Abstract
Background
Although combination therapy with bronchodilators is recommended for chronic obstructive pulmonary disease (COPD), there is insufficient evidence for the efficacy of some combinations of long-acting bronchodilators.
Objective
We investigated the effects of a combination therapy with tiotropium and theophylline in COPD patients.
Methods
In a 12-week, open-labeled, parallel-group randomized study, pulmonary functions and dyspnea scores were compared between the combination and theophylline alone therapy at baseline, and 4 and 8 weeks after randomization in COPD.
Results
Sixty-one COPD patients completed the trial (31 combination therapy, 30 theophylline alone; mean age 70 years; 58 males; mean dyspnea score 2.0 and forced expiratory volume in one second (FEV1) 1.5 L [62.5% predicted]). FEV1 in the combination group, but not in the theophylline alone, was significantly increased at 4 (1.56 ± 0.13 L, p < 0.001) and 8 weeks (1.60 ± 0.13 L, p < 0.001) from the baseline (1.40 ± 0.12 L). In the combination group, but not the theophylline alone group, the dyspnea score was significantly improved after 4 (p < 0.01) and 8 weeks (p < 0.05) compared with baseline. In 17 patients who did not receive theophylline at screening, treatment with 4 or 8 weeks of theophylline alone did not improve dyspnea score or FEV1.
Conclusion
Addition of tiotropium therapy to theophylline treatment can improve dyspnea and pulmonary function in COPD. Although this study did not assess whether there was any benefit of adding theophylline to patients treated with tiotropium, tiotropium can be a useful addition in COPD already treated with theophylline.
Introduction
Chronic obstructive pulmonary disease (COPD) is characterized by progressive airway obstruction, chronic respiratory symptoms, and impaired health status, and it is a leading cause of morbidity and morality worldwide (CitationGold 2006). COPD is treatable, and pharmacological treatment is effective in controlling symptoms and health status. In particular, the use of bronchodilators plays a central role in the pharmacological treatment of symptomatic COPD patients. Bronchodilators improve airway obstruction, symptom control, health status, and health-related quality of life (QOL), and they reduce the frequency of exacerbations (CitationDonohue 2005; CitationGold 2006).
Tiotropium bromide is a long-acting anticholinergic that provides sustained bronchodilation through prolonged M3 muscarinic receptor blockade (CitationDisse et al 1999). Previous studies have shown that inhaled tiotropium improves pulmonary function, dyspnea, and QOL in COPD to a significantly greater extent than placebo or the short-acting anticholinergic ipratropium (CitationCasaburi et al 2002; CitationVincken et al 2002). Tiotropium also reduces COPD exacerbations and may reduce related utilization of health-care facilities in patients with moderate to severe COPD (CitationNiewoehner et al 2005; CitationDusser et al 2006). Furthermore, one recent study based on a retrospective 1-year analysis has raised the possibility that tiotropium is associated with a reduced rate of loss of forced expiratory volume in 1 second (FEV1) (CitationAnzueto et al 2005).
Oral slow-released theophylline is used widely as a bronchodilator worldwide (CitationTurner-Warwick 1957; CitationJackson et al 1964; CitationMitenko and Ogilvie 1973). Previous studies have reported that long-term theophylline use for COPD results in improvement of pulmonary functions, including vital capacity (VC), FEV1, minute ventilation, and gas exchange (CitationMurciano et al 1989). Theophylline also has a beneficial effect on exercise endurance in COPD (CitationGuyatt et al 1987). Recent studies have shown that theophylline reduces the numbers of neutrophils and concentrations of interleukin-8 in the airways of COPD patients (CitationCulpitt et al 2002). Low-dose theophylline can also prevent oxidative stress, and it restores corticosteroid responsiveness (CitationIto et al 2002). These results suggest that theophylline has anti-inflammatory effects in COPD, as it does in asthma (CitationSullivan et al 1994).
The GOLD (Global Initiative for Chronic Obstructive Lung Disease) guidelines recommend combination therapy with different potential bronchodilators for the pharmacological treatment of COPD (CitationGold 2006). Theophylline has an additional effect in the clinical improvement of COPD when it is used in combination with a long-acting β2-agonist (LABA) (CitationZuwallack et al 2001). However, few investigations have reported the efficacy of combination therapy with inhalation of the long-acting anticholinergic tiotropium and oral administration of slow-release theophylline in COPD patients. In Japan, theophylline is prescribed for most COPD patients (CitationIchinose et al 2006). Our purpose was to investigate the efficacy and safety of add-on treatment with tiotropium in COPD patients treated with theophylline.
