Abstract
Limited information exists regarding measurement, reproducibility and interrelationships of non-invasive biomarkers in smokers. We compared exhaled breath condensate (EBC) leukotriene B4 (LTB4) and 8-isoprostane, exhaled nitric oxide, induced sputum, spirometry, plethysmography, impulse oscillometry and methacholine reactivity in 18 smokers and 10 non-smokers. We assessed the relationships between these measurements and within-subject reproducibility of EBC biomarkers in smokers. Compared to non-smokers, smokers had significantly lower MMEF % predicted (mean 64.1 vs 77.7, p = 0.003), FEV1/FVC (mean 76.2 vs 79.8 p = 0.05), specific conductance (geometric mean 1.2 vs 1.6, p = 0.02), higher resonant frequency (mean 15.5 vs 9.9, p = 0.01) and higher EBC 8-isoprostane (geometric mean 49.9 vs 8.9 pg/ml p = 0.001). Median EBC pH values were similar, but a subgroup of smokers had airway acidification (pH < 7.2) not observed in non-smokers. Smokers had predominant sputum neutrophilia (mean 68.5%). Repeated EBC measurements showed no significant differences between group means, but Bland Altman analysis showed large individual variability. EBC 8-isoprostane correlated with EBC LTB4 (r = 0.78, p = 0.0001). Sputum supernatant IL-8 correlated with total neutrophil count per gram of sputum (r = 0.52, p = 0.04) and with EBC pH (r = −0.59, p = 0.02). In conclusion, smokers had evidence of small airway dysfunction, increased airway resistance, reduced lung compliance, airway neutrophilia and oxidative stress.
Introduction
Cigarette smoking is the major risk factor for the development of chronic obstructive pulmonary disease (COPD). Smokers without COPD have evidence of airway inflammation, small airway dysfunction and bronchial hyperreactivity (CitationCosio et al 1978; CitationTashkin et al 1996; CitationStanescu et al 1998; CitationClark et al 2001; CitationSaetta et al 2001). In a proportion of cases, these pathophysiological abnormalities become amplified, causing airflow obstruction. The early pathophysiological changes caused by smoking therefore form an integral part of the study of COPD.
Spirometry is routinely used to diagnose COPD. Alternative pulmonary function methods such as body plethysmography, which measures lung volumes and airway conductance, and impulse oscillometry (IOS), which measures pulmonary resistance and compliance, provide valuable additional information on pulmonary dynamics. Using these additional methods may provide evidence of the early physiological abnormalities present in smokers without airflow obstruction ie, with normal forced expiratory volume in 1 second (FEV1).
Non-invasive techniques such as induced sputum, exhaled breath condensate (EBC) and exhaled nitric oxide (NO) are being increasingly used to identify biomarkers that are linked to the effects of smoking and the development of airflow obstruction. Although bronchial biopsy remains the gold standard investigation of airway inflammation, these techniques have the benefit of being non-invasive, safe and easily repeatable. There is evidence that smokers without COPD have sputum neutrophilia (CitationPizzicini et al 1996; CitationChalmers et al 2001; CitationRytila et al 2006), increased EBC 8-isoprostane (CitationMontuschi et al 2000) and reduced exhaled NO (CitationKharitonov et al 1995; CitationCorradi et al 1999; CitationMalinovschi et al 2006; CitationRytila et al 2006). Although EBC pH is known to be reduced in COPD patients (CitationKostikas et al 2002), this has not been studied in smokers.
Induced sputum, EBC and exhaled NO measurements have not been investigated during the same study in smokers, so it is not known whether these measurements are independent or related variables in this population group. Induced sputum, EBC and exhaled gas analysis all sample different compartments of the airways by different methods, and can be used to analyze different biological mediators that are involved in a range of inflammatory processes. For this reason, it is important to understand whether biomarkers measured by these techniques provide similar or different information about airway inflammation. For example, it is not known if airway neutrophilia is related to increased 8-isoprostane production or airway acidification in smokers.
EBC measurements can be prone to significant variability (Horvath et al 2005). Although studies have shown raised levels of EBC 8 isoprostane and LTB4 in smokers (CitationMontuschi et al 2000; CitationCarpagnano et al 2003), there have been concerns about the reproducibility of these assays (Citationvan Hoydonck et al 2004; CitationBorrill et al 2005; Rahman 2005).
