Abstract
Bronchiectasis is defined by permanent and abnormal widening of the bronchi. This process occurs in the context of chronic airway infection and inflammation. It is usually diagnosed using computed tomography scanning to visualize the larger bronchi. Bronchiectasis is also characterized by mild to moderate airflow obstruction. This review will describe the pathophysiology of noncystic fibrosis bronchiectasis. Studies have demonstrated that the small airways in bronchiectasis are obstructed from an inflammatory infiltrate in the wall. As most of the bronchial tree is composed of small airways, the net effect is obstruction. The bronchial wall is typically thickened by an inflammatory infiltrate of lymphocytes and macrophages which may form lymphoid follicles. It has recently been demonstrated that patients with bronchiectasis have a progressive decline in lung function. There are a large number of etiologic risk factors associated with bronchiectasis. As there is generally a long-term retrospective history, it may be difficult to determine the exact role of such factors in the pathogenesis. Extremes of age and smoking/chronic obstructive pulmonary disease may be important considerations. There are a variety of different pathogens involved in bronchiectasis, but a common finding despite the presence of purulent sputum is failure to identify any pathogenic microorganisms. The bacterial flora appears to change with progression of disease.
Introduction
Bronchiectasis is defined by the presence of permanent and abnormal dilation of the bronchi.Citation1,Citation2 This usually occurs in the context of chronic airway infection causing inflammation. The main clinical manifestation is a productive cough. Bronchiectasis is currently nearly always diagnosed using high-resolution computed tomography (HRCT) scanning. The main diagnostic features are: 1) internal diameter of a bronchus is wider than its adjacent pulmonary artery; 2) failure of the bronchi to taper; and 3) visualization of bronchi in the outer 1–2 cm of the lung fields.Citation3 This review will describe the pathophysiology of noncystic fibrosis (CF) bronchiectasis.
With the widespread availability of HRCT it has been realized that bronchiectasis remains a common and important cause of respiratory disease. It has been estimated that there are at least 110,000 adults in the United States with this condition.Citation4 In addition, there is overlap with chronic obstructive pulmonary disease (COPD) with two studies reporting an incidence of bronchiectasis in COPD as being 29%Citation5 and 50%,Citation6 respectively.
Bronchiectasis is characterized by mild to moderate airflow obstructionCitation7–Citation11 that tends to worsen over time.Citation12–Citation14 The most widely known model of the development of bronchiectasis is Cole’s “vicious cycle hypothesis”.Citation15 In this model, Cole proposed that an environmental insult often on a background of genetic susceptibility impaired muco-ciliary clearance resulting in persistence of microbes in the sinobronchial tree and microbial colonization. The microbial infection caused chronic inflammation resulting in tissue damage and impaired mucociliary motility. In turn this led to more infection with a cycle of progressive inflammation causing lung damage. The current view is that the two factors required for the development of this condition are persistent infection and a defect in host defense.
There are no well established animal models of bronchiectasis nor have there been studies performed in the early stages of the disease. Bronchiectasis is also a very heterogeneous condition and can be considered the end result of a variety of different factors. As a consequence the pathophysiologic processes are still not well defined. This review will discuss different aspects in which this condition may develop.
Pathology
Most studies of the pathology of bronchiectasis were reported between 1930 and 1960 as there was access to significant quantities of operative and postmortem lung specimens at this time. Reid categorized bronchiectasis as having three main phenotypes: 1) tubular characterized by smooth dilation of the bronchi; 2) varicose in which the bronchi are dilated with multiple indentations; and 3) cystic in which dilated bronchi terminate in blind ending sacs.Citation16 The current major form seen on HRCT is the tubular form of bronchiectasis. The CT appearance of these three different forms of bronchiectasis is demonstrated in .
Figure 1 HRCT examples of Reid’s three forms of bronchiectasis: A) tubular B), varicose, and C) cystic.
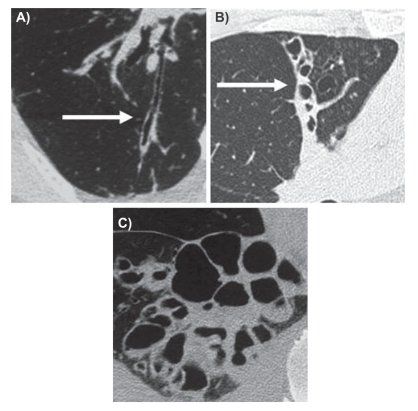
Arguably the most definitive study of the pathology of bronchiectasis was performed by WhitwellCitation17 who studied 200 consecutive operative lung specimens. This study demonstrated marked inflammation of the bronchial wall, principally in the smaller airways. Bronchial dilation was characterized by deficiency/loss of elastin and more advance disease by destruction of muscle and cartilage. The specific mechanism of how this loss of tissue leads to bronchial dilatation is not known. There was variable bronchial wall fibrosis, atelectasis and peribronchial pneumonic change. Whitwell classified bronchiectasis into three different types: follicular, saccular, and atelectatic. Follicular bronchiectasis was the dominant form and this corresponded to tubular bronchiectasis (the main form commonly seen).