Material and methods
The study was performed at Kurume University Hospital and at each medical institute of the Kurume COPD Study Group. The protocol was designed in accordance with good clinical practice and the latest revisions to the Declaration of Helsinki, and was approved by the institutional ethics committees of Kurume University and each medical institute.
Subjects
COPD patients ≥40 years old and with a cigarette smoking history of ≥10 pack-years and respiratory symptoms related to COPD were enrolled in the study. All patients were diagnosed on the basis of clinical history, physical examination, chest X-ray, chest computed tomography, and pulmonary function tests, in accordance with the clinical criteria for the diagnosis and severity of COPD by the GOLD guidelines (CitationGold 2006). Patients with a history of asthma, atopy, absolute peripheral eosinophil count >600 mm3, and/or reversibility of FEV1 by >200 mL and >12% after inhalation of 200 μg salbutamol were carefully excluded. Patients who had a history of renal failure, moderate to severe prostatic hypertrophy or bladder-neck obstruction, narrow-angle glaucoma, heart failure, arrhythmia, bronchiectasis, pneumoconiosis, old mycobacterial infections, interstitial pneumonia, mental disorders, lung surgery, or any malignancies were also excluded. Five patients (16.6%) in the theophylline alone group and two patients (6.5%) in the combination group were being treated with inhaled corticosteroids at the screening visit. There was no significant difference of number between the two groups (p = 0.2554). Written informed consent was obtained from all patients.
Study design
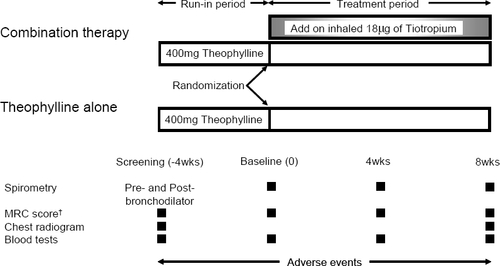
The study was performed over a 12-week period. We used an open-labeled, parallel-group, randomized design to compare the efficacy and safety of the addition of 18 μg inhaled tiotropium once daily to theophylline in stable COPD patients. The primary end-point for this study was the change in FEV1 from baseline to the end of 8 weeks after treatment, and the secondary end-points were the British MRC (Medical Research Council) dyspnea scale and forced vital capacity (FVC).
At the first visit, each patient underwent recording of medical, occupational, and smoking history; physical examination; chest radiography, including high-resolution computed tomography; electrocardiogram; blood testing; and spirometry as screening tests to ensure that they met the inclusion criteria. The spirometry was performed before and after inhalation of a bronchodilator at the first visit. Dyspnea was scored using the British MRC dyspnea scale (CitationMoor-Jankowski 1976). Patients who met all the criteria were enrolled and given 200 mg theophylline twice daily for 4 weeks (a run-in period). The patients had been receiving different doses of theophylline, or none, before the run-in period. In those patients who had been receiving higher doses, the dose was reduced to 200 mg twice daily, as reported in previous studies, to prevent high serum concentrations (CitationKelly 1987; CitationBarnes 1997). None of the patients was treated with anti-histamines, anti-leukotrienes, cromolyn, β-blockers, ACE inhibitors, oral prednisolone, and/or LABAs during the study. Some of the patients had discontinued these medications at least 4 weeks before enrollment. Patients were excluded if they had experienced an exacerbation within 4 weeks before enrollment. The use of a short-acting β2-agonist or short-acting anticholinergic on demand was permitted.
Following a 4-week run-in period (the end of which was defined as the baseline), patients were randomized to two groups. In one group, 18 μg of tiotropium was added on once daily from 6:00 to 8:00 am (combination group), and the other continued with the theophylline alone (theophylline alone group) for 8 weeks (the end of the treatment period). Patients who developed emesis or anorexia associated with the theophylline were withdrawn from the study. Smoking status and participation in rehabilitation programs were not altered during the trial.