We report a comprehensive assessment of non-invasive biomarkers of airway inflammation (EBC, exhaled NO and induced sputum), bronchial hyperreactivity (BHR) and lung function (spirometry, plethysmography and IOS) in smokers without airflow obstruction. The primary aims of this study were 1) to compare pulmonary function and non-invasive biomarker data between smokers and non-smokers to gain a comprehensive understanding of the early physiological and inflammatory effects of cigarette smoking, and 2) to investigate the relationships between non-invasive biomarkers in smokers. We also investigated the reproducibility of EBC biomarkers in smokers.
Methods
Subjects and study design
18 current smokers (mean age 46.4 [SD 9.6], 7 male, mean pack years 25.5 [SD 10.3]) and 10 lifelong non-smoking healthy controls (mean age 44.8 [SD 15.6], 4 male) with normal lung function were recruited. Exclusion criteria were; history of asthma or atopy, FEV1 <85% predicted, FEV1/FVC <70%, respiratory tract infection within 2 weeks, any concomitant medication or major concurrent medical condition. Subjects were asked to avoid caffeine and cigarettes for 2 hours prior to each visit. Written informed consent was obtained and the study was approved by the South Manchester Medical Research Ethics Committee, Gateway House, Piccadilly South, Manchester, UK. The study was conducted in accordance with the Declaration of Helsinki of 1975.
Subjects underwent EBC, exhaled NO, respiratory function tests (IOS, plethysmography and spirometry), methacholine challenge and induced sputum assessments in that order (visit 1). One week later, all smokers attended for repeated EBC (visit 2). EBC samples were obtained from all subjects, and were used firstly for 8-isoprostane and LTB4 analysis. After 8-isoprostane and LTB4 analysis there was sufficient sample remaining for pH analysis in all non-smokers, 17 smokers at visit 1, and 14 at visit 2. Adequate sputum samples were obtained from 16 smokers but only 2 non-smokers. Non-smokers’ sputum data was not used further. Methacholine challenge was performed in 15 smokers and all non-smokers. The relationship between non-invasive biomarkers was assessed in smokers at visit 1.
Pulmonary function and methacholine challenge
For IOS (Masterscreen IOS, Erich Jaeger, Hoechberg, Germany) subjects supported their cheeks to reduce upper airway shunting while impulses were applied during tidal breathing for 30 seconds. R5 and R20 (respiratory resistance at 5 and 20Hz respectively), X5 (reactance at 5 Hz) and RF (resonant frequency) were recorded. Airways resistance (Raw), specific conductance (sGaw), functional residual capacity (FRC), vital capacity (VC), inspiratory capacity (IC), total lung capacity (TLC) and residual volume (RV) were measured in a constant volume plethysmograph (Vmax 6200, Sensormedics, Bilthoven, Netherlands). IOS and body plethysmograph measurements were performed in triplicate and the mean calculated. Maximum expiratory flow volume measurements (FEV1, forced expiratory volume in one second, FVC, forced vital capacity and MMEF, maximum mean expiratory flow) were performed using a spirometer (Super Spiro, Micromedical, Rochester, UK). Readings were performed in triplicate, with the highest measurement used.
Methacholine challenge was performed using a previously described method (CitationLangley et al 2002). A DeVilbiss 646 nebuliser (Sunrise medical, Wollaston, UK) and a Rosenthal dosimeter (PDS research, Gravesend, UK) were used to deliver doubling doses of methacholine, administered using 3 stock concentrations (1.5 mg/ml, 12 mg/ml and 50 mg/ml; Stockport pharmaceuticals, Stockport, UK). FEV1 measurements were made immediately before the challenge procedure, one minute after the administration of saline and one minute after each dose of methacholine. Doubling doses of methacholine starting at 0.015 mg were administered until a fall of ≥20% from the post-saline FEV1 was observed or the maximum dose of methacholine (5.96 mg) had been administered.
Exhaled breath condensate
EBC was collected during tidal breathing for 10 minutes (EcoScreen, Jaeger, Hoechberg, Germany) without a nose peg as previously described (CitationBorrill et al 2005). Samples were aliquoted into separate 200 μl tubes and frozen at −80 °C for later analysis. Argon gas was passed over the sample at 2L/min for 10 minutes to achieve gas standardisation, after which pH was measured using pH 210 meter (Hanna instruments, Bedfordshire, UK) with a Biotrode electrode (Hamilton, Nevada, US). LTB4 and 8-isoprostane were measured by enzyme immunoassays (Cayman Chemical, Ann Arbour, MI, USA). All samples were analysed in triplicate. The lower limits of detection were 13 pg/ml and 5 pg/ml for LTB4 and 8-isoprostane respectively.
