Abstract
COPD is a chronic disease and, like many other chronic diseases, there is no treatment to reverse the severity of the disease except for lung transplant. To date, no inhaled medications have been shown to improve survival. Tiotropium bromide is a long-acting inhaled anticholinergic drug for the treatment of COPD that can improve lung function, reduce symptoms and exacerbations, and improve quality of life with once-daily dosing. It was initially approved and marketed in several countries in Europe in 2002 and then approved in the US in 2004. Tiotropium is generally well tolerated with dry mouth being the main adverse effect. Other adverse effects include constipation, tachycardia, blurred vision, urinary retention and increased intraocular pressure. Despite the recently raised concerns about an excess risk of cardiovascular adverse events with inhaled anticholinergic agents, the risk/benefit ratio of tiotropium appears still favorable given the favorable safety profile demonstrated in the UPLIFT study. However, caution should be advised in patients at high risk for cardiovascular disease given the paucity of data in such patients.
Management issues in treating COPD
COPD is a chronic disease and, like many other chronic diseases, there is no treatment to reverse the severity of the disease except for lung transplant. COPD is the fourth leading cause of death in the US and is expected to be the third by 2020. The prevalence of COPD is on the increase globally with an attendant increase in morbidity and mortality.
Despite the recent advances in understanding of the disease and its management, only a few therapies can have an impact on mortality in patients with stable COPD. These therapies include smoking cessation (CitationAnthonisen et al 2005), continuous oxygen therapy for hypoxemic patients (CitationNocturnal Oxygen Therapy Trial Group 1980; CitationMedical Research Council Working Party 1981), influenza vaccination (CitationNichol et al 1999), and lung reduction surgery for selected patients (CitationFishman et al 2003).
Pharmacotherapy for COPD has been used to alleviate symptoms, prevent exacerbations, and improve exercise capacity and quality of life. However, to date no inhaled medications have been shown to improve survival. The international guidelines developed by Global Initiative for Chronic Obstructive Lung Disease currently set the standard of care (CitationRabe et al 2007) and long-acting bronchodilators are considered as the first-line maintenance therapy in patients with moderate to severe COPD.
The US Food and Drug Administration (FDA) recently issued a black box warning to long-acting beta agonists (LABAs) for asthma to alert healthcare professionals and patients that these medicines may increase the chance of severe asthma episodes and death (CitationFDA 2005). Although information is not available for similar concerns applicable to patients with COPD, caution may be advised given the relatively high prevalence of reversible component in patients with very severe COPD and exclusion of such patients in most clinical trials.
A recent observational study of a cohort of 175,906 elderly COPD patients found that the use of inhaled corticosteroids (ICSs) was associated with a dose-dependent increase in hospitalization with pneumonia followed by death within 30 days (CitationErnst et al 2007).
Combination therapy with a LABA with an ICS reduces COPD-related hospitalizations in patients with moderate to severe COPD and is the only pharmacotherapy that has been shown to alter the decline in lung function, which is a hallmark of the disease (CitationCalverley et al 2007). Further studies are needed to determine whether this combination might increase the number of adverse side effects given recently raised concerns with LABAs and ICSs.
Tiotropium bromide (Boehringer Ingelheim, Ingelheim, Germany) is a long-acting inhaled anticholinergic agent for the treatment of COPD that can improve lung function, reduce symptoms and COPD-related hospitalizations, and improve quality of life with once-daily dosing. The results of some studies have suggested that tiotropium is more effective than LABAs in reducing COPD-related hospitalizations and improving quality of life (CitationBrusasco et al 2003; CitationOba 2007). Tiotropium was initially approved and marketed in several countries in Europe in June 2002 and then in the US in early 2004.
Two recently published studies have raised concerns for a possible increase in mortality and cardiovascular events with the use of inhaled anticholinergics. In a nested case-control study of a cohort of 32,120 COPD patients and 320,501 control participants, ipratropium bromide (Boehringer Ingelheim, Ingelheim, Germany) was associated with an increased risk for mortality, whereas ICSs appeared to reduce the risk for death (CitationLee et al 2008). In a 17-trial meta-analysis, the use of inhaled anticholinergics (ipratropium and tiotropium) was associated with an increased risk for a composite of myocardial infarction (MI), stroke and cardiovascular death (CitationSingh et al 2008).
Although recent guidelines have advocated the use of inhaled anticholinergics for disease control (CitationRabe et al 2007), there has been a growing concern in the clinical community that inhaled anticholinergics might increase the risk for cardiovascular events and mortality as describe above. This review examines the safety, tolerability and risk/benefit ratio of a long-acting anticholinergic agent, tiotropium bromide.
Overview of pharmacology of tiotropium and short- and long-acting bronchodilators
Short- and long-acting bronchodilators
Short-acting beta-2 agonists act directly upon bronchial smooth muscle causing the airways to dilate for up to 6 hours. In turn, this improves ‘smooth muscle dependent’ outcome parameters such as symptoms and airway caliber (Sestini et al 2003).
The prime action of beta-adrenergic drugs is to stimulate adenyl cylase, the enzyme that catalyzes the formation of cyclic-3, 5-adenosine monophosphate from adenosine triphosphate.
