Abstract
Individuals with COPD have systemic inflammation that can be assessed by measuring C-reactive protein (CRP). In this paper we evaluated whether CRP is related to COPD, lung function and rate of lung function decline.
We included 1237 randomly selected subjects (mean age 42, range 28–56 years) from three centers in the European Community Respiratory Health Survey: Reykjavik, Uppsala and Tartu. CRP was measured at the end of the follow-up (mean 8.3 years) and the values were divided into 4 quartiles.
Fifty-three non-asthmatic subjects fulfilled spirometric criteria for COPD (FEV1/FVC < 70%). COPD occurred more often in the 4th CRP quartile (OR (95% CI) 3.21 (1.13–9.08)) after adjustment for age, gender, body weight and smoking. High CRP levels were related to lower FEV1 values in both men (−437 (−596, −279) mL) and women (−144 (−243, −44) mL). The negative association between CRP and FEV1 was significantly larger in men than women (p = 0.04). The decline in FEV1 was larger (16 (5, 27) mL) in men with high CRP levels whereas no significant association between CRP and FEV1 decline was found in women.
Higher CRP values are significantly associated with COPD and lower lung function in men and women. In men higher CRP values are related to a larger decline in FEV1.
Introduction
Chronic obstructive lung disease (COPD) is characterized by a progressive airflow limitation and is associated with an abnormal inflammatory process in the lungs (CitationPauwels et al 2001). COPD is a major cause of morbidity and disability (CitationMurray and Lopez 1996). Forced expiratory volume in one second (FEV1) is a marker of COPD used in staging and evaluating prognosis of the disease and correlates with mortality and health status (CitationJones and Agusti 2006). Factors associated with decline in FEV1 are of interest as they might have prognostic importance in COPD.
C-reactive protein (CRP) is a sensitive marker of inflammation, infection and tissue damage which contributes to host defenses against infection by activating complement pathways (CitationPepys and Hirschfield 2003). Highly sensitive assays for CRP are available and reflect low grade inflammation (CitationWilkins et al 1998).
Elevated levels of CRP have been reported in overweight adults (CitationVisser et al 1999; CitationDanesh et al 2004). Adiposity and weight change have been associated with an unfavorable development in respiratory function (CitationBurchfiel et al 1996; CitationChinn et al 1996; CitationWang et al 1997). In a study estimating the effects of smoking and weight change a gender difference was reported where weight gain seems to diminish the benefit of smoking cessation by 38% in men and by 17% in women (CitationChinn et al 2005).
Studies have demonstrated elevated levels of CRP and fibrinogen in patients with COPD (CitationMannino et al 2003; CitationGan et al 2005) and a meta-analysis by CitationGan et al (2004) confirmed a significant increase in CRP levels in COPD patients compared with controls indicating a persistent systemic inflammation in subjects with COPD. CitationDonaldson et al (2005) examined 148 patients with moderate to severe COPD and showed that high levels of inflammatory markers are associated with a faster decline in lung function.
Smoking is the major contributor to COPD and a fast decline in FEV1 (CitationAnthonisen et al 2002). Numerous reports have shown current smokers to have higher CRP levels than non-smokers (CitationTamakoshi et al 2003; CitationDanesh et al 2004; CitationGan et al 2005) and a positive association with the number of pack-years smoked (CitationFrohlich et al 2003) but interestingly smoking and reduced lung function seem to have independent effects on CRP levels (CitationGan et al 2005).
The aim of this paper was to explore the relationship between CRP, smoking, COPD and lung function in a population sample of young and middle aged adults from Iceland, Estonia and Sweden.
Methods
Population
The European community respiratory health survey (ECRHS) is an international multi-centre epidemiological study of asthma and allergy. The first part, ECRHS I, was conducted in 1990–1994 and the follow-up study, ECRHS II, in 1999–2001. The design of ECRHS I and ECRHS II has been published elsewhere (CitationBurney et al 1994; CitationAnon 2002).
The present study includes data from three of the 29 centers in the ECRHS II: Reykjavik in Iceland, Tartu in Estonia and Uppsala in Sweden – where 2033 subjects participated in stage 2 of ECRHS I (CitationÓlafsdóttir et al 2005). The number of subjects in the present analysis was 1289 (age range 28–56 years), of which 512 subjects were from Reykjavik, 288 from Tartu and 489 from Uppsala (participation rate 63.4%). Mean time between first (ECRHS I) and second spirometry (ECRHS II) was 8.3 ± 0.8 years. Only subjects with CRP measurement and an acceptable spirometry were included in the study (n = 1237).
