Abstract
Chronic obstructive pulmonary disease (COPD) is an epidemic in many parts of the world. Most patients with COPD demonstrate mild disease. The cornerstone of management of mild disease is smoking cessation, which is the only proven intervention to relieve symptoms, modify its natural history and reduce mortality. For asymptomatic patients, it is the only required therapy. Short-acting bronchodilators can be added on an as needed basis for those with intermittent symptoms and regularly for those with persistent symptoms. Long-acting bronchodilators can be substituted for those who remain symptomatic despite regular use of short-acting bronchodilators. Inhaled corticosteroids do not modify the natural history of COPD and as such cannot be recommended as standalone therapy for mild COPD. However, for patients with refractory and intractable symptoms, they may be used in combination with long-acting beta-2 agonists. Influenza and pneumococcal vaccination and pulmonary rehabilitation are other therapies that may be considered for select patients with mild disease. In this paper, we summarize the current standard of care for patients with mild COPD.
Keywords:
Introduction
Chronic obstructive pulmonary disease (COPD) is an inflammatory disorder of the lung that is characterized by irreversible or partially reversible airflow limitation (CitationRabe et al 2007). It is highly prevalent affecting 600 million people worldwide and accounting for nearly 4 million deaths annually (CitationMurray and Lopez 1997b). Over the next 20 years, the burden of COPD is expected to increase, making it the third leading cause of mortality worldwide (currently fourth) (CitationMurray and Lopez 1997a). COPD is a relentless and progressive disease, caused by a complex interaction between genes and environment. Although cigarette smoking is the single most important risk factor, smokers constitute only ~50% of the worldwide cases of COPD; the rest occur in life-time never smokers (CitationMannino and Buist 2007). Furthermore, once COPD develops, smoking cessation does not abrogate the increased risk of morbidity and mortality (though the risk is smaller than when they were actively smoking) (CitationAnthonisen et al 2005; CitationPelkonen et al 2000; CitationSin et al 2005b) and smoking cessation does not halt the underlying inflammatory process in the lungs of COPD patients (CitationWillemse et al 2005). Other known risk factors for COPD include airway hyperresponsiveness, genetic abnormalities such as alpha-1-antitrypsin deficiency, air pollution, biomass smoke exposure, occupational dusts and chemicals, respiratory infections especially during childhood, and poor nutrition (CitationChapman et al 2006). Unfortunately, there is a dearth of therapies that can effectively modify disease activity or progression. The current treatment is largely aimed at relieving patient symptoms and reducing long-term complications (CitationSin et al 2003) and is modified by disease severity (CitationRabe et al 2007). The management algorithms for moderate to severe COPD have been reviewed expertly elsewhere (CitationSin et al 2003; CitationWilt et al 2007). In this paper, we will review the management goals and strategies for patients with mild COPD.
Definition of mild COPD
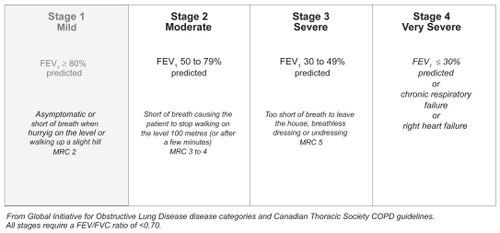
COPD is diagnosed clinically based on history and physical examination, complemented by spirometric data demonstrating irreversible or poorly reversible airflow obstruction in the absence of an alternate diagnosis such as congestive heart failure, neuromuscular disease or asthma (CitationMan et al 2003). Most but not all patients with COPD are either current or ex-smokers with at least 10 pack-year smoking history (pack-years is calculated by multiplying the number of cigarettes smoked per day by the years smoked divided by 20). The most common presenting symptom is dyspnea with exertion or chronic cough with or without sputum production. Other (but more infrequent) symptoms include chest pain, orthopnea and wheezing. However, there is also a group of patients with abnormal spirometry but are otherwise asymptomatic. The physical examination is completely unremarkable in most patients with mild COPD. In some cases, however, patients may demonstrate a positive cough test (which is defined as recurrent coughing after patients take a deep breath to maximal lung capacity and coughs more than once), and have a forced expiratory time at the bedside of 9 seconds or greater (CitationStraus et al 2000). On spirometry, patients with COPD demonstrate a forced expiratory volume in one second (FEV1) to forced vital capacity (FVC) ratio of less than 0.70 following receipt of a bronchodilator (eg, albuterol 200–400 μg) (CitationO’Donnell et al 2007; CitationRabe et al 2007). Once the diagnosis of COPD is made, severity is assessed using the post-bronchodilator FEV1 value. An example of the severity classification scheme is shown in (CitationO’Donnell et al 2007). Mild COPD is defined by a post-bronchodilator FEV1 that is 80% of predicted or greater in the presence of an FEV1/FVC ratio of less than 70% and characteristic symptoms such as exertional dyspnea in most cases (CitationCelli and MacNee 2004; CitationRabe et al 2007). However, some who meet the spirometric criteria of mild COPD may be asymptomatic. In one study of patients who were seen at a primary care office, over a third of ex- and current smokers who were diagnosed with mild COPD based on screening spirometry were asymptomatic at the time of testing, while 2/3 of never smokers diagnosed with mild COPD were asymptomatic (CitationBednarek et al 2008). Thus, the prevalence of COPD based on physician or self-diagnosis likely under-estimates the prevalence of COPD based on spirometry (CitationBuist et al 2007). A more liberal use of spirometry in primary care may increase the detection and diagnosis of COPD in the community.