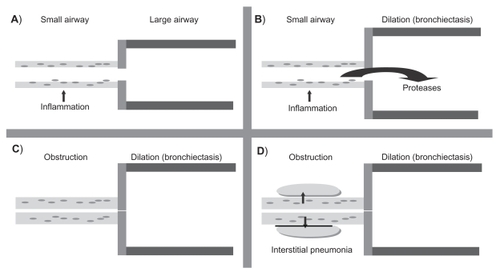
Follicular bronchiectasis was characterized by the presence of lymphoid follicles in the bronchial wall. The inflammatory process commenced in the small airway. This small airway inflammation caused the release of mediators such as proteases which damaged the large airways causing loss of elastin and other components such as muscle and cartilage which resulted in bronchial dilation. With progression of the disease lymphoid follicles enlarged in size and caused airflow obstruction to the small airways. The final event was spread of the inflammation beyond the airways to cause interstitial pneumonia. This process is demonstrated in . Recently Hogg and colleaguesCitation18 described similar lymphoid follicles in chronic obstructive pulmonary disease (COPD) which had a strong association with bronchial wall thickening and airflow obstruction.
Figure 2 Pathologic changes in follicular bronchiectasis as described by Whitwell. A) The first process involves infection of the small airways. B) This leads to the release of inflammatory mediators such as proteases which damage the large airways resulting in bronchial dilation and bronchiectasis. C) Infection drives progressive inflammation in the small airways which become thicker from a combination of cell-mediated inflammatory infiltrate and lymphoid follicles resulting in obstruction. D) The final process involves the spread of inflammation beyond the airways resulting in interstitial pneumonia.
The dominant cell types involved in the inflammatory process in bronchiectasis are neutrophils, lymphocytes, and macrophages.Citation19 Neutrophils are the most prominent cell type in the bronchial lumenCitation20,Citation21 and release mediators, particularly proteases/elastase which cause bronchial dilation (ie, bronchiectasis).Citation22,Citation23 The infiltrate in the cell wall is predominantly composed of macrophages and lymphocytes.Citation20,Citation24 Studies have reported that the main lymphocyte is the T cellCitation24,Citation25 and these are cells that are likely to produce the lymphoid follicles described by Whitwell.
Emphysema may also occur in bronchiectasis. Loubeyre and colleaguesCitation26 reported that half of a cohort of subjects had localized emphysema in association with bronchiectasis. This presumably corresponds to the interstitial pneumonia described by Whitwell that spreads into the parenchyma of the lungs to cause localized damage.
Distribution of bronchiectasis
The distribution of bronchiectasis may be associated with different pathophysiologic processes eg, allergic bronchopulmonary aspergillosis is classically associated with central bronchiectasis. Bronchiectasis has been described as being localized (ie, confined to one lobe) or generalized. Most commonly it is generalized and seems to be most common in the lower lobes.Citation2,Citation27 The involvement of the lower lobes may reflect gravity dependent retention of infected secretions.
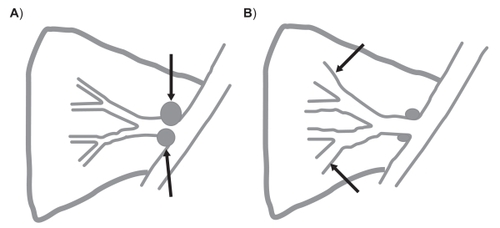
Right middle lobe bronchiectasis has been well described in the context of tuberculosis.Citation17,Citation28–Citation32 The right middle lobe bronchus is long, often bends sharply at its bifurcation and is of relatively small caliber. A collar of lymph nodes also surrounds the proximal bronchus and any condition that causes a prolonged enlargement of these nodes may lead to obstruction and secondary bronchiectasis. This may also occur in malignancyCitation33 and in nontuberculous mycobacterial infection (often with the lingula lobe).Citation34 This event is demonstrated in .
Figure 3 Pathologic process in the right middle lobe with mycobacterial infection. A) Infection causes enlargement of peribronchial lymph nodes resulting in obstruction. B) The obstruction results in bronchiectasis that persists when the nodes return to normal size.