Subjects were asked to postpone their examination if they had suffered from respiratory infection in the 3 weeks immediately preceding the examination, as this was a criterion for exclusion. Written informed consent was obtained from each subject before inclusion in the study. The relevant ethics authorities in each of the participating research centers approved the protocol.
Smoking
A questionnaire administered on each occasion provided information on smoking history. Those who answered “yes” to the lead question (“Have you ever smoked for as long as a year?”) were asked “Do you smoke now, as of one month ago?” Those that answered yes to the first question and no to the second were considered to be ex-smokers. Additional questions were asked on age at starting, amount smoked currently, whether they had stopped or cut down, and amount smoked previously. Based on this information the subjects were classified into Never-smoker, Ex-smoker and Smokers. Lifetime and between survey exposure to smoking was calculated as pack years (CitationChinn et al 2005).
Spirometry
In all three centers lung function was performed using the same spirometer in ECRHS I and II. The maximum FEV1 and maximum forced vital capacity (FVC) of up to five technically acceptable blows were determined, and also whether FEV1 and FVC each met the American Thoracic Society criterion for reproducibility (CitationAnon 1995). Decline in FEV1 and FVC was expressed per year of follow-up (ECRHS I value minus ECRHS II value) (CitationChinn, Jarvis et al 2005). Predicted values for forced expiratory volume in one second (FEV1) were calculated based on the European Coal and Steel Union reference values (CitationAnon 1983).
Definition of COPD
The criterion for COPD in the present study was a FEV1/FVC < 70% (CitationPauwels et al 2001; Citationde Marco et al 2004). Subjects with an FEV/FVC ≥ 70% that reported usually having cough or bringing up phlegm at least three months each year were defined as being at risk for COPD (Global initiative for chronic obstructive lung disease (GOLD) stage 0) (CitationPauwels et al 2001; Citationde Marco et al 2004). Subject with a self-reported history of physician’s diagnosed asthma were not considered as having COPD or GOLD stage 0.
Body mass index
BMI was calculated as weight in kilograms divided by the square of height in meters.
CRP measurements
CRP was measured at the end of the follow-up period. The analysis was carried out at the Dept. of Clinical Biochemistry, Landspitali University Hospital Iceland. All serum samples were stored frozen at −20 ºC. High sensitivity CRP concentrations were measured on a Hitachi 911 analyzer using a commercially available latex-enhanced immunoturbidimetric assay from Roche. The lower detection limit of the assay is 0.1 mg/L. Two internal control specimens provided by the reagent manufacturer were measured in each batch of samples. The total coefficient of variation for CRP measurements of the internal controls was 1.1% at a concentration of 3.73 mg/L and 1.9% at a concentration of 0.68 mg/L.
Statistical analyses
Log-transformed values of CRP were used when analysing the relationship between CRP and pack years and the association between CRP and FEV1 in subjects with COPD. The subjects were divided into four groups according to the quartile distribution of the CRP values (≤0.45, 0.46–0.96, 0.97–2.21 and >2.21) when estimating risk association. Test for trend was used when analysing associations between CRP-quartiles and age, sex, smoking and BMI in the univariate analyses. Odds ratios for the relationship between COPD and CRP were calculated using logistic regression while multiple linear regressions were used to examine the association between lung function and CRP. Analyses of sex interaction were performed. Analyses of the association between CRP and lung function was performed separately in men and women as a significant sex interaction was found in the association between CRP and FEV1. The adjusted risk ratios and adjusted estimates of the linear regressions with a 95% confidence interval (CI) were first analyzed on pooled data from all three centers, adjusting for centre and then calculated separately at each centre. Potential heterogeneity between centers was examined using standard methods for random-effects meta-analysis.
Results
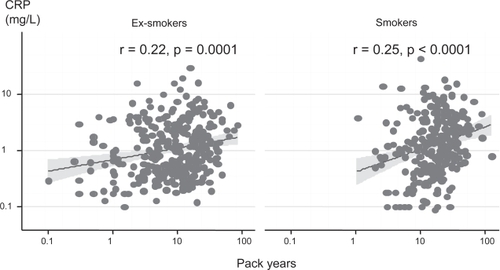
The study population (n = 1237) included 595 men and 642 women, mean age 42 (range 28–56) years, 29.7% ex-smokers and 26.4% current smokers. CRP values ranged from <0.1 to 70.0 mg/L. Characteristics of the study population divided in CRP quartiles are presented in . There were no significant centre or gender differences in CRP levels, but there was a statistically significant positive correlation between CRP and current smoking, pack years and BMI (). The positive association between the number of pack years smoked and CRP was found in both ex-and current smokers ().