Similar to short-acting agents, LABAs act directly upon beta-2 adrenoreceptors, causing smooth muscle to relax and airways to dilate. Both salmeterol (GlaxoSmithKline, Brentford, UK) and formoterol (Foradil®, Novartis Pharma AG, Basel, Switzerland) are relatively lipophilic, which may in part explain their prolonged duration of action.
Salmeterol interacts with both the active site and an exosite of the beta-2 adrenoreceptor, and the molecular basis of this interaction is termed the salmeterol hinge (charniere) theory (CitationPauwels et al 2001; CitationCelli and MacNee 2004). Formoterol is partially lipophilic and forms a membrane depot. Formoterol has a more rapid onset of action than salmeterol (CitationNational Collaborating Centre for Chronic Conditions 2004).
The onset of action for both short- and long-acting beta-2 agonist is 5 to 15 min. Effects of short-acting agents usually last only 4 to 6 hours whereas those of LABAs last 12 hours.
Short- and long-acting anticholinergics
The characteristic airflow obstruction in COPD is multi-factorial in origin and in part due to potentially reversible high cholinergic tone (CitationGross and Skorodin 1984; CitationChapman et al 1990). Moreover, vagally mediated mechanisms are also implicated in enhanced submucosal gland secretion in patients with COPD (CitationDahl et al 2001).
Short-acting anticholinergics such as ipratropium (with a duration of action of 3 to 6 hours) offset high resting bronchomotor tone to relax smooth muscle with subsequent improvement in airway caliber (CitationMahler et al 1999; CitationDahl et al 2001; CitationRennard et al 2001).
Three main subtypes (M1, M2 and M3) of muscarinic receptors exist. The activation of both M1 and M3 receptors results in bronchoconstriction whereas the M2 receptor is protective against such an effect.
In contrast to ipratropium, tiotropium dissociates rapidly from the M2 receptor (therefore minimizing the loss of any putative benefit) and dissociates only slowly from the M3 receptor (CitationDisse et al 1993). This in turn causes a reduction in resting bronchomotor tone, smooth muscle to relax and airways to dilate for a greater length of time. The prolonged duration of action of tiotropium therefore facilitates once-daily administration with potential concordance benefits.
The peak onset of bronchodilation with tiotropium occurs persisting between 1 to 3 hours with improvements in FEV1 for over 24 hours (CitationBarnes et al 2000). In a pharmacodynamic study, it was discovered that 90% of the improvement in was achieved within 24 hours of first inhalation of FEV1 tiotropium, while ongoing improvements in forced vital capacity were expected beyond 1 week of regular treatment (Citationvan Noord et al 2002).
Tolerability
Inhaled LABAs are generally well tolerated although adverse effects such as fine tremor and palpitations are occasionally troublesome. These agents should be used in caution in patients with cardiovascular disease, at risk of developing prolongation of the QT interval and in whom concomitant drug administration may increase the risk of serious hypokalaemia (CitationSalpeter et al 2004).
Tiotropium is generally well tolerated and poorly absorbed from the gastrointestinal tract, but as with all inhaled anti-cholinergic agents, care should be taken in patients with glaucoma and prostatic hyperplasia. In clinical trials comparing tiotropium with placebo, the frequency of dry mouth, constipation, and urinary tract infection appears to increase with patient age. Further details are described in the following section.
It is also important to point out that no tachyphylaxis to its bronchodilatory effect has been observed with tiotropium (CitationCasaburi et al 2000), a phenomenon that is known to occur with LABAs (CitationDonohue et al 2003).
Safety and tolerability of tiotropium
Comparison with placebo
Tiotropium was generally well tolerated in randomized clinical trials which ranged from 2 to 12 months (CitationCasaburi et al 2002; CitationBrusasco et al 2003; CitationNiewoehner et al 2005; CitationDusser et al 2006; CitationVerkindre et al 2006; CitationChan et al 2007; CitationCriner et al 2008). In all studies, the completion rate was higher with tiotropium (77%–98%) than with placebo (71%–92%). The most commonly cited reason for withdrawal was worsening of COPD or adverse events. The completion rate in a recently published 4-year randomized controlled trial involving 5993 patients (UPLIFT, Understanding Potential Long-Term Impacts on Function with Tiotropium; CitationTashkin et al 2008) was significantly higher with tiotropium than with placebo (63% vs 55%, p < 0.0001). The most common reason for withdrawal in the UPLIFT study was adverse events.