Exhaled nitric oxide
Exhaled nitric oxide was measured using a chemiluminescence analyser according to the ATS guidelines (CitationAmerican Thoracic Society 1999). The results from 5 different flow rates (10, 30, 50, 100 and 200 ml/s) were applied to one non-linear (CitationSilkoff et al 2000) and two mixed linear and non-linear mathematical models (CitationPietropaoli et al 1999; CitationHogman et al 2002) with the following unknown variables; CawNO (concentration of NO in the airway wall), CalvNO (alveolar concentration) and DawNO (diffusing capacity of NO from the airway wall). Total maximal airway wall NO flux (J’awNO in pl/s) was also calculated as the product of CawNO and DawNO.
Induced sputum
Sputum was induced and processed as previously described (CitationPizzicini et al 1996). Briefly, sputum was induced using 3%, 4%, and 5% saline, inhaled in sequence for 5 min each via an ultrasonic nebulizer (Ultraneb 2000, Medix, Harlow, UK) 20 minutes after 200 mcg inhaled salbutamol. Once expectorated, the sputum was stored on ice and processed within 1 hour. Sputum was selected from saliva and treated by adding four volumes of 0.1% dithiothreitol, followed by four volumes of phosphate buffered saline (Sigma, St Louis, MO, USA). The suspension was then filtered through 48 mcm nylon gauze (Sefar, Bury, UK) and centrifuged at 2000 rpm for 10 minutes. The resulting supernatant was stored at −80 °C for later analysis. Total leukocyte count and evaluation of cell viability (trypan blue exclusion method) was made and the cell suspension adjusted to 1.0 × 106/ml. Cytospin preparations were made with 50 mcl and 100 mcl of the cell suspension (Cytospin 4, Shandon, Runcorn, UK) after which slides were air dried, fixed with methanol and stained with Rapi-diff (Triangle, Skelmersdale, UK). Four hundred leukocytes were counted and the results expressed as a percentage of the total leukocyte count. Supernatant IL-8 was measured using a commercially available quantitative enzyme linked sandwich immunoassay (ELISA, R&D Systems Europe, Oxon, UK) with a lower limit of detection of 15.625 pg/ml.
Statistical analysis
PD20, sGaw, EBC 8-isoprostane, EBC LTB4, percentage eosinophil count, percentage lymphocyte count and absolute cell counts were normally distributed after natural log transformation and are expressed as geometric mean (SD). EBC pH data were not normally distributed and are expressed as median (range). All other data including supernatant IL-8, percentage neutrophil and macrophage counts were normally distributed and expressed as mean (SD). Parametric data and natural log transformed data were compared using unpaired t tests, and correlated using Pearson’s correlations. EBC pH data were compared using Mann-Whitney U test and correlated with other non-invasive biomarkers using Spearman’s correlations. Significance was defined as a p value of <0.05. Subjects who did not react to the highest dose of methacholine were assigned a PD20 of 11.92 mg (2 × maximum dose). Between day variability in smokers was analysed using the Bland Altman method expressed as mean difference and limits of agreement (CitationBland and Altman 1986).
Results
Comparison of smokers and non-smokers
Lung function
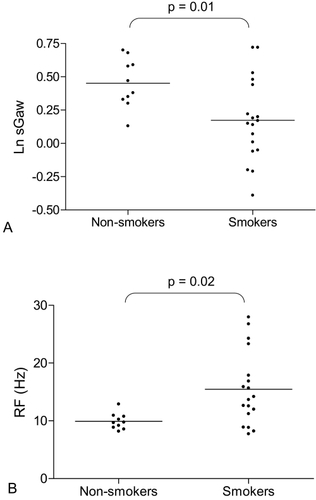
As a group, smokers had significantly lower MMEF and sGaw, and significantly higher RF compared to non-smokers (, ). FEV1/FVC was not quite significantly lower in smokers compared to non-smokers (p = 0.05) ().
Table 1 Pulmonary function, bronchial hyperreactivity, exhaled breath condensate and exhaled nitric oxide results in smokers and non-smokers
Figure 1 (A) Natural log (Ln) sGaw in non-smokers and smokers. Non-smokers (n = 10) and smokers (n = 18). Bars represent geometric means, t test used for comparison. (B) Resonant frequency (RF) in non-smokers and smokers. Non-smokers (n = 10) and smokers (n = 18). Bars represent means, t test used for comparison.