Physical examinations, spirometry, and blood testing, including the monitoring of plasma concentrations of theophylline and MRC scoring, were performed at screening and baseline, and after 4 and 8 weeks of treatment. Spirometry was performed at least three times between 11:00 am and noon, and the best dataset was accepted. On the basis of the results of a previous study, these values were regarded as the near-peak changes after tiotropium inhalation (CitationDisse et al 1999). Adverse events were evaluated during the study ().
Figure 1 Study design.
Data on exacerbations of COPD were also collected throughout the trial. Information on exacerbation was obtained by direct questioning of each patient. Exacerbation was defined in accordance with the description by CitationRodrignez-Roisin (2000).
Statistical analysis
The number of subjects completing the study to the stage of primary end-point (FEV1) testing was 61, the experiment had 90% validity at the 5% significance level in detecting differences between treatments, as reported in previous studies (CitationHirata et al 2003; CitationIchinose et al 2003).
Demographic data and MRC score were expressed as mean ± SD. Comparisons in the demographic characteristics of patients with COPD between the combination and theophylline alone groups were analyzed by Fisher’s exact test. All data on spirometry and the time course of percentage change in pulmonary function since the screening visit were expressed as means ± SEM. Mean percentage changes between baseline (end of the run-in period) and after 4 and 8 weeks of treatment (treatment period) in each group were calculated and then compared. The unpaired t-test was used for comparison between the two groups. Two-way ANOVA was used for comparison of the time course data of each group at the baseline and after 4 and 8 weeks of treatment. MRC scoring of the time course data of each group was performed by non-parametric two-way ANOVA corrected by post-testing. The relationship between the changes in each spirometric parameter and MRC score was tested by Spearman’s non-parametric correlation test. Data on the plasma concentration of theophylline were expressed as means ± SD and compared between the two groups by an unpaired t-test. Differences were considered statistically significant when the p value was less than 0.05.
Results
Patients
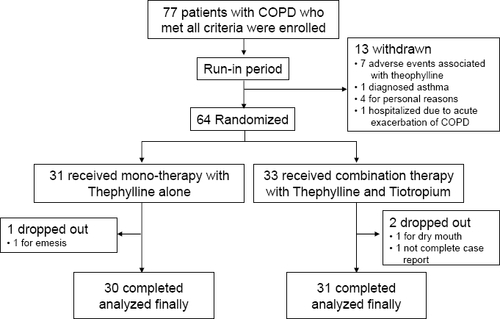
Demographic characteristics at the baseline are shown in . There was no significance difference in demographic characteristics between the two groups at the end of the run-in period. Seventy-seven COPD patients were matched to the entry criteria and enrolled in the study; they received theophylline (200 mg twice daily) for 4-weeks as a run-in period. During the run-in period, 13 patients were withdrawn from the study: 7 patients had adverse events associated with the theophylline (anorexia, 4; emesis, 1; ischuria, 1; and stomatitis, 1); 4 patients refused for personal reasons to continue; 1 patient had accompanying asthma, and one had an exacerbation of COPD. During the 8-week treatment period, two and one patient dropped out from the combination and theophylline alone groups, respectively. Finally, data on 61 COPD patients (31 combination; 30 theophylline alone) were used in the analysis (). No subject in either group experienced disease exacerbation from baseline to 8 weeks.
Table 1 Characteristics of patients with COPD at baseline
Figure 2 Trial profile.
Pulmonary function tests
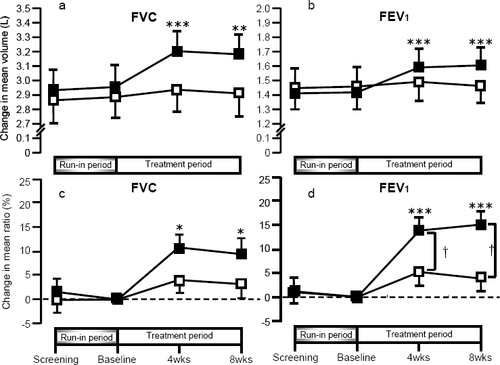
The FVC and FEV1 values in the combination therapy group were significantly increased 4 and 8 weeks after the addition of tiotropium, when compared with the baseline (). The increase in FEV1 from the baseline was 0.17 ± 0.03 L at 4 weeks and 0.21 ± 0.03 L at 8 weeks. In contrast, these effects were not observed in the theophylline-alone group. The percentage changes in FVC and FEV1 from the baseline were significantly increased at 4 and at 8 weeks in the combination therapy group, but not in the theophylline-alone group (). In addition, the percentage change in FEV1 in the combination therapy group was significantly greater than that in the theophylline-alone group.