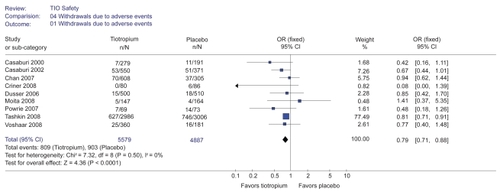
We conducted a pooled analysis to examine the incidence of serious adverse events (SAEs) and all-cause mortality using the same methods as in a recent meta-analysis by Singh et al. Ten randomized control trials reported incidence of SAEs (CitationCasaburi et al 2000, Citation2002, Citation2005; CitationCovelli et al 2005; CitationNiewoehner et al 2005; CitationChan et al 2007; CitationCriner et al 2008; CitationMoita et al 2008; CitationTashkin et al 2008; CitationVoshaar et al 2008) and 11 trials reported all-cause mortality (CitationCasaburi et al 2000, Citation2002, 2003, Citation2005; CitationNiewoehner et al 2005; CitationChan et al 2007; CitationPowrie et al 2007; CitationCriner et al 2008; CitationMoita et al 2008; CitationTashkin et al 2008; CitationVoshaar et al 2008). There was no difference in all-cause mortality between the tiotropium and placebo recipients when all reported results were combined (odds ratio [OR] 0.94; 95% confidence interval [CI] 0.82–1.08). However, the incidence of SAEs was significantly lower in the tiotropium recipients (OR 0.88; 95% CI 0.81–0.96). () The most frequently reported SAEs were respiratory events such as COPD exacerbation or pneumonia (CitationCasaburi et al 2005; CitationCovelli et al 2005; CitationNiewoehner et al 2005; CitationCriner et al 2008; CitationTashkin et al 2008). The incidence of discontinuation due to adverse events was significantly lower with tiotropium than with placebo (21% vs 25%, p < 0.0001) in the UPLIFT study (CitationTashkin et al 2008) as well as in a pooled analysis conducted by us (OR 0.79; 95% CI 0.71–0.88) ().
Figure 1 Summary effects of tiotropium on serious adverse events and all-cause mortality.
Abbreviations: CI, confidence interval; OR, odds ratio.
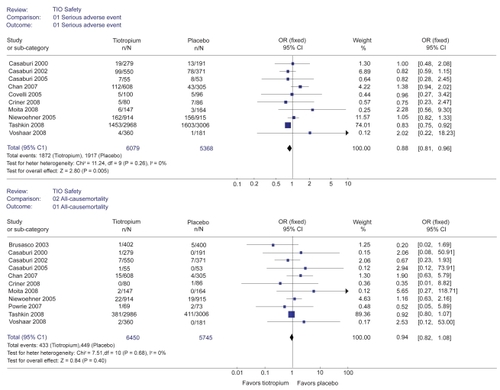
Figure 2 Forest plot examining the incidence of discontinuation due to adverse events with tiotropium vs placebo including the UPLIFT study.
The causes of death were consistent with what might be expected in the patient population. In a meta-analysis, pulmonary mortality was non-significantly lower with tiotropium than with placebo (OR 0.5; 95% CI 0.19–1.29) (CitationBarr et al 2006). Cardiovascular (OR 1.17; 95% CI 0.54–2.51) and cancer mortality (OR 0.77; 95% CI 0.28–2.12) were similar in the tiotropium and placebo recipients.
There has been a growing concern in the clinical community that inhaled anticholinergics might increase the risk for cardiovascular adverse events. Although tiotropium was approved by FDA in 2004, the Pulmonary and Allergy Drugs Advisory Committee of the agency concerned about suggestions of increased cardiovascular risk when pivotal clinical trials were reviewed (CitationFDA 2002). CitationBarr et al (2006) conducted a meta-analysis in 2006 in which the frequency of arrhythmia was significantly higher with tiotropium than with placebo when adjusted for statistical heterogeneity (OR 2.33; 95% CI 1.11–4.88).
In March 2008, The FDA issued a warning about a potential increased risk of stroke in patients using tiotropium (CitationFDA 2008). Boehringer Ingelheim, the manufacturer of tiotropium, reported to the agency a preliminary estimate that the risk of stroke during 29 clinical trials was 8 patients per 1000 patients treated for 1 year with tiotropium and 6 patients per 1000 patients treated with placebo for the same amount of time. In these trials, which included approximately 13,500 patients with COPD, the estimated excess risk of any type of stroke caused by tiotropium was 2 patients for each 1000 patients using tiotropium for 1 year. The FDA cautioned practitioners that the findings were only preliminary and no regulatory action had been taken at that time.
After the FDA warning, two major studies were published concerning the possible association between inhaled anticholinergics and elevated risk for all-cause mortality and cardiovascular events. One study, which was a nested case-control study with a cohort of 32,120 case patients and 320,501 control participants, showed that ipratropium was associated with an increased risk for mortality in patients with COPD, whereas inhaled corticosteroids appeared to reduce the risk for death (CitationLee et al 2008). The use of ipratropium was associated with a higher risk of all-cause mortality (OR 1.11; 95% CI 1.08–1.15) and a 34 % increase (95% CI 22%–47%) in the risk for cardiovascular death, whereas ICSs and LABAs both reduced the risk for all-cause mortality by 20% and 8%. ICSs were also associated with a 20% decrease (95% CI 12%–28%) in the risk for cardiovascular death (CitationLee et al 2008).
The other study was a 17-trial meta-analysis, in which the use of inhaled anticholinergics (ipratropium and tiotropium), compared with control (placebo or comparator), was associated with an increased risk for a composite of MI, stroke and cardiovascular death (CitationSingh et al 2008). The use of inhaled anticholinergics in patients with COPD was associated an increase risk for MI with a number needed to harm of 174 per year and an increased risk for cardiovascular death with a number needed to harm of 40 per year. The authors concluded that clinician should closely monitor patients with COPD who were receiving an inhaled anticholinergic agent.