Figure 1 COPD Severity Classification Scheme Copyright © 2007. Reproduced with permission from CitationO’Donnell DE, Aaron S, Bourbeau J, et al 2007. Canadian Thoracic Society recommendations for management of chronic obstructive pulmonary disease – 2007 update. Can Respir J, 14(Suppl B):5B–32B.
Treatment goals
Although patients with mild COPD are at increased risk of respiratory infections and respiratory failure, COPD-related hospitalizations and deaths are relatively infrequent in this group of patients (CitationAnthonisen et al 1994). Thus, dissimilar to those with more severe disease, prevention of respiratory complications such as exacerbations and respiratory mortality is not the primary goal in the treatment of mild COPD. Instead, treatment goals are focused on the following 3 domains: 1) relieving patient symptoms; 2) slowing the progression of disease; and 3) mitigating the risk for cardiovascular disease (CVD) and lung cancer, which are the leading causes of hospitalization and mortality in patients with mild COPD (CitationAnthonisen et al 1994).
Treatment goal 1: relief of patient symptoms
The most common symptom in mild COPD is exertional dyspnea with or without chronic cough. In assessing these symptoms, physicians must rule out all other causes of dyspnea including cardiovascular de-conditioning, neuromuscular disease, interstitial lung disease, ischemic heart disease, congestive heart failure, pulmonary embolism, anemia and pulmonary hypertension. A careful history and physical examination, accompanied by simple laboratory tests such as pulse oximetry, chest radiograph, electrocardiogram, complete blood count and spirometry are usually sufficient in excluding other common causes of dyspnea. In a minority of cases, additional tests including incremental cardiopulmonary exercise testing, echocardiogram and computed tomography (CT) may be necessary. Once all causes of dyspnea have been ruled out and COPD is confirmed by spirometry, management can be initiated.
Smoking cessation
Symptomatic treatment starts with smoking cessation for smokers with mild COPD. In a dose dependent manner, smoking induces cough and dyspnea and smoking cessation attenuates these symptoms (CitationStein et al 2005). Although the prevalence of smoking has declined over the past two decades in the US and other industrialized nations, 20% of adults in the western world continue to smoke. In the developing world, smoking rates are increasing with nearly 40% of adults smoking on a daily basis in certain jurisdictions (CitationEzzati and Lopez 2003). Although clinicians should encourage patients to stop smoking and provide practical advices in their clinic, these measures are generally ineffective, leading to smoking cessation in only about 5% of smokers (CitationBailey 1985). This intervention, however, is more effective when offered at the time the diagnosis of COPD is made (CitationStratelis et al 2006). Another way to increase cessation rate is to convey the concept of “lung age” to the patients. Lung age is defined as the age of the average person who has the same FEV1 as that of the patient and can be calculated using the formula: lung age (for men) = 2.87 × height (in inches) −31.25 × observed FEV1 (liters) − 39.375 and lung age (for women) = age = 3.56 × height (in inches) − 40 × observed FEV1 (liters) − 77.28 (CitationMorris and Temple 1985). In the largest randomized trial of its kind, Parkes et al showed that smokers who received information regarding their “lung age” were twice as more likely to quit than smokers who received their raw FEV1 data (CitationParkes et al 2008). At 12 months of follow-up, the cessation rate was 14% in the lung age group versus 6% in the control group.
Comprehensive smoking cessation clinics consisting of physician services, cognitive and behavioral modification programs, and nicotine replacement therapy achieve the best results (CitationSchroeder 2005). Cognitive programs employ techniques such as distraction, positivism, relaxation, and mental imagery to modify patient’s attitude towards smoking (CitationSchroeder 2005). Behavioral interventions, on the other hand, focus on breaking the smoking habit by avoiding smoking triggers such as drinking coffee or alcohol or associating with friends who smoke. Collectively, these methods are effective in fostering quitting in about 10% to 15% of motivated smokers (CitationKanner et al 1999).
One of the cornerstones in smoking cessation is the use of nicotine replacement therapy (NRT). NRT has been expertly reviewed elsewhere (CitationMolyneux 2004). The major goals of NRT are to 1) attenuate withdrawal symptoms, 2) eliminate craving; and 3) make smoking less rewarding. NRT generally doubles the cessation rate compared to physician advice alone (CitationMolyneux 2004). High doses of NRT are more effective than lower doses but are fraught with more side effects (CitationSchroeder 2005). However, for those patients refractory to the lower doses, higher doses should be considered. Side effects include insomnia, skin irritation (for patches), and early morning cravings for nicotine. There are 6 ways in which NRT can be administered: as a patch, gum, sublingual tablet, lozenge, nasal spray, or inhaler. The patches are the most common mode of delivery and are found in 16-hour (5, 10, 15 mg) or 24-hour (7, 14, 21 mg) formulations. The gums are also frequently used and they are packaged in 2- or 4-mg pieces.
Non-nicotine based pharmacologic therapies are also available and are as effective as NRT in fostering smoking cessation. Anti-depressants and in particular bupropion significantly enhance cessation rates. Similar to NRTs, bupropion and nortryptylline double the quitting rates compared with advice alone (CitationHughes et al 2007). Bupropion should be prescribed at least 1 week before the cessation date, so that adequate blood levels can be achieved and continued for 2 to 3 months following cessation. There is insufficient evidence to determine whether or not anti-depressants provide incremental benefits on cessation beyond that achieved by NRT alone. Serious side effects from anti-depressants are relatively uncommon. The risk of seizures is about 0.1% with the use of bupropion (CitationHughes et al 2007). Thus, bupropion should be avoided in patients with a seizure disorder (CitationSchroeder 2005). Although there are ongoing concerns regarding the possible increased risk of suicides among those who take bupropion, there is insufficient body of evidence to support this notion.
