surg83034
- HuntsJPatrinelyJHoldsJ1994Orbital emphysema. Staging and acute managementOphthalmology10196068190488
- WoodBMirvisSShanmuganathanK1996Tension pneumocephalus and tension orbital emphysema following blunt traumaAnn Emerg Med2844698839534