Table 1 Characteristics of the study population in relation to CRP values
Figure 1 Correlation between pack years and CRP in ex- and current smokers.
CRP and COPD
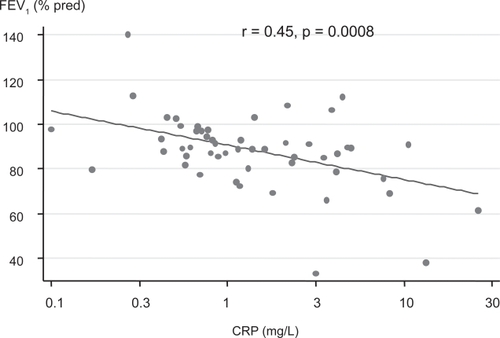
Fifty-three participants (4.2%, 25 men and 28 women) fulfilled the criteria for having COPD and additionally 87 (7.0%) were defined as being at risk for COPD (GOLD stage 0). Eleven subjects had GOLD stage II or more. The lowest prevalence of subjects fulfilling the criteria for COPD was in those with the lowest CRP values and remained significant after adjusting for centre, age, sex, BMI and pack years (). There was no significant relation between CRP and GOLD stage 0. There was a correlation between COPD severity expressed as FEV1 as % of the predicted and CRP in the 53 subjects with COPD (). No significant gender interaction (p = 0.91) or centre heterogeneity was found in the associations between CRP and COPD (p for heterogeneity = 0.31).
Table 2 Prevalence of GOLD stage 0 and COPD and the independent association to CRP
Figure 2 Correlation between CRP values and FEV1 expressed as % of the predicted in subjects with COPD (n = 53).
CRP and lung function
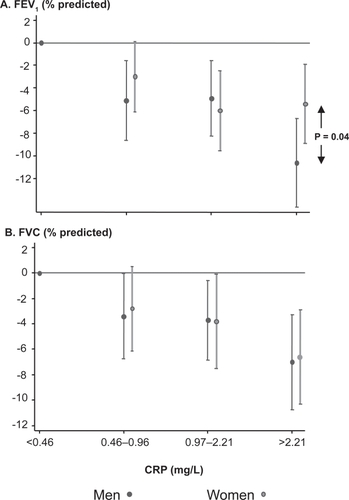
Men and women with CRP values above 0.46 mg/L had significantly lower FEV1 and FVC values than subjects with CRP values within the first quartile (, ). The negative association between CRP and FEV1 was significantly larger in men than women (p = 0.04), whereas no gender difference in the association between CRP and FVC was found (). The mean annual decline in FEV1 was 44 mL in men and 31mL in women. Men with higher CRP values than 0.46 mg/L had a significantly larger decline in FEV1 while no significant association between CRP and decline in lung function was found in women (). Decline in FEV1, when not adjusted for CRP, was also significantly related to elevated BMI in both men and women and to the intensity of smoking between the surveys in women (). In men the association between change in BMI and FEV1 decline increased when not adjusting for CRP [13 (6, 21) mL/year for each 5 unit increase in BMI, (adjusted effect (95% CI)], while no similar effect was found in women.
Table 3 Estimated effect (95% CI) of CRP on lung function. Subjects with CRP value ≤ 0.45 mg/L are the reference group. The values are adjusted for centre, age, (age)2, height, BMI and pack years (estimate in mL (95% CI))
Table 4 Estimated effect (95% CI) of CRP on annual decline in FEV1 (mL/year). Subjects with CRP value ≤ 0.45 mg/L are the reference group. The values are adjusted for centre, age, (age)2, height, BMI at baseline, change in BMI and pack years
Figure 3 Estimated difference in FEV1 (A) and FVC (B) between subjects with different CRP values, where subjects in the 1st CRP quartile are the reference. The estimates are adjusted for age, sex, BMI and pack years.
No significant interaction was found between CRP, smoking and change in body mass index in relation to lung function and decline in FEV1. No centre heterogeneity was found in the associations between CRP and lung function with one exception. A significantly larger decline in FEV1 was found in women with the highest CRP values in Uppsala [15 (6–24) mL/year] (p for heterogeneity = 0.002). No such association was found in the other centres.