More recently α4β2 nicotinic acetylcholine receptor agonists (eg, varenicline) have been introduced into the market for smoking cessation (CitationGonzales et al 2006). Varenicline is a partial α4β2 nicotinic receptor agonist. It is approximately three times more effective in effecting smoking cessation than is placebo (CitationCahill et al 2007). It should be started at 0.5 mg daily while the patient is still smoking and then escalated to 1 mg per day by the second week. The patient should quit smoking completely by week 2 and the drug should be continued for another 12 weeks. The most common side effect of this drug is nausea, which can be mitigated by taking the drug following meals. Varenicline appears to be more effective than bupropion (odds ratio for smoking cessation, 1.66) (CitationCahill et al 2007). However, it should be used with extreme caution (if at all) in patients with a past history of severe depression or a psychosis as it has been rarely associated with major psychiatric adverse effects (CitationPumariega et al 2008).
Bronchodilators
For those who remain symptomatic despite smoking cessation, bronchodilators may be used to improve patient symptoms. If the symptoms are periodic, short-acting bronchodilators (eg, beta-2 agonists or anticholinergics) can be used on an as-needed basis. For those with persistent symptoms, short-acting bronchodilators may be used regularly (eg, 4 times a day) or, alternatively, long-acting bronchodilators may be used instead. All bronchodilators work by increasing expiratory flow, reducing dynamic hyperinflation and improving exercise capacity and quality of life of patients (CitationHanania and Donohue 2007). However, the improvement in symptoms and exercise capacity is not readily predictable from the spirometric response to bronchodilators. There are two major classes of bronchodilators: β2-agonists and anti-cholinergic agents.
β2-agonists
All β2-agonists act by binding to and stimulating cell surface β2-adrenoceptors, which belong to a seven transmembrane G-protein coupled receptor family. Upon ligand binding, the α-component of the G-protein dissociates and activates adenylate cyclase (CitationJohnson 1998), which in turn stimulates the production of cyclic adenosine monophosphate, and activates protein kinase A (PKA). PKA then phosphorylates a number of intracellular regulatory proteins (CitationJohnson 1998). Stimulation of the β2- adrenoreceptors can also inhibit histamine and cysteinyl-leukotriene release from mast cells, prevent plasma exudation from postcapillary venules, and modulate sensory neural outputs in the airways (CitationJohnson 1998). Thus, in addition their bronchodilatory properties, β2-agonists may have anti-inflammatory effects.
There are two major categories of β2-agonists: short acting β2-agonists (SABA) and long-acting β2-agonists (LABA). SABAs have a rapid onset of action (1–3 minutes) and their pharmacologic effects last less than six hours (CitationRabe et al 2007). Thus, they provide quick relief of dyspnea and are best used as rescue medications for patients with intermittent symptoms. In patients with persistent symptoms, regular use of SABAs (usually four times a day) either alone or in combination (of β2-agonist and anticholinergic) is recommended. Of the SABAs, salbutamol (albuterol) is the most commonly used agent and can be delivered via a metered dose inhaler or a nebulizer. For patients with mild COPD who have symptoms refractory to SABAs, LABAs may be considered. The two most commonly used LABAs in clinical practice are salmeterol and formoterol. Both of these compounds have high affinity for β2-adrenoreceptors. Salmeterol is considered a partial agonist because the ligand-receptor coupling is incomplete. In contrast, formoterol binds completely to the β2-adrenoreceptor, making it a full agonist. Salmeterol binds to β2-adrenoreceptor in airway smooth muscle with an efficacy of 65% compared to formoterol (CitationBall et al 1991). Despite these differences, clinically, they appear to have similar effectiveness. On average, formoterol provides faster relief of symptoms than does salmeterol but salmeterol may provide longer duration of relief (CitationJohnson, 1998). Although some safety concerns have been raised regarding their use in asthma (CitationMartinez 2005; CitationSalpeter et al 2006), LABAs appear to be safe in COPD (CitationCalverley et al 2007).
Anticholinergics
Anticholinergic agents, on the other hand, reduce airway tone by blocking the muscarinic receptors that induce bronchial smooth muscle contraction. Ipratropium bromide is the prototypical short acting anticholinergic agent, which has a half-life of less than 6 hours (CitationRabe et al 2007). Tiotropium is a longer acting anticholinergic agent that is approximately 10-fold more potent than ipratropium bromide. This is because tiotropium dissociates very slowly from lung muscarinic receptors and in airway smooth muscles demonstrates partial selectivity for the M3-receptors. Clinically, tiotropium provides bronchodilation for greater than 24 hours and thus is suitable for once-daily dosing (CitationBarnes et al 1995).
Tiotropium has been largely tested in patients with moderate to severe disease. Clearly, in moderate to severe disease, tiotropium reduces patient symptoms, improves health-related quality of life, reduces exacerbations (CitationBarr et al 2006), decreases dynamic hyperinflation of the lungs (CitationMaltais et al 2005) and increases exercise tolerance (CitationCasaburi et al 2005). However, there is little information on the effectiveness of tiotropium in patients with mild disease. In one 12-week randomized controlled trial (N = 224; mean FEV1, 74% of predicted), patients with mild COPD who received tiotropium experienced a 118 mL improvement FEV1 and required fewer daily doses of a short-acting in β2-agonists compared to those who received placebo (CitationJohansson et al 2008). However, symptom and quality of life scores were no different between the two groups.