It is generally not known if bronchiectasis starts in one section of the respiratory tract and then spreads or if it begins as a generalized process. Childhood bronchiectasis has a high proportion of subjects who have chronic rhinosinusitis as well.Citation10,Citation27,Citation35 One report described the apparent spread of sinus infection to the lungs resulting in bronchiectasis.Citation36
Lung function
A number of studies have described the lung function in bronchiectasis. Patients usually have mild to moderate air-flow obstruction. It has also been demonstrated recently that there is a progressive decline in lung function over time with loss of forced expiratory volume in one second (FEV1).Citation12–Citation14 This is a paradoxical finding as the characteristic feature of bronchiectasis is airway dilation.
A CT/lung function study found that airflow obstruction in bronchiectasis was predominantly due to small and medium airway involvement with features of decreased attenuation and mucosal wall thickening. The decreased attenuation was a marker of small airway constrictive bronchiolitis. The small airway constrictive bronchiolitis is diagnosed by the presence of a mosaic pattern on expiratory films.Citation37
The pathology studies by Whitwell explain the finding of airflow obstruction in bronchiectasis. These studies show the large airways become dilated but the small and medium airways are characterized by airflow obstruction predominantly arising from thickening of the bronchial wall. As most of the respiratory tree is composed of medium and small airways the net effect of the inflammatory process in bronchiectasis is airflow obstruction ().
Etiologic factors
There have been a large number of factors that have been described as causative for bronchiectasis. A problem with assigning these factors as being causative is that subjects have usually had their lung disease for a long time (often more than 10 years) and the attribution may rely on long-term retrospective recall. It may perhaps be more appropriate to consider them as risk factors rather than the definitive cause. The etiologic factors that have been described generally all have some role in impairing host defence to infection. Some important etiologic factors are discussed below. A list of etiologic factors is given in .
Table 1 Etiologic/risk factors associated with bronchiectasis
Postinfectious
The most common cause of bronchiectasis is the literature is postinfectious. This is not a well defined entity but the usual context appears to be one acute infectious episode which is thought to result in bronchiectasis. To the author’s knowledge, the development of bronchiectasis after one infectious episode have not been definitively demonstrated in a cohort of patients. At some stage all bronchiectasis patients become colonized with bacteria but this appears to be a little different from acute process in the postinfectious entity that is described in the literature. A possible mechanism for postinfectious bronchiectasis is a significant infection in early childhood which causes structural damage to the developing lung and permits bacterial infection which is not cleared. Over time persistent infection may then result in bronchiectasis.
One well characterized form of bronchiectasis occurs in the context of mycobacterial infection and this form is particularly prevalent in the right middle lobe with nontuberculous mycobacterium.Citation17,Citation38,Citation39 The mechanism of this form of bronchiectasis appears to arise from lymph node obstruction. The acute infection causes enlargement of peribronchial nodes which obstruct the bronchus and result in secondary bronchiectasis. This bronchial dilation persists when the mycobacterial infection resolves and the nodes return to normal size. This process is demonstrated in .
Muco-ciliary clearance
Muco-ciliary clearance is a key defence mechanism against pulmonary infection. Its compromise is important in the development of the vicious cycle of bronchiectasis as proposed by Cole.Citation15 Cystic fibrosis is associated with defective muco-ciliary clearance but this area is beyond the scope of the current review. There has been renewed interest recently in ciliary defects and this has been recently reviewed.Citation40–Citation42 The most prominent cilial disorder is primary ciliary dyskinesia (PCD) which combines upper and lower respiratory tract infection, male infertility and in approximately 50%, situs inversus. PCD arises primarily from a defect in the dynein arms which are necessary for normal cilial beating. This area has been the subject of recent discoveries.Citation43,Citation44 Bronchiectasis is a prominent manifestation of PCD. The definitive diagnosis of PCD requires electron microscopy to demonstrate loss of dynein and this requires specialized expertise available only in a limited number of centers. Screening can be undertaken more easily using nasal nitric oxide and in vivo tests of ciliary motility such as the saccharin test. Young’s syndrome is another condition in which the primary defect is thought to be defective mucous function.Citation45
Malnutrition/socioeconomic
Bronchiectasis has been described as being a major problem in developing nations although the prevalence has not been well defined. Authors from South America,Citation46 Hong Kong/China,Citation47 India,Citation48 and TurkeyCitation49 all report that bronchiectasis is an important local problem. It is certainly a major problem in certain indigenous populations such as Australian aborigines, New Zealand Maori, and Alaskan natives.Citation50–Citation52 A common feature of these groups is malnutrition and social disadvantage which are likely to be associated with impaired immune function (Torzillo and Chang, pers comm.).Citation53 Malnutrition/socioeconomic disadvantage is not commonly listed as an etiologic factor for bronchiectasis, but in selected populations it may be important.