Figure 3 Changes in FVC and FEV1 in the theophylline alone (white squares) and the combination therapy group (black squares). In a and b, absolute values of FVC and FEV1 are shown. In c and d, percentage changes in FVC and FEV1 from the baseline are shown.
Abbreviations: FVC, forced vital capacity; FEV1, forced expiratory volume in one second.
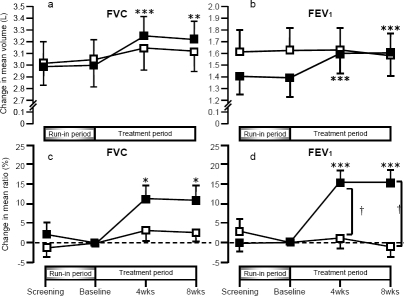
shows the results from 42 subjects from both groups who did not receive theophylline at screening (25 combination; 17 theophylline-alone). Theophylline-alone group did not cause a significant improvement in pulmonary function and symptoms over the 12 weeks (4-week run-in plus 8-week therapeutic period). However, in the combination therapy group, FVC and FEV1 were significantly increased after the addition of tiotropium.
Figure 4 Changes in FVC and FEV1 in the theophylline-alone (white squares, n = 17) and the combination therapy group (black squares, n = 25), in patients who did not receive regular treatment with theophylline at the time of screening. In a and b, absolute values of FVC and FEV1 are shown. In c and d, percentage changes in FVC and FEV1 from the baseline are shown.
Abbreviations: FVC, forced vital capacity; FEV1, forced expiratory volume in one second.
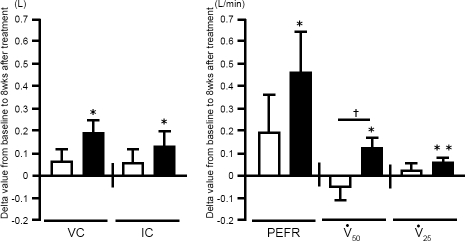
After 8 weeks of treatment, VC, inspiratory capacity (IC), peak expiratory flow rate (PEFR), ⩒50, and ⩒25 were significantly higher than the baseline values in the combination group. These effects were not observed in the theophylline-alone group ().
Figure 5 Changes in VC, IC, PEFR, ⩒50 and ⩒25 at 8 weeks. Changes in VC, IC, PEFR, ⩒50, and ⩒25 at 8 weeks were analyzed in theophylline-alone (white bars, n = 26) and combination therapy (solid bars, n = 30) groups.
Abbreviations: IC, inspiratory capacity; PEFR, peak expiratory flow rate; VC, vital capacity.
MRC score
MRC score was analyzed in 59 of 61 patients (two patients withdrew from the study at the stage of MRC scoring). MRC scores in the theophylline-alone group (n = 29) at screening, baseline, and 4 and 8 weeks after treatment were 2.00 ± 1.10, 1.75 ± 1.14, 2.04 ± 0.94, and 2.04 ± 1.21, respectively. The respective MRC scores in the combination group (n = 30) were 2.03 ± 1.10, 2.03 ± 1.19, 1.57 ± 1.14, and 1.57 ± 1.14. When compared with the baseline values, the mean MRC score in the combination group was significantly decreased by 0.46 (p < 0.01) and 0.46 (p < 0.05) at 4 and 8 weeks after treatment, respectively. The improvement was small but clinically meaningful, because the changes in MRC score were greater than those in a previous study (CitationAkamatsu et al 2007). In contrast, there was no significant change in the theophylline-alone group when compared with baseline. There was no significant difference in MRC score between the two groups at each time point ().
Figure 6 British Medical Research Council (MRC) scores 4 and 8 weeks after the addition of tiotropium. (a) MRC scores 4 and 8 weeks after the addition of tiotropium were analyzed in theophylline-alone (white bars, n = 29) and combination therapy (solid bars, n = 30) groups. (b) MRC scores 4 and 8 weeks after the addition of tiotropium were analyzed in 42 patients who were not receiving theophylline at the time of screening: theophylline-alone (white bars, n = 17) and combination therapy (solid bars, n = 25).