Non-participants
Subjects that participated in both surveys (n = 1289) were slightly older (33.7 ± 7.2 vs 32.1 ± 7.0 years), had a higher BMI (23.9 ± 4.0 vs 23.3 ± 3.7 kg/m2) (p < 0.0001) and were less often smokers (32.4 vs 37.0, p = 0.03) in the ECRHS I than the subjects that only participated in the first survey (n = 744).
Discussion
This study focuses on a well-defined general population. It demonstrates a strong association between elevated CRP levels and the prevalence of COPD and lower lung function (FVC and FEV1). The negative association between CRP and FEV1 was stronger in men than women and an association between faster decline of FEV1 and higher CRP levels was found in men but not women.
Our results are in accordance with a cross sectional study from the Third National Health and Nutrition Survey where CRP levels, independent of smoking, were found to be related to reduced FEV1 (CitationGan et al 2005). CitationBroekhuizen et al (2006) showed that in 102 clinically stable COPD patients, 48 had elevated CRP levels (>4.21 mg/l) and these high levels where strongly associated with impaired energy metabolism and distress due to respiratory symptoms. A comparison of 88 COPD patients with 33 smokers and 38 non-smokers controls, showed higher levels of CRP in COPD patients (CitationPinto-Plata et al 2006). In assessing the association between CRP and lung function CitationShaaban et al (2006) looked at cross-sectional and longitudinal changes between CRP and FEV1 decline. Their analysis included 531 subjects demonstrating a negative association between FEV1 and CRP (p = 0.002) and higher CRP levels over time were associated with a faster FEV1 decline. Similarly a recent study found CRP levels associated with accelerated decline in FEV1 and mortality in patients with mild to moderate COPD indicating that CRP measurements might enable identification of patients at a high risk of disease progression and mortality (CitationMan et al 2006).
The present study underscores the link between systemic inflammation and COPD. Many of prior studies have been focused on hospitalized subjects or COPD patients with severe COPD (GOLD III or IV). Our study implies that systemic inflammation is a factor even in the early phase of the COPD process. The exact role of inflammation in the pathogenesis of COPD is not fully understood. Lower airway bacterial colonization (CitationWilkinson et al 2003) and possibly upper airway bacterial inflammation (CitationHurst et al 2005) might provoke a systemic inflammatory response in COPD patients. Elevated levels of inflammatory markers such as plasma fibrinogen have been associated with reduced FEV1, accelerated decline in lung function and increased risk of COPD hospitalizations in the future (relative risk 1.7 (95% CI: 1.1–2.6)) (CitationDahl et al 2001). A prospective study by CitationWilkinson et al (2003) including 30 patients with moderate COPD over 12 months, showed that FEV1 decline was related to an increase in airway bacterial load (r = 0.59, p = 0.001) and higher sputum Il–8 was associated with greater declines in FEV1 (p = 0.03). However, CRP was not reported in these studies. Faster decline in FEV1 has also been associated with more frequent exacerbations of COPD (CitationDonaldson et al 2002) and a recent publication suggested that the chronic deterioration in FEV1 decline is explained by the acute events in COPD causing a faster rate of rise in airway inflammation (CitationDonaldson et al 2005).
In our study men with higher CRP values had significantly larger decline in FEV1 than men with low CRP whereas no such association was found in women. In an epidemiological follow-up study like ours the fast rate of lung function decline and the diagnosis of COPD are strongly interrelated and in other studies it has usually been described as one of the deleterious consequences of smoking (CitationLange et al 1989; CitationTownsend et al 1991; CitationXu et al 1994; CitationBurchfiel et al 1995). Chinn et al studied the effects of smoking cessation and weight gain on lung function in 6654 subjects. They showed gender differences with a significantly faster rate of lung function decline in relation to weight gain in men than women (CitationChinn et al 2005).
We found that the association between weight change and FEV1 decline decreased when adjusting for CRP in men. This might indicate that weight-related effect on change in FEV1 could partly be mediated through increased systemic inflammation. The strong relationship between increased body fat and lower lung function raises the question whether elevated CRP reflects inflammatory processes in the airways that overflow into the systemic circulation, promoting a generalized inflammatory reaction (CitationGan et al 2004). However in a recent review CitationWouters (2005) concluded that the inflammatory process in the airways and the systemic circulation were two independent processes. It is also possible that smoking induces CRP elevation, as a significant relationship was found between number of pack years and CRP levels in both ex- and current smokers in the present study. Alternatively elevated CRP may reflect a genetic or constitutional factor predisposing individuals with COPD to both systemic and pulmonary inflammation (CitationBarnes 2000; CitationHersh et al 2006).