Extremes of age
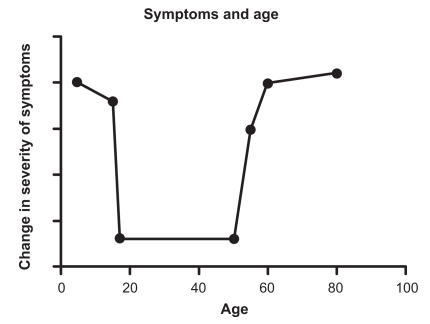
The immune system is less effective in young children and elderly adults which results in an increased incidence of infection in these two groups.Citation54,Citation55 Bronchiectasis has most commonly been described as commencing in childhood, particularly in the first five years of life, with chronic productive cough and unresolved infection.Citation2,Citation10,Citation27 Field performed a long-term prospective follow-up on 225 patients with bronchoscopy. She found that 74% of the cohort had the onset of chronic respiratory infection in the first five years of life and subjects tended to significantly improve in late adolescence regardless of treatment.Citation27 Our group has studied adult patients with bronchiectasis who had the onset of symptoms in childhood.Citation2 Most of these subjects (about two-thirds) described the improvement of their symptoms in late adolescence and then a worsening of their symptoms from the age of 50 to 60 years when they represented for medical assessment. These two studies suggest that a common feature of childhood-onset bronchiectasis may be an improvement with adulthood and then clinical deterioration again beyond the age of 50 years. This is shown in .
Figure 4 Change in severity of symptoms over time in those with childhood-onset bronchiectasis. A common finding in subjects whose symptoms began in childhood is improvement in late adolescence and then deterioration again from about the age of 50 years.
We have also described the phenotype of patients who first develop bronchiectasis in adulthood.Citation35 The onset of chronic chest suppuration cough was uncommon from the ages of 15–50 years. Eighty-one percent of adult-onset patients had the onset of chronic chest suppuration over the age of 50 years. Weycker and colleauges report a prevalence of bronchiectasis as being 4.2 per 100,000 persons aged 18 to 34 years and 272 per 100,000 in those aged over 75 years.Citation4 Therefore extremes of age may be important in the development and clinical manifestations of bronchiectasis. Increasing age has been recently described as being an important factor in COPD.Citation56
Chronic obstructive pulmonary disease
A cardinal feature of COPD is the presence of chronic bronchitis. Recently two studies have reported a high incidence of bronchiectasis in COPD patients. O’Brien and colleaguesCitation5 studied 110 patients with COPD who presented with an acute exacerbation in a primary care setting and found HRCT evidence of bronchiectasis in 29% of the cohort. Patel and colleaguesCitation6 studied 54 patients with severe COPD for the presence of bronchiectasis. They found that 50% of the patients had co-existent bronchiectasis and this was associated with bacterial airway colonization and inflammatory markers and longer duration of exacerbations.Citation6 Patients with COPD and bronchiectasis tend to have more dyspnea, worse lung function, and a lack of upper airway involvement when compared to other bronchiectasis subjects.Citation35
There is also some overlap in the pathology of COPD and bronchiectasis. Both conditions have neutrophils and T lymphocytes as the predominant inflammatory cell,Citation19,Citation57 protease release causes pulmonary damage and lymphoid follicles have a role in airflow obstruction.Citation17,Citation18
Immune dysfunction
The term immune dysfunction covers a wide variety of causes but some conditions associated with bronchiectasis are primarily categorized as immune dysfunction disorders. These can be considered in terms of primary immune deficiencies such as hypogammaglobulinemia, human immunodeficiency virus (HIV), interferon gamma receptor deficiency, and type I major histocompatibility complex deficiency.Citation2 Detection of hypogammaglobulinemia is important as replacement therapy may have therapeutic implications. The clinical significance of immunoglobulin subclass deficiency is controversial.