Soon after the above two studies were published, the manufacturer reported the results of the UPLIFT study, which is a large 4-year, randomized, placebo-controlled, double-blind trial of tiotropium in patients with moderate to severe COPD conducted at 490 centers in 37 courtiers involving 5993 patients (Tashkin et al 2004). The UPLIFT study provided additional long-term safety data and additional insight into the risk of stroke or other safety findings of tiotropium.
Tiotropium showed a trend toward reduced mortality (14.9% vs 16.5%, hazard ratio [HR] 0.89; 95% CI 0.79–1.02). The incidence of adverse events (92.6% vs 92.3%) and the proportion of SAEs (51.6% vs 50.2%) were similar in the tiotropium and placebo group. Cardiovascular adverse events were significantly less with tiotropium (relative risk [RR] 0.84; 95% CI 0.73–0.98). The incidence of MI was also less with tiotropium (RR 0.71; 95% CI 0.52–0.99). There were 82 strokes among the 2987 patients (2.7%) taking tiotropium and 80 strokes among the 3006 patients (2.7%) taking placebo. The difference was not statistically significant.
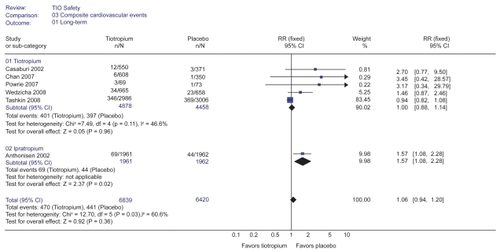
We reanalyzed the meta-analysis conducted by CitationSingh et al (2008) incorporating the results of UPLIFT study to further investigate the possible association between tiotropium and increased risk of cardiovascular events. The association between inhaled anticholinergics (ipratropium and tiotropium) and increased risk for a composite of MI, stroke and cardiovascular death became no longer significant with the use of tiotropium ().
Figure 3a Forest plot examining the incidence of composite cardiovascular events with anticholinergics vs control. All studies (short and long term) including UPLIFT study.
Abbreviations: CI, confidence interval; RR, relative risk.
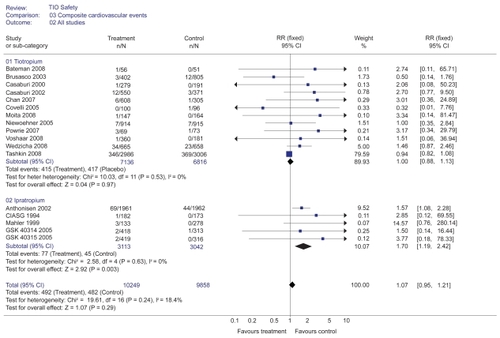
Figure 3b Forest plot examining the incidence of composite cardiovascular events with anticholinergics vs control. Long-term trials (≥6 months) including UPLIFT study.
We also found the following errors in the meta-analysis by CitationSingh et al (2008): 1) The number of the control group in the study by Chan et al was 305 instead of 350 (CitationChan et al 2007). 2) The incidence of serious cardiovascular events in the study by Wedzicha et al was 34 with tiotropium and 23 with placebo instead of 23 and 13 (CitationWedzicha et al 2008). 3) The study by CitationDonohue et al (2002) should have been excluded since CitationBrusasco et al (2003) reported combined results of the study by Donohue et al and another unpublished study (CitationBarr 2004). Although these errors did not affect the results, they were corrected in our pooled analysis.
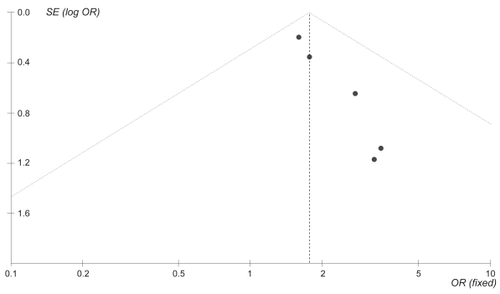
The difference in the cardiovascular events in the Singh’s study was primarily derived from long-term studies (ie, duration of study >6 months). We found evidence of possible publication bias when the long-term studies were analyzed with a funnel plot () and a statistical test (Horbold-Egger: bias = 0.722318 [92.5% CI = 0.450252–0.994383] p = 0.003). The difference in the cardiovascular events detected in the Singh’s study could be due to publication bias. The FDA is currenlty reconsidering its recent warning that tiotropium might raise stroke risk as of October 10, 2008. The FDA said it would take several months for it to finish its review of the huge amount of data from the UPLIFT study.
Figure 4 Funnel plot inspection on major adverse cardiovascular events in the long-term trials reveals significant asymmetry which suggests publication bias.