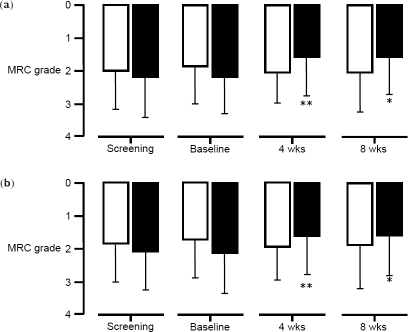
Next, we performed a sub-analysis of 42 of these 59 patients who were not receiving theophylline at screening to determine the therapeutic effects of theophylline itself. MRC scores at screening, baseline, and 4 and 8 weeks after treatment in the theophylline-alone group (n = 17) were 1.85 ± 1.14, 1.74 ± 1.15, 1.95 ± 1.03, and 1.88 ± 1.32, respectively. The respective MRC scores in the combination group (n = 25) were 2.08 ± 1.15, 2.12 ± 1.24, 1.60 ± 1.15, and 1.58 ± 1.21. When compared with the baseline values, the mean MRC score in the combination group was significantly decreased by 0.52 (p < 0.01) and 0.54 (p < 0.05) at 4 and 8 weeks, respectively, after treatment ().
Physical examination
No significant difference was observed between the two groups in terms of respiratory rates, blood pressure, heart rates, body temperature, and oxygen saturation of arterial blood by pulse oximeter at the screening visit, at the baseline, and after 4 and 8 weeks of treatment with tiotropium (data not shown).
Serum theophylline concentrations at the baseline and after 4 and 8 weeks of treatment were 8.6 ± 5.0, 8.9 ± 5.5, and 8.5 ± 4.7 μg/mL in the theophylline-alone group, and 9.5 ± 5.7, 9.4 ± 3.6, and 9.1 ± 4.9 μg/mL in the combination therapy group, respectively. There were no significant differences between the two groups at any time. Serum theophylline levels greater than 20 μg/mL were not observed in any patient.
Adverse events
During the run-in period, 7 patients dropped out because of theophylline-related adverse events, as described above. We observed 9 adverse events during the treatment period. Two and 7 adverse events were observed in the theophylline-alone group and the combination therapy group, respectively. In the theophylline-alone group, these events were anorexia (n = 1) and hematuria (n = 1). In the combination therapy group, they were dry mouth (n = 2), pharyngolaryngeal paresthesia (n = 3), fatigue (n = 1), and bitter taste (n = 1). One of the patients with emesis dropped out of the theophylline-alone group, and one with dry mouth and one with pharyngolaryngeal paresthesia dropped out of the combination therapy group.
Discussion
To our knowledge, this is the first study to show the efficacy and safety of tiotropium add-on therapy in COPD patients treated with theophylline. We demonstrated that add-on therapy with tiotropium significantly improved the MRC dyspnea score and pulmonary function in COPD patients already being treated with theophylline. According to the GOLD guidelines, combination therapy with different kinds of bronchodilators is recommended for COPD patients, because it can improve efficacy without increasing the risk of side effects, as compared with increasing the dose of monotherapy (CitationGold 2006).
Previous studies have reported that treatment with relatively low dose of theophylline has anti-inflammatory effects in COPD patients (CitationCulpitt et al 2002; CitationKobayashi et al 2004; CitationHirano et al 2006). These patients were treated with theophylline at 400 mg/day, and/or plasma levels of theophylline were approximately 5 to 10 mg/L. These concentrations of theophylline had anti-inflammatory effects. However, these studies did not determine whether theophylline had clinical benefits on pulmonary function or physical condition in COPD patients. The Japanese Respiratory Society’s guidelines for the diagnosis and treatment of COPD suggested that low dose of theophylline may be effective for COPD patients, as high doses of theophylline have toxic effects (CitationGuidelines for the Diagnosis and Treatment of COPD 2006). On the basis of these studies, we treated COPD patients with 400 mg theophylline (200 mg twice daily). Plasma levels of theophylline were approximately 8 to 10 mg/L in these patients, and theophylline alone did not improve pulmonary function (FEV1) or MRC scores in 30 COPD patients analyzed. Moreover, in 17 patients who were not receiving theophylline at screening, treatment with theophylline alone did not improve MRC score or FEV1. The possibility remains that this concentration of theophylline in the plasma may not exert sufficient bronchodilatation (CitationMitenko and Ogilvie 1973). Here we evaluated whether the combination of theophylline and tiotropium could improve FEV1 and MRC scores in COPD patients, and we compared our results with those of previous studies in Japan (CitationHirata et al 2003; CitationIchinose et al 2003).