Bronchiectasis may occur in the late stages of lung transplant rejection. Allergic bronchopulmonary aspergillosis (ABPA) is a classic cause of bronchiectasis and this is important to diagnose as there are specific ramifications for treatment. Bronchiectasis may also occur in subjects with very high levels of immunoglobulin E but without ABPA.Citation36
Mycobacterial infections have been recognized to be associated with bronchiectasis, particularly in older women where the combination of mycobacterium avium complex (MAC) infections causing obstruction from lymphad-enopathy with right middle lobe bronchiectasis is a well described syndrome.Citation58,Citation59 It should also be remembered that MAC infections are opportunistic and may cause infection in other chronic lung diseases such as COPD and therefore infection with MAC may be secondary to bronchiectasis. It is not clear from the literature what the effect of secondary MAC colonization is on the progression of bronchiectasis. In four children who had disseminated mycobacterial infection, researchers recently found a mutation defect in the gene for interferon gamma receptor, the primary protective cytokine against intracellular mycobacterial infection.Citation60
Rheumatological/inflammatory conditions
There is a well described association between bronchiectasis and rheumatoid arthritis. In rheumatoid arthritis the incidence of bronchiectasis has been described to be 1%–3%. Recent studies of patients with rheumatoid arthritis have described the prevalence of bronchiectasis on HRCT in such patients as being up to 30%.Citation61,Citation62 Bronchiectasis is described as preceding and occurring after the development of rheumatoid arthritis. Bronchiectasis may also occur in association with Sjogren’s syndromeCitation63 and Churg–Strauss syndrome.Citation64 It is possible that immune suppression may predispose to chronic airway infection.Citation64 Bronchiectasis also occurs in subjects with inflammatory bowel disease.Citation65
Alpha1-antitrypsin deficiency
Alpha1-antitrypsin deficiency (AAT) is associated with increased risk of COPD and bronchiectasis. Parr and colleagues studied the prevalence of airways disease in AAT-deficient subjects and found that 70 of 74 subjects had radiological evidence of bronchiectasis and 20 subjects were classified as having clinically significant bronchiectasis.Citation66
Microbiology
A large number of different pathogens have been isolated in studies of microbiologic flora in bronchiectasis. There is often significant variation between different locations. The main findings from recent studies have been that Haemophilus influenzae is the most common pathogen (range 29%–70%) followed by Pseudomonas aeruginosa (range 12%–31%).Citation7,Citation10,Citation67–Citation71 The other major finding of these studies is that 30%–40% of sputum samples despite being good quality and purulent will fail to grow any pathogenic bacteria; and this applies even when bronchoscopy and protected brush/bronchoalveolar lavage is used. The bronchi also have a dynamic turnover of pathogens. A two-year prospective study found that a proportion of patients were continually colonized by Branhamella catarrhalis (the name Branhamella has recently been changed to Moxarella) but there was a continous turnover of strains every 2–3 months.Citation72 In COPD, there is evidence for considerable turnover of bacteria with the acquisition of new strains demonstrated to be associated with exacerbations.Citation73
An important finding of bronchiectasis is that there appears to be a change in microbial flora with severity of disease.Citation71 Typically subjects with the best preserved lung function are most likely to have no pathogenic bacteria isolated. As lung function declines H. influenzae becomes predominant and finally in patients with the most severe disease the usual pathogen isolated is P. aeruginosa.
Specific pathogens
H. influenzae is the most common isolate and is nearly always the nontypeable form (NTHi). P. aeruginosa is associated with more sputum, more extensive bronchiectasis, more hospitalizations and worse quality of life. Nontuberculous mycobacterial infection may be important in bronchiectasis but studies have reported variable prevalence of 2%Citation71,Citation74 to 10%.Citation75
The role of viral infection in bronchiectasis is not well defined. BecroftCitation76 identified adenovirus as a risk factor for the development of bronchiectasis in young children. Influenzae A infection in vitro inhibits neutrophil function in bronchiectasis subjects.Citation77 Viral infections have a role in exacerbations of COPD but this has not been defined for bronchiectasis.Citation78
Effects of bacterial pathogens on the respiratory tract
Bacterial pathogens may exert a number of direct effects on the respiratory tract that impairs host defence. The most well described effects in bronchiectasis are inhibition of the mucociliary clearance. Mediators released by H. influenzae, P. aeruginosa, and Streptococcus pneumoniae may directly interfere with ciliary function, damage ciliated epithelium, and inhibit mucous transport.Citation79 Bacteria release products such as glycoproteins which attract neutrophils. H. influenzae has the capacity to cause direct damage to airway epithelium and is also able to invade into the bronchial wall and interstitium of the lung.Citation80,Citation81 P. aeruginosa has the capacity to form biofilms.Citation82 Biofilms occur particularly in advanced disease and form an impenetrable matrix around the Pseudomonas, shielding it from the effects of the immune system and antibiotics and allowing the bacterial infection to cause severe damage to the underlying lung.