Similarly, there is a large body of evidence indicating that LABA is effective in relieving symptoms and improving health status in patients with moderate to severe COPD (CitationCalverley et al 2007; CitationSin et al 2003). However, as with tiotropium, there is a marked scarcity of information regarding their effectiveness in mild COPD. In general, while they improve lung function, they do not appear to have a major impact on patient symptoms or quality of life in mild COPD (CitationAppleton et al 2006). Thus, LABAs cannot be recommended routinely for mild COPD except in patients who have persistent symptoms despite SABAs or in those who have frequent exacerbations requiring systemic corticosteroid therapy and/or hospital visits.
Inhaled glucocorticoids
Inhaled glucocorticoids have been used for COPD over the past 3 decades. Nevertheless, their exact role in COPD management remains uncertain. In the 1990s, several large-scale randomized controlled trials were conducted to clearly define the benefits and the hazards of inhaled corticosteroids in the treatment of COPD. All of these studies were powered to determine whether or not inhaled corticosteroids modified the rate of decline in FEV1. However, several studies also captured the effects of these drugs on patient symptoms. In one of the largest study of its kind, the Lung Health Study (LHS)-2 evaluated the effects of inhaled triamcinolone on symptoms in patients with mild to moderate COPD (mean FEV1, 68% of predicted) (CitationLung Health Study Group, 2000). On average, the subjects were followed for 40 months. Triamcinolone had no significant effect on cough and sputum production (p = 0.26) but a significant impact in reducing dyspnea (p = 0.02). Sixty-eight percent of patients in the triamcinolone arm did not complain of dyspnea by the end of the study, while 62% did not have dyspnea in the placebo arm (a difference of 6.7%). Importantly, compared with placebo, there was a 29% relative reduction in the number of patients who complained of difficulty breathing (p = 0.05), and a 35% relative reduction in the number of patients with wheezing in the group that took triamcinolone (CitationLung Health Study Group, 2000). In the Copenhagen City Heart Study (mean FEV1, 87% of predicted), similar to LHS-2, inhaled budesonide did not have a significant impact on cough and sputum production (CitationVestbo et al 1999). Collectively, these data suggest that inhaled corticosteroids probably do not have any significant effect on cough and sputum production; they appear to have a modest effect in reducing dyspnea. However, in view of the long-term safety concerns associated with inhaled corticosteroids including bone demineralization and skin bruising, they cannot be routinely recommended in patients with mild COPD. Inhaled corticosteroids may be considered for patients with dyspnea refractory to smoking cessation and bronchodilators.
Pulmonary rehabilitation
In COPD, patients experience dyspnea and exercise limitation because of impaired gas exchange, increased dead space ventilation and dynamic hyperinflation (CitationOfir et al 2008). Additional demands are placed on the respiratory system by physical deconditioning and peripheral muscle dysfunction. Exercise training programs in COPD have the goal of improving cardiovascular fitness, increasing aerobic capacity of muscles and decreasing symptoms. Pulmonary rehabilitation programs have also been shown to decrease the number of exacerbations and shorten the length of hospital stay during an exacerbation (CitationHunter and King 2001; CitationNici et al 2006). Although most of these studies were conducted in patients with moderate to severe disease, several studies were evaluated patients with mild COPD (CitationBianchi et al 2002; CitationClark et al 2000; CitationDourado et al 2006; CitationGarrod et al 2004; CitationKamahara et al 2004; CitationKarapolat et al 2007; CitationRossi et al 2005). Clinical outcomes were measured by activity endurance (6 minute walk test) as well as with a quality of life instrument such as the St Georges Respiratory Questionnaire (SGRQ). One study found that muscle function and oxygen utilization (VO2max, VTmax, paired t-test) improved after a 12-week rehabilitation program involving isokinetic strength training (CitationClark et al 2000), while another showed improved exercise endurance with pulmonary rehabilitation (R2 = 0.146) (CitationEakin et al 1992). However, the beneficial effects of pulmonary rehabilitation appear to be time-limited and wears off over time unless the exercise program is continued (CitationKarapolat et al 2007). Additionally, pulmonary rehabilitation programs that are longer in duration appear to be superior to short programs. One study found that a 20-session course led to improved 6 minute walk distance and better quality life compared with a 10-session course. Thus, pulmonary rehabilitation program should be considered for patients with mild COPD, who are symptomatic and are experiencing limitations in activity endurance and reduced quality of life.
Independent of symptoms all patients should be encouraged to exercise regularly (low to moderate intensity exercise for 30 minutes greater, at least 3 to 4 times per week) as regular physical activity independent of other factors is associated with slower progression of disease (CitationGarcia-Aymerich et al 2007). Additionally, patients should receive dietary counseling to ensure that adequate amount of calories are consumed each day and the diet is enriched for fruits, vegetables and fish, which may decrease COPD progression (CitationVarraso et al 2007).
Treatment goal 2: slow the progression of disease
Smoking cessation
The most commonly used metric for measuring disease progression in COPD is the rate of decline in lung function, as assessed by FEV1. Due to the intrinsic variability of the measurement, at least 3 FEV1 values measured over 3 years are needed to adequately assess progression. It is well known that smoking accelerates the decline in FEV1, while smoking cessation normalizes the rate of decline. In the Lung Health Study, which evaluated 5,800 smokers with mild to moderate COPD, smokers who continued to smoke lost on average 60 mL/year in FEV1 over a 5 year follow-up period. In contrast, sustained quitters lost 14 ml/year in FEV1 (CitationAnthonisen et al 1994). Over 11 years of follow-up, sustained quitters lost 26 to 30 mL/year (or 0.23% to 0.40% of predicted/year) in FEV1, whereas intermittent quitters lost 48 to 50 mL/year (or 0.91% to 1.02% of predicted/year) and continued smokers lost 60 to 64 mL/year (or 1.29 to 1.44% of predicted/year) in FEV1 (CitationAnthonisen et al 2002). Smoking cessation is the only proven method of retarding disease progression in COPD.