Methacholine challenge
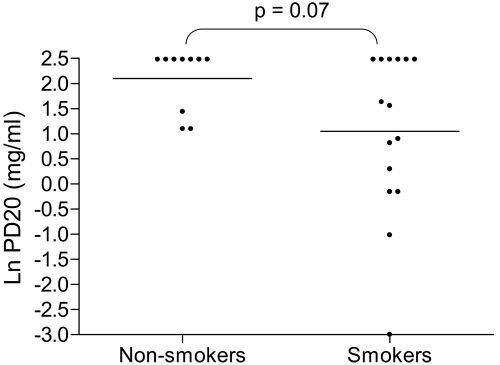
A numerically higher proportion of smokers reacted to methacholine (ie, PD20 of 5.96 mg or less) compared to non-smokers (60% versus 30%) with a trend towards increased BHR in smokers that did not reach statistical significance (p = 0.07) (, ).
Figure 2 Natural log (Ln) methacholine challenge PD20 in non-smokers and smokers. Non-smokers (n = 10) and smokers (n = 15). Bars represent geometric means, t test used for comparison.
Exhaled breath condensate
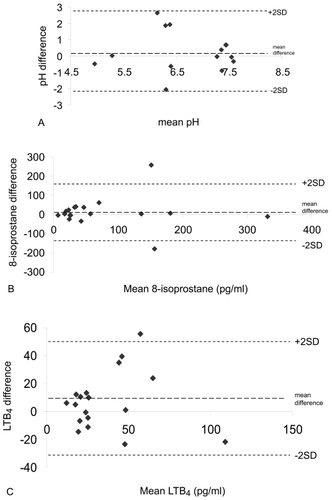
8-isoprostane was significantly higher in smokers compared to non-smokers (, ). In contrast, levels of LTB4 did not differ between the 2 groups (). There was no statistical difference between the median values of EBC pH in smokers and non-smokers (, ). However, there was evidence of airway acidification in some smokers; 5 smokers had very acidic EBC pH (less than 6). In contrast, the pH values in all non-smokers were greater than 7.2. While the within subject mean differences in EBC biomarkers was small and statistically insignificant (p > 0.05 for all comparisons), Bland Altman analysis revealed wide limits of agreement indicating marked between day variability in some individuals ().
Figure 3 (A) Natural log (Ln) exhaled breath condensate 8-isoprostane concentration in non-smokers and smokers. Non-smokers (n = 10) and smokers (n = 18). Bars indicate geometric mean values, t test used for comparison. (B) Exhaled breath condensate pH in non-smokers and smokers. Non-smokers (n = 10) and smokers (n = 17). Bars indicate median values, Mann-Whitney U test used for comparison.
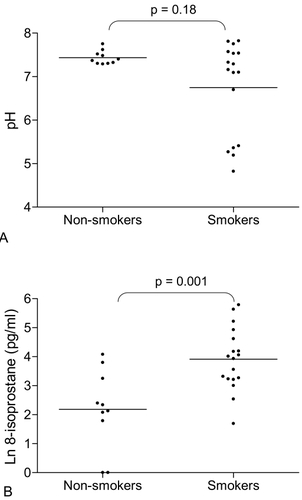
Figure 4 (A) Bland Altman plot of EBC pH reproducibility between visit 1 and visit 2 (n = 14). (B) Bland Altman plot of EBC 8-isoprostane reproducibility between visit 1 and visit 2 (n = 18). (C) Bland Altman plot of EBC LTB4 reproducibility between visit 1 and visit 2 (n = 18).
Exhaled NO
FeNO at 50 ml/s and non-linear model derived parameters using multiple flow rates did not differ between the 2 groups (). Similarly, data derived using two other NO models did not differ between smokers and non-smokers (data not shown).
Induced sputum
The predominant cell type in smokers was neutrophils. Mean (SD) percentage neutrophil and macrophage count were 68.5% (18.8) and 30.4% (18.8) respectively. Geometric mean percentage eosinophil count and lymphocyte count (SD) were 0.51 (2.54), and 0.35 (2.31) respectively. Geometric mean (SD) total cell, neutrophil and macrophage count per gram of selected sputum were 1.2 (2.6) × 106, 0.8 (3.1) × 106 and 0.3 (2.6) × 106 respectively. Mean (SD) supernatant IL-8 concentration was 322.5 (154.7) pg/ml.