A study that compared the effects of the short-acting anticholinergic ipratropium and theophylline reported that improvement of pulmonary function and exercise endurance was significantly greater in the combination therapy group than in each monotherapy group (CitationTsukino et al 1998). In addition, a combination of the short-acting anti-cholinergic oxitropium and theophylline improved QOL to a significantly greater extent than did each monotherapy (CitationBellia et al 2002). Furthermore, combination treatment with a short-acting β2-agonist, a short-acting anticholinergic agent, and oral theophylline led to significantly greater improvement in FEV1 compared with the results of monotherapy, without any severe adverse effects (CitationKarpel et al 1994).
Long-acting bronchodilators have recently become standard medicines in the pharmacological treatment of COPD (CitationGold 2006). Therefore, the establishment of combination therapy for COPD with long-acting bronchodilators is an expected trend. Combination of the LABA salmeterol with theophylline leads to significantly better pulmonary functions, greater improvement in symptoms, improved reduction in the use of short-acting β2-agonists, and decrease in exacerbation frequency compared with the use of theophylline alone (CitationZuwallack et al 2001). In both stable COPD patients and those with exacerbations, combination therapy with the inhaled LABA formoterol and the inhaled long-acting anticholinergic tiotropium improves pulmonary function indicators such as FEV1, IC, and FVC to a significantly greater extent than is seen with each agent alone (CitationDi Marco et al 2006; CitationVan Noord et al 2006). A previous study also showed additional clinical improvement when COPD patients were treated with theophylline added to salmeterol (CitationZuwallack et al 2001). However, evidence of the effects of combination therapy with long-acting bronchodilators, especially anticholinergics and theophylline, is still scant.
One recent study reported the effect of combination therapy with tiotropium and theophylline (CitationCazzola and Gabriella Matera 2007). They investigated the additive effect of theophylline in patients with stable COPD who were receiving both tiotropium and formoterol. Although their findings question the importance of adding theophylline in stable COPD patients already being treated with two long-acting bronchodilators, they also indicate that some patients may benefit from theophylline because of symptomatic improvement. We chose to investigate the effects of adding tiotropium in patients already treated with theophylline because theophylline is widely used for COPD treatment, both in Japan and worldwide (CitationIchinose et al 2006).
Dyspnea upon exercise is one of the most important symptoms in patients with COPD. We used the MRC dyspnea score to assess symptoms: the MRC questionnaire can easily classify symptom severity. We demonstrated that the mean MRC dyspnea score in patients with combination therapy improved significantly after both 4 and 8 weeks of tiotropium add-on therapy.
The beneficial effect of combination therapy might be attributable to the different mechanisms of bronchodilation (CitationThirstrup 2000). Theophylline had been reported to have extrapulmonary effects, such as increased diaphragmatic contractility and reversed diaphragm fatigue, although the validity of these effects remains controversial (CitationAubier et al 1981). There is also increasing evidence that low-dose theophylline has anti-inflammatory effects in asthma and COPD (CitationCulpitt et al 2002; CitationCosio et al 2004; CitationBarnes et al 2005).
The effects of treatment with tiotropium alone on pulmonary function, when compared with placebo, include improvements in peak expiratory flow volume, FEV1, FVC, VC, and IC (CitationCasaburi et al 2002; CitationVincken et al 2002; CitationBrusasco et al 2003; CitationCelli et al 2003; CitationO’Donnell et al 2004; CitationVan Noord et al 2006). Our findings confirmed these previous observations. In the study of Japanese COPD patients, the increase in peak FEV1 with tiotropium alone was 0.20 ± 0.02 L after 6 months of treatment (CitationHirata et al 2003; CitationIchinose et al 2003). In our patients, addition of tiotropium to theophylline increased the mean FEV1 by 0.17 ± 0.03 L and 0.21 ± 0.03 L after 4 and 8 weeks, respectively. These increases in FEV1 were similar to those in other investigations (CitationHirata et al 2003; CitationIchinose et al 2003). Our present study did not include a group of patients treated with tiotropium alone, so we were unable to assess whether there was any benefit of adding theophylline to patients treated with tiotropium. The above-mentioned recent study in which the add-on effect of theophylline was investigated in patients already being treated with tiotropium and formoterol reported a limited effect of theophylline add-on (CitationCazzola and Gabriella Matera 2007). Evaluation of all of these results together indicates that tiotropium is a useful addition in COPD patients already treated with theophylline.