Inhaled glucocorticoids
In the 1990s, there was renewed enthusiasm for using inhaled corticosteroids to modify the natural history of COPD (CitationSin et al 2005a). Several long-term randomized controlled trials were performed in mostly mild to moderate COPD subjects. Collectively, these trials indicated that within the first 6 months of therapy, inhaled corticosteroids increased FEV1 compared to placebo. The effect was most pronounced in female non-smokers. However, they did not modify the long-term decline in FEV1 (CitationSoriano et al 2007).
Combination of inhaled glucocorticoids and LABAs
In moderate to severe COPD, LABAs and inhaled corticosteroids either by themselves or in combination have a modest effect on disease progression. In the TORCH (TOwards a Revolution in COPD Health) Study, which evaluated these medications in moderate to severe COPD, patients who received inhaled fluticasone or salmeterol experienced a slower decline in FEV1 (by 13 mL/year) compared to those who received placebo (CitationCalverley et al 2007). Patients who received a combination of fluticasone and salmeterol demonstrated the slowest decline (by 16 mL/year). The effects of tiotropium on disease progression have been assessed in the UPLIFT trial (Understanding the Potential Long-Term Impacts on Function with Tiotropium) (CitationDecramer et al 2004). The findings of this trial are expected in the fall of 2008.
Treatment goal 3: reduce the risk of CVD and lung cancer related morbidity and mortality
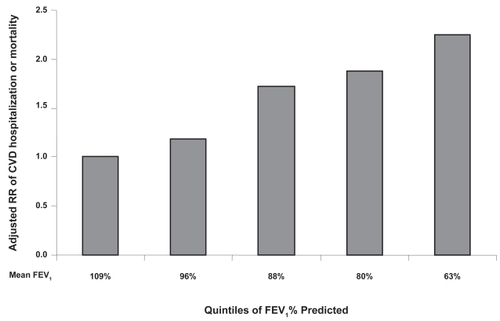
In the Lung Health Study, which studied patients with mild to moderate COPD, the leading cause of hospitalization were CVDs, accounting for nearly 50% of all hospitalizations (CitationAnthonisen et al 1994). Although deaths were rare, over 20% of all deaths were CVD in nature. In the National Health Examination Follow-up Survey, which sampled a representative mix of the US civilian adult population, baseline FEV1 was independent predictor of CVD hospitalization and mortality over 10 years of follow-up. Even within the “normal ranges” of FEV1 values, individuals who had the highest FEV1 were least likely to develop CVDs (see ), while those with reduced FEV1 values had higher risk of CVD (CitationSin et al 2005b). Mild COPD is associated with a 2-fold increased risk of CVD compared to individuals without COPD (CitationSin et al 2005b). Similarly, the risk of lung cancer is increased in mild COPD (CitationWasswa-Kintu et al 2005). Indeed, lung cancer is the most common cause of death in mild COPD, accounting for 1/3 of all deaths in this group of patients (CitationAnthonisen et al 1994). The mechanisms by which mild COPD increase the risk of CVD and lung cancer are still a mystery. Inflammation, oxidative stress, DNA mutation and shared risk factors are some of the common explanations.
Figure 2 The relationship between forced expiratory volume in one second (FEV1) and cardiovascular mortality or hospitalization in the First National Health Nutrition and Examination Survey (derived from CitationSin et al 2005b).
The Y-axis plots the relative risk of cardiovascular disease (CVD) hospitalization or mortality in subjects who participated in the NHANES 1 study. The x-axis plots the group in quintiles of FEV1 and the mean FEV1 value is shown for each of the quintile.
Smoking cessation
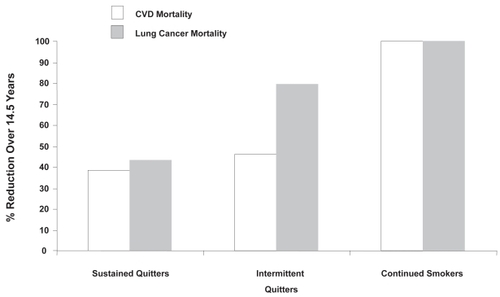
Smoking cessation is the only proven of way of reducing CVD and lung cancer in COPD patients. CVD risk is particularly responsive to smoking cessation. Compared to continued smokers, CVD mortality is reduced by over 60% in sustained quitters (CitationAnthonisen et al 2005). Interestingly, the CVD mortality risk is reduced by 54% even among intermittent quitters. In contrast, the risk of lung cancer mortality is only reduced by 20% among intermittent quitters compared to continued smokers, although it is reduced by ~55% in sustained quitters (see ).
Figure 3 The effect of smoking cessation on cardiovascular and lung cancer mortality (derived from CitationAnthonisen et al 2005).
The Y-axis plots the relative risk reduction in mortality from each of the causes relative continued smokers. Sustained quitters are defined as those who stopped smoking entirely during the follow-up period. Intermittent quitters are those who quit and re-started smoking.