Correlations between non-invasive inflammatory markers in smokers
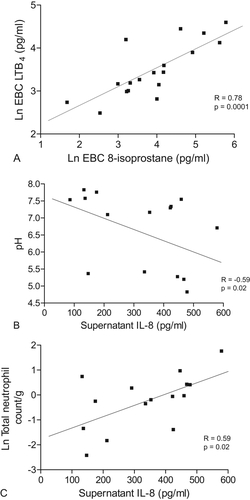
There was a significant correlation between EBC 8-isoprostane and LTB4 (r = 0.78, p < 0.0001) in smokers (, ). However, 8-isoprostane and LTB4 did not correlate with sputum neutrophilia or with any other measurements (p > 0.05 for all comparisons, ). Sputum supernatant IL-8 correlated significantly with EBC pH (r = −0.59, p = 0.02 , ), total neutrophil count per gram of sputum (r = 0.59, p = 0.02, , ) and total cell count per gram of sputum (0.54, p = 0.04, ). Exhaled NO (including model derived parameters) showed no significant correlations with the other measurements (p > 0.05 for all comparisons, data not shown).
Table 2 Correlations between non-invasive biomarkers. Data are Spearman’s correlations for EBC pH data and Pearson’s correlations for all other data
Figure 5 (A) Pearson’s correlation in smokers between natural log (Ln) exhaled breath condensate 8-isoprostane and LTB4 (n = 18). (B) Spearman’s correlation in smokers between sputum supernatant IL-8 (pg/ml) and EBC pH (n = 15). (C) Pearson’s correlation in smokers between sputum supernatant IL-8 (pg/ml) and natural log (Ln) sputum total neutrophil count (n = 15).
Discussion
The major findings of this study were that the sensitive techniques of plethysmography and IOS showed the detrimental effects of smoking even while FEV1 was normal, and that smokers had raised EBC 8-isoprostane and sputum neutrophilia, while a proportion had acidified airway pH. Reduced EBC pH has been reported in established COPD (CitationKostikas et al 2002) but this is the first study to demonstrate acidification of EBC in smokers without COPD. The significant association between sputum IL-8 and EBC pH is suggestive of links between airway acidity and airway inflammation in smokers. We also observed considerable variability in EBC measurements. These key findings are now discussed in more detail.
Comparison of smokers and non-smokers
Smokers with normal lung function are known to have increased mucosal inflammation, mucus hypersecretion and pathological changes typical of early emphysema (CitationClark et al 2001; CitationSaetta et al 2001). The current study suggests that these pathological abnormalities lead to reduced MMEF, reduced sGaw and increased RF. The spirometric abnormalities observed in the current study have been previously reported (CitationClark et al 2001; CitationD’Ippolito et al 2001). To our knowledge, this is the first study to also use body plethysmography and IOS. There is published oscillometry evidence (using a forced random noise generator) that smokers have abnormal RF20 (CitationHayes et al 1979). Abnormalities of MMEF and RF may be due to peripheral airway dysfunction (CitationCosio et al 1978; CitationBouaziz et al 1996; CitationKaczka et al 1999). We also observed reduced sGaw in smokers, indicating that the decreased airway conductance found in COPD patients (CitationMitchell et al 1967) is also present in smokers. Overall, these findings demonstrate that in smokers with normal FEV1 there is small airway dysfunction, decreased airway conductance and reduced lung compliance.
A numerically higher number of smokers had methacholine hyperreactivity compared to non-smokers, although there was no difference between the group PD20 mean values. This may have been due to insufficient sample size. Nevertheless, our results show that bronchial hyperreactivity is present is some smokers, and previous data indicates that these subjects may be at increased risk of COPD (CitationTashkin et al 1996).
Acidified EBC pH has been reported in established COPD (CitationKostikas et al 2002) but there are no reports of EBC pH in smokers without COPD. We found that several smokers had very acidic EBC pH (< 6), a phenomenon observed in COPD but not in non-smokers (CitationBorrill et al 2005, Citation2006). Although the median pH values of smokers and non-smokers were not statistically different, it is clear that a subgroup of smokers have acidic airway pH. The reasons for this finding are unclear. It has previously been reported that airway acidification is related to bacterial colonisation in bronchiectasis and to neutrophilic inflammation and oxidative stress in COPD (CitationKostikas et al 2002). This study provides supporting evidence to suggest a link between neutrophilic inflammation and airway acidity, demonstrating a correlation between sputum supernatant IL-8 and EBC pH. Cigarette smoke contains substances capable of causing oxidative stress and cellular toxicity (CitationMcNee and Rahman 2001). These properties alter airway cell function, increasing levels of airway inflammation in smokers. Such altered cell function may also lead to airway acidification, either due to increased acid production, or decreased buffering capacity. Further work is needed to elucidate the reasons for and importance of airway acidification in smokers.