The adverse event data indicated that anticholinergic effects were more frequent with tiotropium (CitationFDA 2002; CitationBarr et al 2006). Dry mouth was by far the most common with an incidence of 16% with tiotropium and 2.7% with placebo (CitationCasaburi et al 2002) and more frequent in women and older patients (CitationFDA 2002). The peak incidence has been reported to occur after 3 to 4 weeks of therapy, when steady-state concentrations are reached. Dry mouth was generally mild and resolved during treatment in most patients and less than 1% of the patients withdrew from the clinical studies as a result (CitationCasaburi et al 2002, 2003; CitationVincken et al 2002). Other anticholinergic effects included constipation and urinary effects. The relative risk of urinary retention was significantly increased in a pooled analysis (RR 10.9; 95% CI 1.26–94.9) (CitationKesten et al 2006). Upper respiratory tract infections were also more common with tiotropium than with placebo (41.1% vs 37.2%) (CitationFDA 2002). The observation that dry mouth, constipation, and urinary tract infection occur more frequently with older age suggests that these adverse events represent systemic effects of the drug (CitationFDA 2002). Tiotropium is associated with detectable plasma concentrations, particularly with chronic use. Other factors that can increase systemic exposure are impaired renal function, increasing age, concomitant cimetidine, and cytochrome P450 2D6 poor metabolizers (CitationFDA 2002). It should be noted that patients with urinary problems and glaucoma were excluded in the most clinical trials; therefore, anticholinergic side effects may be more common in a real-world setting. The adverse effects of tiotropium are summarized in .
Table 1 Adverse effects of tiotropium
Comparison with other bronchodilators
The tolerability of tiotropium in comparison with ipratropium (CitationVincken et al 2002), salmeterol (CitationBrusasco et al 2003; CitationBriggs et al 2005), formoterol (Citationvan Noord et al 2005), or salmeterol/fluticasone (SFC) combination (CitationBateman et al 2008; CitationWedzicha et al 2008) was investigated in randomized clinical trials.
Fewer patients treated with tiotropium than with ipratropium (15.2% vs 21.2%) withdrew from the 1-year study (CitationVincken et al 2002) but the difference was not statistically significant (p = 0.08). The withdrawal rates were also lower with tiotropium than with salmeterol. The difference was statistically significant in the 6-month trial (15.4% vs 18.8%; p < 0.05) (CitationBrusasco et al 2003) but not in the 3-month trial (CitationBriggs et al 2005) (8.8% vs 12.6%; p = 0.15). Similar proportions of tiotropium and formoterol recipients withdrew from the randomized crossover study (Citationvan Noord et al 2005).
The withdrawal rate was similar between tiotropium and SFC in a 6-week trial (CitationBateman et al 2008. However, in a 2-year randomized control trial, the withdrawal rate was significantly higher with tiotropium compared with SFC (HR 1.29; 95% CI 1.08–1.54; p = 0.005) (CitationWedzicha et al 2008). In this study, more patients treated with tiotropium withdrew from the study because of COPD exacerbation, perceived lack of efficacy, or unwillingness to remain in the study.
There was no statistically significant difference in all-cause mortality comparing tiotropium with ipratropium (CitationVincken et al 2002) or salmeterol (CitationBrusasco et al 2003; CitationKesten et al 2006). However, mortality was significantly higher with tiotropium than with SFC (6% vs 3%; p = 0.032) (CitationWedzicha et al 2008). The leading causes of death, in order of prevalence, were cardiac, respiratory and neoplastic disorders. The incidence of cardiac death was non-significantly higher with tiotropium than with SFC (3% vs 1%; p = 0.09). The authors concluded that further studies powered on mortality would be required to confirm these findings since the all-cause mortality was not a primary outcome in the study (CitationWedzicha et al 2008). It should be kept in mind that this study compared one drug (ie, tiotropium) with a combination therapy with a LABA and an ICS (ie, salmeterol plus fluticasone).
Dry mouth occurred more frequently with tiotropium than with ipratropium (12.1% vs 6.1%; p = 0.03) (CitationVincken et al 2002) or with salmeterol (8.2% vs 1.7%; p < 0.05) (CitationBrusasco et al 2003). According to a recent meta-analysis (CitationBarr et al 2006), other anticholinergic adverse events such as constipation, urinary retention and urinary tract infections occurred more frequently with tiotropium than with ipratropium or salmeterol. However, the differences were not statistically significant. The incidence of adverse cardiac events was similar between tiotropium and SFC (5% vs 3%, CitationWedzicha et al 2008) or salmeterol (CitationBrusasco et al 2003; CitationSingh et al 2008). However, it is unlikely that these studies were sufficiently powered to detect a significant difference in the incidence of cardiac adverse events.
Patient satisfaction, adherence, and quality of life
In clinical practice, frequent administration creates a problem with drug adherence. Adherence with inhaled medications are generally fair to poor with compliance rates of somewhere between 10% and 50% (CitationRand et al 1995; CitationBreekveldt-Postma et al 2004; CitationBender et al 2006; Kingsman et al 2007). Once-a-day administration with tiotropium is likely to improve compliance compared to multiple daily administration required with other inhaled medications. In a retrospective analysis including 5330 patients in the Netherlands, about 37% of new users of tiotropium continued treatment for 1 year whereas only 14% with ipratropium, 13% with LABA and 17% with LABA plus ICS remained on the treatment for the same duration (CitationBreekveldt-Postma et al 2007). A Canadian study also showed that patients taking tiotropium had significantly longer persistence at 12 months compared with other inhaled medications including ipratropium, ipratropium plus salbutamol, formoterol, formoterol plus budesonide, salmeterol, and salmeterol plus fluticasone (53% vs 7% to 30%; all p < 0.0001) (CitationCramer et al 2007).