*Appendix
The Kurume COPD Study Group includes Dr Toshinobu Yokoyama and Dr Tomoko Kamimura, (Kurume University); Dr Kazuhito Taguchi, (National Hospital Organization Kyushu Medical Center); Dr Rumi Gohara and Dr Yoshikazu Tominaga (Yame General Hospital); Dr Toru Rikimaru and Dr Mamoru Nishiyama (Saiseikai Futsukaichi Hospital); Dr Koichi Azuma (Social Insurance Tagawa Hospital); Dr Kazuko Matsunaga (National Hospital Organization Omuta Hospital); and Dr Hideyuki Koga (Keisinkai Hospital).
Acknowledgements
We especially thank Dr Gail M Gauvreau of the Asthma Research Group, McMaster University, Canada, for critical reading of this manuscript. This work was supported by Nippon Boehringer Ingelheim Co, Ltd (Tokyo, Japan) and by a Grant-in-Aid for Scientific Research (B) (no. 18390244) and Grants-in-Aid for Scientific Research (B) (no. 17390244) and Exploratory Research (no. 18659244) from the Ministry of Education, Science, Sports, and Culture of Japan.
References
- AkamatsuKYamagataTTakahashiTImprovement of pulmonary function and dyspnea by tiotropium in COPD patients using a transdermal beta(2)-agonistPulm Pharmacol Ther200720701717049894
- AnzuetoATashkinDMenjogeSOne-year analysis of longitudinal changes in spirometry in patients with COPD receiving tiotropiumPulm Pharmacol Ther200518758115649848
- AubierMDe TroyerASampsonMAminophylline improves diaphragmatic contractilityN Engl J Med1981305249527242614
- BarnesPJCurrent therapies for asthma. Promise and limitationsChest199711117S26S9042023
- BarnesPJAdcockIMItoKHistone acetylation and deacetylation: importance in inflammatory lung diseasesEur Respir J2005255526315738302
- BelliaVForesiABiancoSEfficacy and safety of oxitropium bromide, theophylline and their combination in COPD patients: a double-blind, randomized, multicentre study (BREATH Trial)Respir Med200296881912418585
- BrusascoVHodderRMiravitllesMHealth outcomes following treatment for six months with once daily tiotropium compared with twice daily salmeterol in patients with COPDThorax20035839940412728159
- CasaburiRMahlerDAJonesPWA long-term evaluation of once-daily inhaled tiotropium in chronic obstructive pulmonary diseaseEur Respir J2002192172411866001
- CazzolaMGabriella MateraMThe additive effect of theophylline on a combination of formoterol and tiotropium in stable COPD: a pilot studyRespir Med20071019576217056241
- CelliBZuWallackRWangSImprovement in resting inspiratory capacity and hyperinflation with tiotropium in COPD patients with increased static lung volumesChest20031241743814605043
- CosioBGTsaprouniLItoKTheophylline restores histone deacetylase activity and steroid responses in COPD macrophagesJ Exp Med20042006899515337792
- CulpittSVde MatosCRussellREEffect of theophylline on induced sputum inflammatory indices and neutrophil chemotaxis in chronic obstructive pulmonary diseaseAm J Respir Crit Care Med20021651371612016098
- Di MarcoFVergaMSantusPEffect of formoterol, tiotropium, and their combination in patients with acute exacerbation of chronic obstructive pulmonary disease: a pilot studyRespir Med200610019253216626956
- DisseBSpeckGARomingerKLTiotropium (Spiriva): mechanistical considerations and clinical profile in obstructive lung diseaseLife Sci1999644576410069510
- DonohueJFCombination therapy for chronic obstructive pulmonary disease: clinical aspectsProc Am Thorac Soc2005227281 discussion: 90–116267348
- DusserDBravoMLIaconoPThe effect of tiotropium on exacerbations and airflow in patients with COPDEur Respir J2006275475516507855
- [GOLD] Global Initiative for Chronic Obstructive Lung DiseaseGlobal strategy for the diagnosis, management and prevention of chronic obstructive pulmonary diseaseNHLBI/WHO workshop report2006BethesdaNational Heart, Lung and Blood Institute online Accessed 11 November 2006. URL: http://www.goldcopd.com