Previously we published that CRP in the same study population is increased in non-allergic but not allergic asthma (CitationÓlafsdóttir et al 2005). In this report COPD was significantly more common in subjects with higher CRP quartiles. Despite adjustments for centre, age, sex, body mass index and pack years, a positive correlation was found between the severity of COPD (FEV1%) and CRP values. The relatively young age of our study population (mean age 42, range 28–56 years) is of great clinical importance, as they have not yet reached the age with repeated hospitalizations due to exacerbations of COPD but do show rapid lung function decline.
The strengths of this study include the use of data from a general population, gathered and assessed with high quality and standardized methods as part of the ECRHS. The limitations merit some discussion. Firstly CRP was only measured at the end of our study while FEV1 was measured at two time points and our assumptions on FEV1 decline are based on these measurements. However, CRP levels measured at multiple time points have been stable in many studies (CitationMacy et al 1997; CitationOckene et al 2001; CitationRidker et al 2005). Secondly we found that the participants were less likely to be smokers and slightly more obese than the non-participants. We cannot rule out selection bias but do not believe that those limitations undermine our work.
The present study indicates that subjects with elevated CRP levels are at greater risk of having COPD and impaired lung function. A significant gender difference was found where men with higher CRP values had a more rapid decline in FEV1 during the study period. Future studies will reveal whether lowering elevated levels of CRP in COPD patients with drugs such as statins (CitationRidker et al 2005) or inhaled corticosteroids in high doses (CitationSin et al 2004) will slow the clinical progress of the main outcome variables in COPD, namely, decline in lung function, number of exacerbations, health related quality of life and mortality. Treatment of a younger population like the one we studied is of particular interest as at their age lung function is rapidly decreasing but loss of health related quality of life is not yet an irreversible fact.
Acknowledgements
We thank AS Ingvarsdottir and VA Gunnlaugsdottir for their expert technical assistance. The study was supported financially by the Icelandic Research Council, the Swedish Heart and Lung Foundation, the Vårdal Foundation for Health Care Science and Allergy Research, the Swedish Association against Asthma and Allergy, and the Estonian Science Foundation grant no 4350.
References
- [Anon]1983Standardisation of lung function tests. European community for Coal SteelClin Respir Phys19Suppl 5227
- [Anon]1995Standardization of spirometry, 1994 update. American Thoracic SocietyAm J Respir Crit Care Med1521107367663792
- [Anon]2002The European Community Respiratory Health Survey II. The European Community Resiratory Health Survey II Steering CommitteeEur Respir J201071912449157
- AnthonisenNRConnettJE2002Smoking and lung function of Lung Health Study participants after 11 yearsAm J Respir Crit Care Med166675912204864
- BarnesPJ2000Chronic obstructive pulmonary diseaseN Engl J Med3432698010911010
- BroekhuizenRWoutersEF2006Raised CRP levels mark metabolic and functional impairment in advanced COPDThorax61172216055618
- BurchfielCMMarcusEB1995Effects of smoking and smoking cessation on longitudinal decline in pulmonary functionAm J Respir Crit Care Med1511778857767520
- BurchfielCMMarcusEB1996Characteristics associated with rapid decline in forced expiratory volumeAnn Epidemiol6217278827157
- BurneyPGLuczynskaC1994The European Community Respiratory Health SurveyEur Respir J7954608050554
- ChinnDJCotesJE1996Longitudinal effects of change in body mass on measurements of ventilatory capacityThorax516997048882076
- ChinnSJarvisD2005Smoking cessation: maximum benefit for lung function requires control of weight gainLancet36516293515885295
- DahlMTybjaerg-HansenA2001Elevated plasma fibrinogen associated with reduced pulmonary function and increased risk of chronic obstructive pulmonary diseaseAm J Respir Crit Care Med16410081111587987
- DaneshJWheelerJG2004C-reactive protein and other circulating markers of inflammation in the prediction of coronary heart diseaseN Engl J Med35013879715070788