There is a paucity of data on patient satisfaction with long-acting bronchodilators.
Risk benefit analysis of tiotropium
Tiotropium can improve lung function, reduce symptoms and exacerbations, and improve quality of life with once-daily dosing (CitationBarr et al 2006). Tiotropium also showed a trend toward reduced mortality and induced long-term improvement in the UPLIFT study (CitationTashkin et al 2008).
Tiotropium is generally well tolerated with dry mouth being the main adverse effect.
Despite recently raised concerns about possible association between inhaled anticholinergics and elevated cardiovascular events, the risk/benefit ratio of tiotropium still appears favorable in symptomatic patients with moderate-to-severe COPD given the favorable safety profile demonstrated in the UPLIFT study. There were fewer cardiovascular events with tiotropium compared with placebo in the UPLIFT study. Our pooled analyses incorporating the UPLIFT study also confirmed the cardiac safety of tiotropium (, ). Respiratory events including COPD-related exacerbations and hospitalizations were also significantly less with tiotropium (RR 0.84; 95% CI 0.77–0.92) as shown in previous studies (CitationBarr et al 2006; CitationOba 2007).
One caveat is that cardiac safety database is very limited in high-risk patients such as those with coronary artery disease, heart failure, cardiac arrhythmia, hypoxemia requiring daytime oxygen therapy, and a creatinine >2.0 mg/dL since such patients were excluded from phase III clinical trials (CitationVincken et al 2002; CitationBrusasco et al 2003; CitationCasaburi et al 2005; CitationNiewoehner et al 2005; CitationDusser et al 2006; CitationTashkin et al 2008). Those patients may be at increased risk of drug-related cardiac events in a real-world setting.
Currently, it is largely clinician and patient preferences as to which inhaled long-acting bronchodilator to be used as the first-line maintenance therapy in symptomatic patients with moderate-to-severe COPD (CitationQaseem et al 2007; CitationRabe et al 2007). For example, clinicians may prefer SFC over tiotropium given possible mortality benefit and/or better tolerability with SFC (CitationCalverley et al 2007; CitationWedzicha et al 2008). Clinicians and patients may elect to use tiotropium over salmeterol if patients are experiencing frequent exacerbations or hospitalizations (CitationBarr et al 2006). Third-party payers may elect tiotropium over salmeterol as a preferred drug in their formulary given more favorable cost-effectiveness ratio with tiotropium (CitationOba 2007).
Conclusions
Tiotropium bromide is a long-acting inhaled anticholinergic agent and one of the first-line maintenance therapies in symptomatic patients with moderate-to-severe COPD. Tiotropium is generally well tolerated with dry mouth being the main adverse effect, which is generally not troublesome enough to discontinue the drug. Other adverse effects include constipation, tachycardia, blurred vision, urinary retention and increased intraocular pressure. Despite the recently raised concerns about an excess risk of cardiovascular adverse events with inhaled anticholinergic agents, the risk/benefit ratio of tiotropium appears still favorable given the favorable safety profile demonstrated in the UPLIFT study. However, caution should be advised in patients at high risk for cardiovascular disease given the paucity of data in such patients. The same is true for LABAs in patients with a reactive airway component and ICSs in patients at high risk for pneumonia.
Disclosures
The authors have no conflicts of interest to disclose.