We observed increased levels of the oxidative stress biomarker EBC 8-isoprostane in smokers compared to non-smokers in agreement with a previous report (CitationMontuschi et al 2000). This was demonstrated despite the recent observation that use of the EcoScreen results in lower levels of 8-isoprostane than other condenser coatings (CitationRosias et al 2006). However, we found no difference in EBC LTB4 between smokers and controls. This is in contrast to a previous study using the same immunoassay method; while LTB4 levels were higher in smokers compared to non-smokers, it should be noted that the levels reported were much lower compared to the current study (CitationMontuschi et al 2003). Furthermore, recent work has suggested that LTB4 present in EBC is mainly due to salivary contamination (CitationGaber et al 2006). Analysis of inflammatory markers in EBC has not been standardized, and reported levels of LTB4 and 8-isoprostane vary (CitationMontuschi et al 2000; CitationKostikas et al 2003; CitationMontushci et al 2003; Citationvan Hoydonck et al 2004). Alternative methods such as mass spectrometry may improve variability and sensitivity (CitationCap et al 2004; CitationMontuschi et al 2004).
Previous studies have shown reduced FeNO in smokers compared to non-smokers (CitationKharitonov et al 1995; CitationCorradi et al 1999; CitationRytila et al 2006), probably through inhibition of nitric oxide synthase activity (CitationHoyt et al 2003). However, increased numbers of inducible nitric oxide synthase positive cells have also been observed in sputum from smokers compared to non-smokers (CitationRytila et al 2006). In the current study there was no difference in FeNO between smokers and non-smokers, and no reduction in the bronchial wall concentration of NO in smokers in contrast to previous studies (CitationHogman et al 2002; CitationMalinovschi et al 2006). Levels of exhaled NO in smokers are determined by the balance between inhibition of nitric oxide synthase activity caused by smoking and upregulation of this enzyme caused by inflammation, as well as NO consumption which may be affected by a variety of factors including the levels of reactive oxygen species (CitationIchinose et al 2000) and the degree of bacterial colonization (CitationGaston et al 2002). We speculate that the smokers in the current study had levels of airway inflammation that counter-balanced the inhibitory effect of smoking on exhaled NO levels.
We were unable to obtain induced sputum specimens from the majority of healthy non-smokers in this study. However, it is known that macrophages are the predominant cell type in induced sputum from healthy non-smokers (CitationBelda et al 2000). In contrast, smokers in this study had predominant neutrophilia. Pizzichini et al showed a trend towards increased neutrophilia in smokers with non-obstructive chronic bronchitis and predominant neutrophilia in established COPD (CitationPizzichini et al 1996). Studies have also observed increased neutrophilia in smokers with normal FEV1 compared to non-smokers (CitationChalmers et al 2001; CitationRytila et al 2006). Neutrophils play a key role in innate immunity, and it is clear that an abnormal innate immune response is present in the airways of smokers with and without COPD.
Reproducibility of EBC biomarkers in smokers
We assessed the reproducibility of EBC biomarkers using the Bland-Altman method, which calculates the limits of agreement (ie, the range of variation that can be expected for repeated measurements from the same subject) (CitationBland and Altman 1986). This is the first report of the variability of EBC pH, 8-isoprostane and LTB4 in smokers. Overall, our results for all measurements demonstrated only small changes in group mean differences over 1 week. However, the variability between individual measurements (determined by the limits of agreement) may be relatively large. Using limits of agreement, we have recently shown considerable within subject variability of EBC 8 isoprostane and LTB4 in COPD patients (CitationBorrill et al 2007) and of EBC pH from COPD patients compared to healthy controls (CitationBorrill et al 2005). We believe that this increased variability compared to that observed in healthy subjects is due to greater changes in airway inflammation over time in COPD patients. Similarly, the results in the current study suggest that these changes in airway inflammation over time also occur in smokers.