Glucocorticoids
Inhaled corticosteroids may modify long-term risk of CVD and lung cancer in patients with COPD. Using a large health administrative database from Veterans Affairs, Parimon and colleagues reported that inhaled corticosteroids (≥1200 μg/day of triamcinolone, which is equivalent to ≥180 μg/day of beclomethasone) were associated with a 61% reduction in the risk of lung cancer (CitationParimon et al 2007). In a randomized control trial, Lam and colleagues evaluated the effects of inhaled budesonide on bronchial dysplasia in 113 smokers (with relatively normal lung function) over 6 months. Although there was no significant effect of inhaled budesonide on disease progression, it significantly reduced prostaglandin E2 levels in the bronchoalveolar lavage fluid and expression of p53 and BCL-2 in bronchial tissues. Inhaled budesonide also reduced the number of pulmonary nodules detected on computed tomographic (CT) scans (CitationLam et al 2004). In the Inhaled Steroid Effects Evaluation in COPD (ISEEC) study, which was a pooled analysis of 7 large trials of inhaled corticosteroids in COPD, there was a trend towards lower cancer mortality in the group that received corticosteoroids compared with placebo (relative risk, 0.55; 95% confidence interval, 0.29 to 1.03) (CitationSin et al 2005a). Long-term large-scale trials are needed to confirm these early observations and determine the effects of inhaled corticosteroids on lung cancer in COPD patients.
Inhaled corticosteroids have also been associated with reduced risk of CVD. Huiart and colleagues, using a large administrative database from Saskatchewan, reported that COPD patients who used 50 to 200 μg/day of beclomethasone (or equivalent) were 32% less likely to experience myocardial infarction than those who did not use any inhaled corticosteroids (CitationHuiart et al 2005). Macie and colleagues, using another large administrative database from Manitoba, showed that COPD patients who used inhaled corticosteroids were nearly 40% less likely to suffer a cardiac mortality than those who did not (CitationMacie et al 2006). In EUROSCOP (European Respiratory Society’s study on Chronic Obstructive Pulmonary Disease), 1,277 patients with mild to moderate COPD (mean FEV1, 77% of predicted) were assigned to inhaled budesonide or placebo for 3 years. A post hoc analysis of the safety data demonstrated that patients assigned to inhaled budesonide had 42% fewer ischemic cardiac events (defined as angina pectoris, myocardial infarction, coronary artery disease, or myocardial infarction) compared to those assigned to placebo (p = 0.048) (CitationLofdahl et al 2007). However, these data must be interpreted cautiously because the baseline event rate was low (4.2%).
Vaccination
COPD independently contributes to mortality and increased length of stay in hospitals from community-acquired pneumonia (Restrepo et al 2006). Influenza vaccination reduces overall mortality by 70% in patients with chronic lung disease (odds ratio 0.30, p < 0.001) (CitationNichol et al 1999a). However, it does not appear to modify the rate of exacerbations in patients with mild COPD (CitationMenon et al 2008; CitationPoole et al 2006). Pneumococcal vaccination is also associated with reduced risk of hospitalizations from pneumonia as well as all-cause mortality beyond that achieved with influenza vaccination (CitationNichol et al 1999b).
Summary and conclusion
COPD is a treatable disease. A short synopsis of a management strategy for mild COPD is provided in . The cornerstone of management is smoking cessation, which not only improves patient symptoms but is the only proven way of modifying its natural history and reducing mortality. Vaccinations for influenza and pneumococcus may reduce morbidity and mortality from community-acquired pneumonia. In patients who have intermittent symptoms, short-acting bronchodilators may be used on an as “as-needed” basis, while for patients with more persistent symptoms, these drugs may be given regularly (eg, 4 times a day). In patients whose symptoms are refractory to short-acting bronchodilators, long-acting bronchodilators may be provided. LABAs and tiotropium appear to have similar effectiveness for patients with mild disease. Pulmonary rehabilitation regimens may also improve exercise tolerance and quality of life. In a small minority of patients who remain symptomatic despite long-acting bronchodilators, a combination of inhaled corticosteroids and LABAs may be considered. Although inhaled corticosteroids by themselves reduce dyspnea and improve lung function, they probably should not be the sole therapy for patients with mild disease in view of their potential long-term side effects. Inhaled corticosteroids do not appear to modify the long-term decline in FEV1; however, there are emerging data suggesting their potential usefulness in reducing the risk of lung cancer and CVD, which are the leading causes of mortality and hospitalization in mild COPD. However, before this notion can be fully accepted, large-scale randomized controlled trials are needed to validate these early findings.
Table 1 Management algorithm for mild COPD
Acknowledgments
This work is supported by the Canadian Institutes of Health Research. DDS is a senior scholar with the Michael Smith Foundation for Health Research and a Canada Research Chair in COPD.
Disclosures
DDS has received research funding and honoraria for speaking engagements from GlaxoSmithKline and AstraZeneca, which make inhaled steroids and long-acting β 2 bronchodilators.