References
- AnthonisenNRConnettJEEnrightPL2002Hospitalizations and mortality in the Lung Health StudyAm J Respir Crit Care Med166333912153966
- AnthonisenNRSkeansMAWiseRA2005The effects of a smoking cessation intervention on 14.5-year mortality: a randomized clinical trialAnn Intern Med142233915710956
- BarnesPJ2000The pharmacological properties of tiotropiumChest11763S6610673478
- BarrRGManagement of chronic obstructive pulmonary disease2004JAMA29110667 author reply 106714996770
- BarrRGBourbeauJCamargoCA2006Tiotropium for stable chronic obstructive pulmonary disease: A meta-analysisThorax618546216844726
- BatemanEDvan DykMSagriotisA2008Comparable spirometric efficacy of tiotropium compared with salmeterol plus fluticasone in patients with COPD: a pilot studyPulm Pharmacol Ther2120517118684
- BenderBGPedanAVarastehLT2006Adherence and persistence with fluticasone propionate/salmeterol combination therapyJ Allergy Clin Immunol11889990417030244
- Breekveldt-PostmaNSGerritsCMLammersJW2004Persistence with inhaled corticosteroid therapy in daily practiceRespir Med98752915303640
- Breekveldt-PostmaNSKoerselmanJErkensJA2007Enhanced persistence with tiotropium compared with other respiratory drugs in COPDRespir Med101139840517368011
- BriggsDDJrCovelliHLapidusR2005Improved daytime spirometric efficacy of tiotropium compared with salmeterol in patients with COPDPulm Pharmacol Ther1839740416179215
- BrusascoVHodderRMiravitllesM2003Health outcomes following treatment for six months with once daily tiotropium compared with twice daily salmeterol in patients with COPDThorax5839940412728159
- CalverleyPMAndersonJACelliB2007Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary diseaseN Engl J Med3567758917314337
- CasaburiRBriggsDDJrDonohueJF2000The spirometric efficacy of once-daily dosing with tiotropium in stable COPD: a 13-week multi-center trial. The US Tiotropium Study GroupChest118129430211083677
- CasaburiRKukafkaDCooperCB2005Improvement in exercise tolerance with the combination of tiotropium and pulmonary rehabilitation in patients with COPDChest1278091715764761
- CasaburiRMahlerDAJonesPW2002A long-term evaluation of once-daily inhaled tiotropium in chronic obstructive pulmonary diseaseEur Respir J192172411866001
- CelliBRMacNeeW2004Standards for the diagnosis and treatment of patients with COPD: a summary of the ATS/ERS position paperEur Respir J239324615219010
- ChanCKMaltaisFSigouinC2007A randomized controlled trial to assess the efficacy of tiotropium in Canadian patients with chronic obstructive pulmonary diseaseCan Respir J144657218060091
- ChapmanKR1990The role of anticholinergic bronchodilators in adult asthma and chronic obstructive pulmonary diseaseLung1682953032143551
- COMBIVENT Inhalation Aerosol Study Group1994In chronic obstructive pulmonary disease, a combination of ipratropium and albuterol is more effective than either agent alone. An 85-day multicenter trialChest105141198181328
- CovelliHBhattacharyaSCassinoC2005Absence of electrocardiographic findings and improved function with once-daily tiotropium in patients with chronic obstructive pulmonary diseasePharmacotherapy2517081816305289
- CramerJABradley-KennedyCScaleraA2007Treatment persistence and compliance with medications for chronic obstructive pulmonary diseaseCan Respir J1425917315055
- CrinerGJSharafkhanehAPlayerR2008Efficacy of tiotropium inhalation powder in african-american patients with chronic obstructive pulmonary diseaseCOPD5354118259973
- DahlRGreefhorstLANowakD2001Inhaled formoterol dry powder versus ipratropium bromide in chronic obstructive pulmonary diseaseAm J Respir Crit Care Med1647788411549532
- DisseBReichlRSpeckG1993Ba 679 BR, a novel long-acting anticholinergic bronchodilatorLife Sci52537448441333
- DonohueJFMenjogeSKestenS2003Tolerance to bronchodilating effects of salmeterol in COPDRespir Med9710142014509555
- DonohueJFvan NoordJABatemanED2002A 6-month, placebo-controlled study comparing lung function and health status changes in COPD patients treated with tiotropium or salmeterolChest122475512114338
- DusserDBravoMLIaconoP2006The effect of tiotropium on exacerbations and airflow in patients with COPDEur Respir J275475516507855
- ErnstPGonzalezAVBrassardP2007Inhaled corticosteroid use in chronic obstructive pulmonary disease and the risk of hospitalization for pneumoniaAm J Respir Crit Care Med176162617400730
- FishmanAMartinezFNaunheimK2003A randomized trial comparing lung-volume-reduction surgery with medical therapy for severe emphysemaN Engl J Med34820597312759479
- Food and Drug Administration2002Pulmonary-Allergy Drugs Advisory Committee. 2002 Clinical briefing documentIntegrated review of safety, NDA21395
- Food and Drug Administration2005FDA Public Health Advisory. Serevent Diskus (salmeterol xinafoate inhalation powder), Advair Diskus (fluticasone propionate and salmeterol inhalation powder), Foradil Aerolizer (formoterol fumarate inhalation powder)Accessed October, 2008 URL: http://www.fda.gov/cder/drug/advisory/LABA.htm
- Food and Drug Administration2008Early Communication about an Ongoing Safety Review of TiotropiumAccessed October, 2008 URL: http://www.fda.gov/cder/drug/early_comm/tiotropium.htm