Conclusions
Bronchiectasis is characterized by airway inflammation. The inflammation appears to arise as a combination of immune deficiency and persistent infection. As proposed by Cole this inflammatory process is progressive and results in a cycle of worsening pulmonary damage. Patients develop progressive obstructive lung disease. The airflow obstruction appears to arise predominantly from involvement of the small airways in which the bronchial wall is infiltrated by inflammatory cells particularly lymphocytes which may form lymphoid follicles.
Bronchiectasis is a heterogeneous condition and there are a large number of etiologic factors have been described. Because of the long-term nature of the disease it is often hard to be clear about the exact role of such factors in the pathogenesis. It may be more appropriate to consider them as being risk factors rather than the single cause of longstanding airway infection.
The microbiology of bronchiectasis is complex and varies significantly between different studies. An important finding is that despite purulent sputum and optimal collection techniques (eg, bronchoscopy) there is often failure to isolate a pathogenic microorganism. The role of viruses is not well understood. A better understanding of the microbiology of bronchiectasis would have direct implications for patient treatment.
Bronchiectasis is a complex condition and the pathophysiology is still not well understood. Defining the inflammatory process particularly before there is significant lung disease may be helpful in developing better strategies of treatment.
Acknowledgments
The author would like to thank Associate Professor Peter Holmes and Professor Stephen Holdsworth for their help with this work. The author reports no conflicts of interest in this work.
References
- BarkerAFBronchiectasisN Engl J Med20023461383139311986413
- KingPTHoldsworthSRFreezerNJVillanuevaEHolmesPWCharacterisation of the onset and presenting clinical features of adult bronchiectasisRespir Med20061002183218916650970
- McGuinnessGNaidichDPCT of airways disease and bronchiectasisRadiol Clin North Am20024011911813813
- WeyckerDEdelsbergJOsterGTinoGPrevalence and economic burden of bronchiectasisClin Pulm Med20054205209
- O’BrienCGuestPJHillSLStockleyRAPhysiological and radiological characterisation of patients diagnosed with chronic obstructive pulmonary disease in primary careThorax20005563564210899238
- PatelISVlahosIWilkinsonTMBronchiectasis, exacerbation indices, and inflammation in chronic obstructive pulmonary diseaseAm J Respir Crit Care Med200417040040715130905
- NicotraMBRiveraMDaleAMShepherdRCarterRClinical, pathophysiologic, and microbiologic characterization of bronchiectasis in an aging cohortChest19951089559617555168
- WilsonCBJonesPWO’LearyCJColePJWilsonRValidation of the St. George’s Respiratory Questionnaire in bronchiectasisAm J Respir Crit Care Med19971565365419279236
- O’DonnellAEBarkerAFIlowiteJSFickRBTreatment of idiopathic bronchiectasis with aerosolized recombinant human DNase I. rhDNase Study GroupChest1998113132913349596315
- PasteurMCHelliwellSMHoughtonSJAn investigation into causative factors in patients with bronchiectasisAm J Respir Crit Care Med20001621277128411029331
- AngrillJAgustiCDe CelisRBronchial inflammation and colonization in patients with clinically stable bronchiectasisAm J Respir Crit Care Med20011641628163211719301
- KingPTHoldsworthSRFreezerNJVillanuevaEGallagherMHolmesPWOutcome in Adult BronchiectasisCOPD: Journal of Chronic Obstructive Pulmonary Diseases200522734
- TwissJStewartAWByrnesCALongitudinal pulmonary function of childhood bronchiectasis and comparison with cystic fibrosisThoraxi200661414418
- Martinez-GarciaMASoler-CatalunaJJPerpina-TorderaMRoman-SanchezPSorianoJFactors associated with lung function decline in adult patients with stable non-cystic fibrosis bronchiectasisChest20071321565157217998359
- ColePJInflammation: a two-edged sword – the model of bronchiectasisEur J Respir Dis Suppl19861476153533593
- ReidLReduction in bronchial subdivisions in bronchiectasisThorax19505223247
- WhitwellFA study of the pathology and pathogenesis of bronchiectasisThorax1952721321912984409