References
- AnthonisenNRConnettJEKileyJP1994Effects of smoking intervention and the use of an inhaled anticholinergic bronchodilator on the rate of decline of FEV1. The Lung Health StudyJAMA27214975057966841
- AnthonisenNRConnettJEMurrayRP2002Smoking and lung function of Lung Health Study participants after 11 yearsAm J Respir Crit Care Med166675912204864
- AnthonisenNRSkeansMAWiseRA2005The effects of a smoking cessation intervention on 14.5-year mortality: a randomized clinical trialAnn Intern Med142233915710956
- AppletonSJonesTPooleP2006Ipratropium bromide versus long-acting beta-2 agonists for stable chronic obstructive pulmonary diseaseCochrane Database Syst Rev3CD00610116856113
- BaileyWC1985Smoking cessationChest8832244028840
- BallDIBrittainRTColemanRA1991Salmeterol, a novel, long-acting beta 2-adrenoceptor agonist: characterization of pharmacological activity in vitro and in vivoBr J Pharmacol104665711686740
- BarnesPJBelvisiMGMakJC1995Tiotropium bromide Ba 679 BR. a novel long-acting muscarinic antagonist for the treatment of obstructive airways diseaseLife Sci56853910188785
- BarrRGBourbeauJCamargoCA2006Tiotropium for stable chronic obstructive pulmonary disease: A meta-analysisThorax618546216844726
- BednarekMMaciejewskiJWozniakM2008Prevalence, severity and underdiagnosis of COPD in the primary care settingThorax63402718234906
- BianchiLFoglioKPortaR2002Lack of additional effect of adjunct of assisted ventilation to pulmonary rehabilitation in mild COPD patientsRespir Med963596712113387
- BuistASMcBurnieMAVollmerWM2007International variation in the prevalence of COPD the BOLD Study: a population-based prevalence studyLancet3707415017765523
- CahillKSteadLFLancasterT2007Nicotine receptor partial agonists for smoking cessationCochrane Database Syst RevCD00610317253581
- CalverleyPMAndersonJACelliB2007Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary diseaseN Engl J Med3567758917314337
- CasaburiRKukafkaDCooperCB2005Improvement in exercise tolerance with the combination of tiotropium and pulmonary rehabilitation in patients with COPDChest1278091715764761
- CelliBRMaCneeW2004Standards for the diagnosis and treatment of patients with COPD: a summary of the ATS/ERS position paperEur Respir J239324615219010
- ChapmanKRManninoDMSorianoJB2006Epidemiology and costs of chronic obstructive pulmonary diseaseEur Respir J2718820716387952
- ClarkCJCochraneLMMackayE2000Skeletal muscle strength and endurance in patients with mild COPD and the effects of weight trainingEur Respir J1592710678627
- DecramerMCelliBTashkinDP2004Clinical trial design considerations in assessing long-term functional impacts of tiotropium in COPD: the UPLIFT trialCOPD13031217136995
- DouradoVZAntunesLCTanniSE2006Relationship of upper-limb and thoracic muscle strength to 6-min walk distance in COPD patientsChest129551716537851
- EakinEGSassi-DambronDKaplanRM1992Clinical trial of rehabilitation in chronic obstructive pulmonary diseaseJ Cardiopulmonary Rehabil1210510
- EzzatiMLopezAD2003Estimates of global mortality attributable to smoking in 2000Lancet3628475213678970
- Garcia-AymerichJLangePBenetM2007Regular physical activity modifies smoking-related lung function decline and reduces risk of chronic obstructive pulmonary disease: a population-based cohort studyAm J Respir Crit Care Med1754586317158282
- GarrodRFordKDalyC2004Pulmonary rehabilitation: analysis of a clinical servicePhysiother Res Int91112015560668
- GonzalesDRennardSINidesM2006Varenicline, an alpha4beta2 nicotinic acetylcholine receptor partial agonist, vs sustained-release bupropion and placebo for smoking cessation: a randomized controlled trialJAMA296475516820546
- HananiaNADonohueJF2007Pharmacologic interventions in chronic obstructive pulmonary disease: bronchodilatorsProc Am Thorac Soc45263417878465
- HughesJRSteadLFLancasterT2007Antidepressants for smoking cessationCochrane Database Syst RevCD00003117253443
- HuiartLErnstPRanouilX2005Low-dose inhaled corticosteroids and the risk of acute myocardial infarction in COPDEur Respir J25634915802336
- HunterMHKingDE2001COPD: management of acute exacerbations and chronic stable diseaseAm Fam Physician646031211529259
- JohanssonGLindbergARombergK2008Bronchodilator efficacy of tiotropium in patients with mild to moderate COPDPrim Care Respir J171697518536860
- JohnsonM1998The beta-adrenoceptorAm J Respir Crit Care Med158S146539817738
- KamaharaKHommaTNaitoA2004Circuit training for elderly patients with chronic obstructive pulmonary disease: a preliminary studyArch Gerontol Geriatr391031015249146
- KannerREConnettJEWilliamsDE1999Effects of randomized assignment to a smoking cessation intervention and changes in smoking habits on respiratory symptoms in smokers with early chronic obstructive pulmonary disease: the Lung Health StudyAm J Med106410610225243
- KarapolatHAtaseverAAtamazF2007Do the benefits gained using a short-term pulmonary rehabilitation program remain in COPD patients after participation?Lung185221517487535
- LamSLericheJCMcWilliamsA2004A randomized phase IIb trial of pulmicort turbuhaler budesonide. in people with dysplasia of the bronchial epitheliumClin Cancer Res1065021115475437
- LofdahlCGPostmaDSPrideNB2007Possible protection by inhaled budesonide against ischaemic cardiac events in mild COPDEur Respir J291115917331963
- Lung Health Study Group2000Effect of inhaled triamcinolone on the decline in pulmonary function in chronic obstructive pulmonary diseaseN Engl J Med3431902911136260