Although the current study used a relatively small sample size, we were still able to adequately assess the reproducibility of the EBC biomarkers. For 8-isoprostane and LTB4, the poor reproducibility contributes to the reduced sensitivity of these measurements in small sample sizes. However, despite these issues, this study still provides some novel insights into the effects of smoking on the airways.
Correlations in smokers
There was a strong correlation between exhaled breath condensate LTB4 and 8-isoprostane in smokers. However, there were no significant correlations between these 2 biomarkers and EBC pH. Similarly, it has been shown in COPD patients that EBC pH and 8-isoprostane are not related (CitationKostikas et al 2003). While pH did not relate to other EBC measurements, there was a significant correlation between EBC pH and sputum supernatant IL-8, a potent neutrophil chemoattractant. This suggests that airway acidification is related to neutrophilic influx in smokers. Indeed in COPD patients a similar relationship was observed between EBC pH and sputum neutrophilia (CitationKostikas et al 2002), although in our study this relationship failed to reach statistical significance. Our observation of a significant correlation between sputum supernatant IL-8 and both total cell count and total neutrophil count are in agreement with a previous study (CitationChalmers et al 2001).
Conclusion
The pathological processes of airway inflammation and oxidative stress were demonstrated in smokers using non-invasive biomarkers. The positive relationship observed between sputum IL-8 and EBC pH suggests that airway acidity is related to neutrophilic inflammation. Therefore, these techniques may be useful in the early detection of cigarette smoke-induced pathophysiological abnormalities. However, our EBC reproducibility data adds to the growing body of evidence indicating that the sensitivity and reproducibility of 8 isoprostane and LTB4 assays need to be improved.
Competing interests
No financial or other potential conflicts of interest exist with regard to this study for any of the contributing authors.
Acknowledgements
We acknowledge the assistance of Andrew Hazel with the exhaled nitric oxide models.
Funding source This study was funded by a grant from Glaxo Smith Kline. The study sponsors (via the listed author) were involved in the study design, data analysis and interpretation, writing the report and the decision to submit the paper for publication. They had no role in the collection of data from subjects.
References
- American Thoracic SocietyRecommendations for standardised procedures for the online and offline measurement of exhaled lower respiratory nitric oxide and nasal nitric oxide in adults and childrenAm J Respir Crit Care Med199916021041710588636
- BeldaJLeighRParameswaranKInduced sputum cell counts in healthy adultsAm J Respir Crit Care Med2000161475810673188
- BlandJMAltmanDGStatistical methods for assessing agreement between 2 methods of clinical measurementLancet19861307102868172
- BorrillZStarkeyCVestboJReproducibility of exhaled breath condensate pH in chronic obstructive pulmonary diseaseEur Respir J2005252697415684290
- BorrillZLSmithJANaylorJThe effect of gas standardisation on exhaled breath condensate pHEur Respir J200628251216816353
- BorrillZLStarkeyRCSinghSDVariability of exhaled breath condensate leukotriene B4 and 8-isoprostane in COPD patientsInt J COPD2007 in press
- BouazizNBeyaertCGauthierRRespiratory system reactance as an indicator of the intrathoracic airway response to methacholine in childrenPediatr Pulmonol1996227138856798
- CapPChladekJPehalFGas chromatography/mass spectrometry analysis of exhaled leukotrienes in asthmatic patientsThorax2004594657015170025
- CarpagnanoGEKharitonovSAFoschino-BarbaroMPIncreased inflammatory markers in the exhaled breath condensate of cigarette smokersEur Respir J2003215899312762340
- ChalmersGWMacLeodKJThomsonLSmoking and airway inflammation in patients with mild asthmaChest200112019172211742922
- ClarkKDWardrobe-WongNElliottJJPatterns of lung disease in a normal smoking population. Are emphysema and airflow obstruction found together?Chest2001120743711555504
- CorradiMMajoriMCaccianiGCIncreased nitric oxide in patients with stable chronic obstructive pulmonary diseaseThorax199954572510377199
- CosioMGhezzoHHoggJCThe relations between structural changes in small airways and pulmonary-function testsN Engl J Med1978298127781651978