- Guidelines for the diagnosis and treatment of COPDGuidelines for the diagnosis and treatment of COPDCommittee for the second edition of the COPD guidelines of the Japanese Respiratory Society20062 online URL: http://www.jrs.or.jp/quicklink/glsm/guideline/nopass_pdf/copd_summary_e.pdf
- GuyattGhTownsendMPugsleySoBronchodilators in chronic air-flow limitation. Effects on airway function, exercise capacity, and quality of lifeAm Rev Respir Dis19871351069743579005
- HiranoTYamagataTGohdaMInhibition of reactive nitrogen species production in COPD airways: comparison of inhaled corticosteroid and oral theophyllineThorax200661761616936236
- HirataKNishimuraMIchinoseMTiotropium once daily improves health status in Japanese patients with COPDAm J Respir Crit Care Med2003167A94
- IchinoseMNishimuraMHirataKTiotropium once daily improves spirometry over 24 hours in Japanese patients with COPDAm J Respir Crit Care Med2003167A95
- IchinoseMFukuchiYNagaiALarge-scale telephone survey on burden of patients with chronic obstructive pulmonary disease (COPD) in Japan: confronting COPDRespirology200611A154
- ItoKLimSCaramoriGA molecular mechanism of action of theophylline: Induction of histone deacetylase activity to decrease inflammatory gene expressionProc Natl Acad Sci USA2002998921612070353
- JacksonRHMcHenryJIMorelandFBClinical evaluation of elixophyllin with correlation of pulmonary function studies and theophylline serum levels in acute and chronic asthmatic patientsDis Chest196445758514114639
- KarpelJPKotchAZinnyMA comparison of inhaled ipratropium, oral theophylline plus inhaled beta-agonist, and the combination of all three in patients with COPDChest19941051089948162730
- KellyHWJenneJWMurphySDekkerMTheophylline toxicityDrug therapy for asthma1987New York92551
- KobayashiMNasuharaYBetsuyakuTEffect of low-dose theophylline on airway inflammation in COPDRespirology200492495415182277
- MitenkoPAOgilvieRIRational intravenous doses of theophyllineN Engl J Med197328960034723589
- Moor-JankowskiJPrimate animals for biomedical research evaluation by the British Medical Research Council Laboratory Animal Centre. A critical reviewJ Med Primatol1976536571828933
- MurcianoDAuclairMHParienteRA randomized, controlled trial of theophylline in patients with severe chronic obstructive pulmonary diseaseN Engl J Med1989320152152498658
- NiewoehnerDERiceKCoteCPrevention of exacerbations of chronic obstructive pulmonary disease with tiotropium, a once-daily inhaled anticholinergic bronchodilator: a randomized trialAnn Intern Med20051433172616144890
- O’DonnellDEFlugeTGerkenFEffects of tiotropium on lung hyperinflation, dyspnoea and exercise tolerance in COPDEur Respir J2004238324015218994
- Rodriguez-RoisinRToward a consensus definition for COPD exacerbationsChest2000117398S401S10843984
- SullivanPBekirSJaffarZAnti-inflammatory effects of low-dose oral theophylline in atopic asthmaLancet1994343100687909049
- ThirstrupSControl of airway smooth muscle tone: II-pharmacology of relaxationRespir Med2000945192810921754
- TsukinoMNishimuraKIkedaAEffects of theophylline and ipratropium bromide on exercise performance in patients with stable chronic obstructive pulmonary diseaseThorax199853269739741369
- Turner-WarwickMStudy of theophylline plasma levels after oral administration of new theophylline compoundsBr Med J1957267913436856
- van NoordJAAumannJLJanssensEEffects of tiotropium with and without formoterol on airflow obstruction and resting hyperinflation in patients with COPDChest20061295091716537846
- VinckenWvan NoordJAGreefhorstAPImproved health outcomes in patients with COPD during 1 yr’s treatment with tiotropiumEur Respir J2002192091611871363
- ZuWallackRLMahlerDAReillyDSalmeterol plus theophylline combination therapy in the treatment of COPDChest200111916617011399688