- de MarcoRAccordiniS2004An international survey of chronic obstructive pulmonary disease in young adults according to GOLD stagesThorax59120514760151
- DonaldsonGCSeemungalTA2002Relationship between exacerbation frequency and lung function decline in chronic obstructive pulmonary diseaseThorax578475212324669
- DonaldsonGCSeemungalTA2005Airway and systemic inflammation and decline in lung function in patients with COPDChest1281995200416236847
- FrohlichMSundM2003Independent association of various smoking characteristics with markers of systemic inflammation in men. Results from a representative sample of the general population (MONICA Augsburg Survey 1994/95)Eur Heart J2413657212871694
- GanWQManSF2005The interactions between cigarette smoking and reduced lung function on systemic inflammationChest1275586415705996
- GanWQManSFP2004Association between chronic obstructive pulmonary disease and systemic inflammation: a systematic review and a meta-analysisThorax5957458015223864
- HershCPMillerDT2006Genetic determinants of C-reactive protein in COPDEur Respir J2811566216971405
- HurstJRWilkinsonTM2005Relationships among bacteria, upper airway, lower airway, and systemic inflammation in COPDChest12712192615821198
- JonesPWAgustiAG2006Outcomes and markers in the assessment of chronic obstructive pulmonary diseaseEur Respir J278223216585091
- LangePGrothS1989Effects of smoking and changes in smoking habits on the decline of FEV1Eur Respir J2811162806504
- MacyEMHayesTE1997Variability in the measurement of C-reactive protein in healthy subjects: implications for reference intervals and epidemiological applicationsClin Chem435288990222
- ManSFPConnettJE2006C-reactive protein and mortality in mild to moderate chronic obstructive pulmonary diseaseThorax618495316738034
- ManninoDMFordES2003Obstructive and restrictive lung disease and markers of inflammation: data from the Third National Health and Nutrition ExaminationAm J Med1147586212829203
- MurrayCJLLopezAD1996Evidence-based health policy: lessons from the Global Burden of Health StudyScience27474038966556
- OckeneISMatthewsCE2001Variability and classification accuracy of serial high-sensitivity C-reactive protein measurements in healthy adultsClin Chem474445011238295
- ÓlafsdóttirIGíslasonT2005C-reactive protein is elevated in non-allergic but not allergic asthma – a multicentre epidemiological studyThorax60451415923243
- PauwelsRABuistAS2001Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: National Heart, Lung, and Blood Institute and World Health Organization Global Initiative for Chronic Obstructive Lung Disease (GOLD): executive summaryRespir Care4679882511463370
- PepysMBHirschfieldGM2003C-reactive protein: a critical updateJ Clin Invest11118051212813013
- Pinto-PlataVMMullerovaH2006C-reactive protein in patients with COPD, control smokers and non-smokersThorax6123816143583
- RidkerPMCannonCP2005C-reactive protein levels and outcomes after statin therapyN Engl J Med35220815635109
- ShaabanRKonyS2006Change in C-reactive protein levels and FEV(1) decline: a longitudinal population-based studyRespir Med Epub ahead of print.
- SinDDLacyP2004Effects of fluticasone on systemic markers of inflammation in chronic obstructive pulmonary diseaseAm J Respir Crit Care Med170760515229100
- TamakoshiKYatsuyaH2003Long-term body weight variability is associated with elevated C-reactive protein independent of current body mass index among Japanese menInt J Obes Relat Metab Disord2710596512917711
- TownsendMCDuCheneAG1991Pulmonary function in relation to cigarette smoking and smoking cessation. MRFIT Research GroupPrev Med20621371758842
- WangMLMcCabeL1997Weight gain and longitudinal changes in lung function in steel workersChest1111526329187168
- WilkinsJGallimoreJR1998Rapid automated high sensitivity enzyme immunoassay of C-reactive proteinClin Chem44(6 Pt 1)1358619625071
- WilkinsonTMPatelIS2003Airway bacterial load and FEV1 decline in patients with chronic obstructive pulmonary diseaseAm J Respir Crit Care Med1671090512684248
- VisserMBouterLM1999Elevated C-reactive protein levels in overweight and obese adultsJAMA2822131510591334
- WoutersEF2005Local and systemic inflammation in chronic obstructive pulmonary diseaseProc Am Thorac Soc2263316113466
- XuXWeissST1994Smoking, changes in smoking habits, and rate of decline in FEV1: new insight into gender differencesEur Respir J71056617925873