- GlaxoSmithKline2005Clinical trial register for a multicenter, randomized, double-blind, double-dummy, parallel group, 8-week comparison of salmeterol xinafoate versus ipratropium bromide versus salmeterol xinafoate plus ipratropium bromide versus placebo in subjects with chronic obstructive pulmonary diseaseAccessed October, 2008 URL: http://www.gsk-clinicalstudyregister.com/files/pdf/2981.pdf
- GlaxoSmithKline2005Clinical trial register for a multicenter, randomized, double-blind, double-dummy, parallel-group, 8-week comparison of salmeterol xinafoate versus ipratropium bromide versus salmeterol xinafoate plus ipratropium bromide versus placebo in subjects with chronic obstructive pulmonary diseaseAccessed October, 2008 URL: http://www.gsk-clinicalstudyregister.com/files/pdf/2843.pdf
- GrossNJSkorodinMS1984Role of the parasympathetic system in airway obstruction due to emphysemaN Engl J Med31142156749189
- KestenSJaraMWentworthC2006Pooled clinical trial analysis of tiotropium safetyChest130169570317166984
- KrigsmanKNilssonJLRingL2007Refill adherence for patients with asthma and COPD: comparison of a pharmacy record database with manually collected repeat prescriptionsPharmacoepidemiol Drug Saf16441817006959
- LeeTAPickardASAuDH2008Risk for death associated with medications for recently diagnosed chronic obstructive pulmonary diseaseAnn Intern Med14963809018794557
- MahlerDADonohueJFBarbeeRA1999Efficacy of salmeterol xinafoate in the treatment of COPDChest1159576510208192
- Medical Research Council Working Party1981Long term domiciliary oxygen therapy in chronic hypoxic cor pulmonale complicating chronic bronchitis and emphysemaLancet168166110912
- MoitaJBarbaraCCardosoJ2008Tiotropium improves FEV1 patients with COPD irrespective of smoking statusPulm Pharmacol Ther211465117693107
- National Collaborating Centre for Chronic Conditions2004Chronic obstructive pulmonary disease. National clinical guideline on management of chronic obstructive pulmonary disease in adults in primary and secondary careThorax59Suppl 11232
- NicholKLBakenLNelsonA1999Relation between influenza vaccination and outpatient visits, hospitalization, and mortality in elderly persons with chronic lung diseaseAnn Intern Med13039740310068413
- NiewoehnerDERiceKCoteC2005Prevention of exacerbations of chronic obstructive pulmonary disease with tiotropium, a once-daily inhaled anticholinergic bronchodilator: a randomized trialAnn Intern Med1433172616144890
- Nocturnal Oxygen Therapy Trial Group1980Continuous or nocturnal oxygen therapy in hypoxemic chronic obstructive lung disease: a clinical trial. Nocturnal Oxygen Therapy Trial GroupAnn Intern Med9339186776858
- ObaY2007Cost-effectiveness of long-acting bronchodilators for chronic obstructive pulmonary diseaseMayo Clin Proc825758217493425
- PauwelsRABuistASCalverleyPM2001Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. NHLBI/WHO Global Initiative for Chronic Obstructive Lung Disease (GOLD) Workshop summaryAm J Respir Crit Care Med16312567611316667
- PowrieDJWilkinsonTMDonaldsonGC2007Effect of tiotropium on sputum and serum inflammatory markers and exacerbations in COPDEur Respir J30472817504798
- QaseemASnowVShekelleP2007Diagnosis and management of stable chronic obstructive pulmonary disease: a clinical practice guideline from the American College of PhysiciansAnn Intern Med147633817975186
- RabeKFHurdSAnzuetoA2007Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summaryAm J Respir Crit Care Med1765325517507545
- RandCSNidesMCowlesMK1995Long-term metered-dose inhaler adherence in a clinical trial. The Lung Health Study Research GroupAm J Respir Crit Care Med15258087633711
- RennardSIAndersonWZuWallackR2001Use of a long-acting inhaled beta2-adrenergic agonist, salmeterol xinafoate, in patients with chronic obstructive pulmonary diseaseAm J Respir Crit Care Med16310879211316640
- SalpeterSROrmistonTMSalpeterEE2004Cardiovascular effects of beta-agonists in patients with asthma and COPD: a meta-analysisChest12523092115189956
- SestiniPRenzoniERobinsonS2002Short-acting beta 2 agonists for stable chronic obstructive pulmonary diseaseCochrane Database Syst RevCD00149512519559
- SinghSLokeYKFurbergCD2008Inhaled anticholinergics and risk of major adverse cardiovascular events in patients with chronic obstructive pulmonary disease: a systematic review and meta-analysisJAMA30014395018812535
- TashkinDPCelliBSennS2008A 4-year trial of tiotropium in chronic obstructive pulmonary diseaseN Engl J Med35915435418836213
- van NoordJASmeetsJJCustersFL2002Pharmacodynamic steady state of tiotropium in patients with chronic obstructive pulmonary diseaseEur Respir J196394411998992
- van NoordJAAumannJLJanssensE2005Comparison of tiotropium once daily, formoterol twice daily and both combined once daily in patients with COPDEur Respir J262142216055868
- VerkindreCBartFAguilaniuB2006The effect of tiotropium on hyperinflation and exercise capacity in chronic obstructive pulmonary diseaseRespiration73420716484769
- VinckenWvan NoordJAGreefhorstAP2002Improved health outcomes in patients with COPD during 1 yr’s treatment with tiotropiumEur Respir J192091611871363
- VoshaarTLapidusRMaleki-YazdiR2008A randomized study of tiotropium Respimat Soft Mist inhaler vs. ipratropium pMDI in COPDRespir Med1021324117996436
- WedzichaJACalverleyPMSeemungalTA2008The prevention of chronic obstructive pulmonary disease exacerbations by salmeterol/fluticasone propionate or tiotropium bromideAm J Respir Crit Care Med177192617916806