- HoggJCChuFUtokaparchSThe nature of small-airway obstruction in chronic obstructive pulmonary diseaseN Engl J Med20043502645265315215480
- FuschilloSDe FeliceABalzanoGMucosal inflammation in idiopathic bronchiectasis: cellular and molecular mechanismsEur Respir J20083139640618238949
- EllerJLapa e SilvaJRPoulterLWLodeHColePJCells and cytokines in chronic bronchial infectionAnn N Y Acad Sci19947253313458031005
- LoukidesSBourosDPapatheodorouGLachanisSPanagouPSiafakasNMExhaled H2O2 in steady-state bronchiectasis: relationship with cellular composition in induced sputum, spirometry, and extent and severity of diseaseChest2002121818711796435
- KhairOADaviesRJDevaliaJLBacterial-induced release of inflammatory mediators by bronchial epithelial cellsEur Respir J19969191319228880112
- ZhengLTipoeGLamWKUp-regulation of circulating adhesion molecules in bronchiectasisEur Respir J20001669169611106214
- Lapa e SilvaJRGuerreiroDNobleBPoulterLWColePJImmunopathology of experimental bronchiectasisAm J Respir Cell Mol Biol198912973042696517
- GagaMBentleyAMHumbertMIncreases in CD4+ T lymphocytes, macrophages, neutrophils and interleukin 8 positive cells in the airways of patients with bronchiectasisThorax1998536856919828857
- LoubeyrePParetMRevelDWiesendangerTBruneJThin-section CT detection of emphysema associated with bronchiectasis and correlation with pulmonary function testsChest19961093603658620706
- FieldEBronchiectasis: a long-term follow-up of medical and surgical cases from childhoodArch Dis Child19613658760313892759
- GrahamEABurfordTHMayerTHMiddle lobe syndromePostgrad Med194842918874043
- BrockRCPost-tuberculosis broncho-stenosis and bronchiectasis of the middle lobeThorax19505511
- FretheimBThe so-called middle lobe syndromeThorax1952715615814931380
- AlboRJGrimesOFThe middle lobe syndrome: a clinical studyDis Chest1966505095185953791
- BombardaSFigueiredoCMSeiscentoMTerra FilhoMPulmonary tuberculosis: tomographic evaluation in the active and post-treatment phasesSao Paulo Med J200312119820214666291
- BertelsenSStruve-ChristensenEAastedASparupJIsolated middle lobe atelectasis: aetiology, pathogenesis, and treatment of the so-called middle lobe syndromeThorax1980354494527434301
- LevinDLRadiology of pulmonary Mycobacterium avium-intracellulare complexClin Chest Med20022360361212370996
- KingPTHoldsworthSFarmerMWFreezerNVillanuevaEHolmesPPhenotypes of bronchiectasis: onset of productive cough in childhood and adulthoodCOPD2009613013619378226
- KingPBronchiectasis and chronic rhinosinusitisRespir Med CME20081284285
- RobertsHRWellsAUMilneDGAirflow obstruction in bronchiectasis: correlation between computed tomography features and pulmonary function testsThorax20005519820410679538
- LynchDASimonePMFoxMABucherBLHeinigMJCT features of pulmonary Mycobacterium avium complex infectionJ Comput Assist Tomogr1995193533607790541
- FujitaJRadiological findings of non-tuberculous mycobacteria respiratory infectionKekkaku20037855756114509228
- BushAChodhariRCollinsNPrimary ciliary dyskinesia: current state of the artArch Dis Child2007921136114017634184
- EscudierEDuquesnoyPPaponJFAmselemSCiliary defects and genetics of primary ciliary dyskinesiaPaediatr Respir Rev200910515419410201
- HoggCPrimary ciliary dyskinesia: when to suspect the diagnosis and how to confirm itPaediatr Respir Rev200910445019410200
- OmranHKobayashiDOlbrichHKtu/PF13 is required for cytoplasmic pre-assembly of axonemal dyneinsNature200845661161619052621
- ColantonioJRVermotJWuDThe dynein regulatory complex is required for ciliary motility and otolith biogenesis in the inner earNature200945720520919043402
- FriedmanKJTeichtahlHDe KretserDMScreening Young syndrome patients for CFTR mutationsAm J Respir Crit Care Med1995152135313577551394
- MarosticaPJFischerGBNon-cystic-fibrosis bronchiectasis: a perspective from South AmericaPaediatr Respir Rev2006727528017098642
- TsangKWTipoeGLBronchiectasis: not an orphan disease in the EastInt J Tuberc Lung Dis2004869170215182138
- SethiGRBatraVBronchiectasis: causes and managementIndian J Pediatr20006713313910832241
- KaradagBKarakocFErsuRKutABakacSDagliENon-cystic-fibrosis bronchiectasis in children: a persisting problem in developing countriesRespiration20057223323815942290