- D’IppolitoRForesiAChattaAEosinophils in induced sputum from asymptomatic smokers with normal lung functionRespir Med2001959697411778794
- GaberFAcevedoFDelinISaliva is one likely source of leukotriene B4 in exhaled breath condensateEur Respir J20062812293516971403
- GastonBRatjenFVaughanJWNitrogen redox balance in the cystic fibrosis airway: effects of antipseudomonal therapyAm J Respir Crit Care Med20021653879011818326
- HayesDAPimmelRLFulltonJMDetection of respiratory mechanical dysfunction by forced random noise impedence parametersAm Rev Respir Dis197912010959507525
- HogmanMHolmkvistTWegenerTExtended NO analysis applied to patients with COPD, allergic asthma and allergic rhinitisRespir Med200296243011863206
- HorvathIHuntJBarnesPJExhaled breath condensate: methodological recommendations and unresolved questionsEur Respir J2006265234816135737
- HoytJCRobbinsRAHabibMCigarette smoke decreases inducible nitric oxide synthase in lung epithelial cellsExp Lung Res200329172812652813
- IchinoseMSugiuraHYamagataSIncrease in reactive nitrogen species production in chronic obstructive pulmonary disease airwaysAm J Respir Crit Care Med2000162701610934109
- KaczkaDWIngenitoEPIsraelEAirway and lung tissue mechanics in asthma. Effects of albuterolAm J Respir Crit Care Med1999159169789872836
- KharitonovSARobbinsRAYatesDAcute and chronic effects of cigarette smoking on exhaled nitric oxideAm J Respir Crit Care Med1995152609127543345
- KostikasKPapatheodorouGGanasKpH in expired breath condensate of patients with inflammatory airways diseasesAm J Respir Crit Care Med200216513647012016097
- KostikasKPapatheodorouGPsathakisKOxidative stress in expired breath condensate in patients with COPDChest200312413738014555568
- LangleySJHoldenJDerhamAFluticasone Propionate via the Diskhaler or Hydrofluoroalkane-134a metered-dose inhaler on methacholine-induced airway hyperesponsivenessChest20021228061112226017
- MalinovschiAJansonCHolmkvistTEffect of smoking on exhaled nitric oxide and flow-independent nitric oxide exchange parametersEur Respir J2006283394516641119
- MacNeeWRahmanIIs oxidative stress central to the pathogenesis of chronic obstructive pulmonary disease?Trends Mol Med20017556211286755
- MitchellMWatanabeSRenzettiADEvaluation of airway conductance measurements in normal subjects and patients with chronic obstructive pulmonary diseaseAm Rev Respir Dis196796685916051203
- MontuschiPCollinsJCiabattoniGExhaled 8-isoprostane as an in vivo biomarker of lung oxidative stress in patients with COPD and healthy smokersAm J Respir Crit Care Med20001621175710988150
- MontuschiPKharitonovSACiabattoniGExhaled leukotrienes and prostaglandins in COPDThorax200358585812832671
- MontuschiPMartelloSFelliMIon trap liquid chromatography/tandem mass spectrometry analysis of leukotriene B4 in exhaled breath condensateRapid Commun Mass Spectrom2004182723915499663
- PietropaoliAPPerilloIBTorresASimiltaneous measurement of nitric oxide production by conducting and alveolar airways of humansJ Appl Physiol19998715324210517788
- PizzichiniEPizzichiniMMMEfthimiadisAIndices of airway inflammation in induced sputum: reproducibility and validity of cell and fluid-phase measurementsAm J Rspir Crit Care Med199615430817
- RahmanIReproducibility of oxidative stress biomarkers in breath condensate: are they reliable?Eur Resp J2004231834
- RosiasPPRobroeksCMNiemarktHJBreath condenser coatings affect measurement of biomarkers in exhaled breath condensateEur Respir J20062810364116870660
- RytilaPRehnTIlumetsHIncreased oxidative stress in asymptomatic current chronic smokers and GOLD stage 0 COPDRespir Res200676916646959
- SaettaMTuratoGMaestrelliPCellular and structural bases of chronic obstructive pulmonary diseaseAm J Respir Crit Care Med20011631304911371392
- SilkoffPESylvesterJTZamelNAirway nitric oxide diffusion in asthma. Role in pulmonary function and bronchial responsivenessAm J Respir Crit Care Med200016112182810764315
- StanescuDSannaAVeriterCIdentification of smokers susceptible to development of chronic airflow limitation. A 13-year follow-upChest1998114416259726724
- TashkinDPAltoseMDConnettJEMethacholine reactivity predicts changes in lung function over time in smokers with early chronic obstructive pulmonary diseaseAm J Respir Crit Care Med19961531802118665038
- van HoydonckPGAWuytsWAVanaudenaerdeBMQuantitative analysis of 8-isoprostane and hydrogen peroxide in exhaled breath condensateEur Respir J 200420042318992