- MacieCWooldrageKManfredaJ2006Inhaled corticosteroids and mortality in COPDChest130640616963657
- MaltaisFHamiltonAMarciniukD2005Improvements in symptom-limited exercise performance over 8 h with once-daily tiotropium in patients with COPDChest12811687816162703
- ManSFMcAlisterFAAnthonisenNR2003Contemporary management of chronic obstructive pulmonary disease: clinical applicationsJAMA2902313614600190
- ManninoDMBuistAS2007Global burden of COPD: risk factors, prevalence, and future trendsLancet3707657317765526
- MartinezFD2005Safety of long-acting beta-agonists--an urgent need to clear the airN Engl J Med3532637916371628
- MenonBGurnaniMAggarwalB2008Comparison of outpatient visits and hospitalisations, in patients with chronic obstructive pulmonary disease, before and after influenza vaccinationInt J Clin Pract62593818284444
- MolyneuxA2004Nicotine replacement therapyBMJ328454614976103
- MorrisJFTempleW1985Spirometric “lung age” estimation for motivating smoking cessationPrev Med14655624070195
- MurrayCJLopezAD1997aAlternative projections of mortality and disability by cause 1990–2020: Global Burden of Disease StudyLancet34914985049167458
- MurrayCJLopezAD1997bGlobal mortality, disability, and the contribution of risk factors: Global Burden of Disease StudyLancet3491436429164317
- NicholKLBakenLNelsonA1999aRelation between influenza vaccination and outpatient visits, hospitalization, and mortality in elderly persons with chronic lung diseaseAnn Intern Med13039740310068413
- NicholKLBakenLWuorenmaJ1999bThe health and economic benefits associated with pneumococcal vaccination of elderly persons with chronic lung diseaseArch Intern Med15924374210665892
- NiciLDonnerCWoutersE2006American Thoracic Society/European Respiratory Society statement on pulmonary rehabilitationAm J Respir Crit Care Med173139041316760357
- O’DonnellDEAaronSBourbeauJ2007Canadian Thoracic Society recommendations for management of chronic obstructive pulmonary disease – 2007 updateCan Respir J14Suppl B5B32B
- OfirDLavenezianaPWebbKA2008Mechanisms of dyspnea during cycle exercise in symptomatic patients with GOLD stage I chronic obstructive pulmonary diseaseAm J Respir Crit Care Med177622918006885
- ParimonTChienJWBrysonCL2007Inhaled corticosteroids and risk of lung cancer among patients with chronic obstructive pulmonary diseaseAm J Respir Crit Care Med175712917185647
- ParkesGGreenhalghTGriffinM2008Effect on smoking quit rate of telling patients their lung age: the Step2quit randomised controlled trialBMJ33659860018326503
- PelkonenMTukiainenHTervahautaM2000Pulmonary function, smoking cessation and 30 year mortality in middle aged Finnish menThorax557465010950892
- PoolePJChackoEWood-BakerRW2006Influenza vaccine for patients with chronic obstructive pulmonary diseaseCochrane Database Syst RevCD00273316437444
- PumariegaAJNelsonRRotenbergL2008Varenicline-induced mixed mood and psychotic episode in a patient with a past history of depressionCNS Spectr13511418567975
- RabeKFHurdSAnzuetoA2007Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summaryAm J Respir Crit Care Med1765325517507545
- RossiGFloriniFRomagnoliM2005Length and clinical effectiveness of pulmonary rehabilitation in outpatients with chronic airway obstructionChest127105915653969
- SalpeterSRBuckleyNSOrmistonTM2006Meta-analysis: effect of long-acting beta-agonists on severe asthma exacerbations and asthma-related deathsAnn Intern Med1449041216754916
- SchroederSA2005What to do with a patient who smokesJAMA294482716046655
- SinDDMcAlisterFAManSF2003Contemporary management of chronic obstructive pulmonary disease: scientific reviewJAMA29023011214600189
- SinDDWuLAndersonJA2005aInhaled corticosteroids and mortality in chronic obstructive pulmonary diseaseThorax60992716227327
- SinDDWuLManSF2005bThe relationship between reduced lung function and cardiovascular mortality: a population-based study and a systematic review of the literatureChest1271952915947307
- SorianoJBSinDDZhangX2007A pooled analysis of FEV1 decline in COPD patients randomized to inhaled corticosteroids or placeboChest131682917356080
- SteinMDWeinstockMCHermanDS2005Respiratory symptom relief related to reduction in cigarette useJ Gen Intern Med208899416191133
- StratelisGMolstadSJakobssonP2006The impact of repeated spirometry and smoking cessation advice on smokers with mild COPDScand J Prim Health Care24133916923621
- StrausSEMcAlisterFASackettDL2000The accuracy of patient history, wheezing, and laryngeal measurements in diagnosing obstructive airway disease. CARE-COAD1 Group. Clinical Assessment of the Reliability of the Examination-Chronic Obstructive Airways DiseaseJAMA2831853710770147
- VarrasoRFungTTHuFB2007Prospective study of dietary patterns and chronic obstructive pulmonary disease among US menThorax627869117504819
- VestboJSorensenTLangeP1999Long-term effect of inhaled budesonide in mild and moderate chronic obstructive pulmonary disease: a randomised controlled trialLancet35318192310359405
- Wasswa-KintuSGanWQManSF2005Relationship between reduced forced expiratory volume in one second and the risk of lung cancer: a systematic review and meta-analysisThorax60570515994265
- WillemseBWTen HackenNHRutgersB2005Effect of 1-year smoking cessation on airway inflammation in COPD and asymptomatic smokersEur Respir J268354516264044
- WiltTJNiewoehnerDMacDonaldR2007Management of stable chronic obstructive pulmonary disease: a systematic review for a clinical practice guidelineAnn Intern Med1476395317975187