- SingletonRMorrisAReddingGBronchiectasis in Alaska Native children: causes and clinical coursesPediatr Pulmonol20002918218710686038
- ChangABGrimwoodKMulhollandEKTorzilloPJBronchiectasis in indigenous children in remote Australian communitiesMed J Aust200217720020412175325
- TwissJMetcalfeREdwardsEByrnesCNew Zealand national incidence of bronchiectasis “too high” for a developed countryArch Dis Child20059073774015871981
- ChinenJShearerWT6. Secondary immunodeficiencies, including HIV infectionJ Allergy Clin Immunol2008121S388S392 quiz S41718241688
- EnglishBKSchroederHWWilsonCBRichRRFleisherTAShearerWTKotzinBLSchroederHWImmaturity of the fetal and neonatal immune systemClinical Immunology, Principles and PracticeLondon, UKMosby200140.1040.41
- WekslerMESzaboPRichRRFleicherTAShearerWTKotzinBLSchroederHWAging and the immune systemClinical Immunology; Principles and PracticeLondon, UKMosby200141.4148
- ShahabLJarvisMJBrittonJWestRPrevalence, diagnosis and relation to tobacco dependence of chronic obstructive pulmonary disease in a nationally representative population sampleThorax2006611043104717040932
- BarnesPJChronic obstructive pulmonary diseaseN Engl J Med200034326928010911010
- WagnerRBJohnstonMRMiddle lobe syndromeAnn Thorac Surg1983356796866344820
- De BoeckKWillemsTVan GyselDCorbeelLEeckelsROutcome after right middle lobe syndromeChest19951081501527606950
- NewportMJHuxleyCMHustonSA mutation in the interferon-gamma-receptor gene and susceptibility to mycobacterial infectionN Engl J Med1996335194119498960473
- CortetBFlipoRMRemy-JardinMUse of high resolution computed tomography of the lungs in patients with rheumatoid arthritisAnn Rheum Dis1995548158197492220
- HassanWUKeaneyNPHollandCDKellyCAHigh resolution computed tomography of the lung in lifelong non-smoking patients with rheumatoid arthritisAnn Rheum Dis1995543083107763110
- LarcheMJA short review of the pathogenesis of Sjogren’s syndromeAutoimmun Rev2006513213516431344
- KingPChurgh-Strauss syndrome and bronchiectasisRespir Med Extra200732628
- BlackHMendozaMMurinSThoracic manifestations of inflammatory bowel diseaseChest200713152453217296657
- ParrDGGuestPGReynoldsJHDowsonLJStockleyRAPrevalence and impact of bronchiectasis in alpha1-antitrypsin deficiencyAm J Respir Crit Care Med20071761215122117872489
- RobertsDEColePUse of selective media in bacteriological investigation of patients with chronic suppurative respiratory infectionLancet198017967976102681
- PangJChanHSSungJYPrevalence of asthma, atopy, and bronchial hyperreactivity in bronchiectasis: a controlled studyThorax1989449489512595637
- HoPLChanKNIpMSThe effect of Pseudomonas aeruginosa infection on clinical parameters in steady-state bronchiectasisChest1998114159415989872194
- AngrillJAgustiCde CelisRBacterial colonisation in patients with bronchiectasis: microbiological pattern and risk factorsThorax200257151911809984
- KingPTHoldsworthSRFreezerNJVillanuevaEHolmesPWMicrobiologic follow-up study in adult bronchiectasisRespir Med20071011633163817467966
- KlingmanKLPyeAMurphyTFHillSLDynamics of respiratory tract colonization by Branhamella catarrhalis in bronchiectasisAm J Respir Crit Care Med1995152107210787663786
- SethiSEvansNGrantBJMurphyTFNew strains of bacteria and exacerbations of chronic obstructive pulmonary diseaseN Engl J Med200234746547112181400
- WickremasingheMOzerovitchLJDaviesGNon-tuberculous mycobacteria in patients with bronchiectasisThorax2005601045105116227333
- FowlerSJFrenchJScreatonNJNontuberculous mycobacteria in bronchiectasis: Prevalence and patient characteristicsEur Respir J2006281204121016807259
- BecroftDMBronchiolitis obliterans, bronchiectasis, and other sequelae of adenovirus type 21 infection in young childrenJ Clin Pathol19712472824324685
- PangGClancyRCongMOrtegaMZhigangRReevesGInfluenza virus inhibits lysozyme secretion by sputum neutrophils in subjects with chronic bronchial sepsisAm J Respir Crit Care Med200016171872210712313
- SeemungalTHarper-OwenRBhowmikARespiratory viruses, symptoms, and inflammatory markers in acute exacerbations and stable chronic obstructive pulmonary diseaseAm J Respir Crit Care Med20011641618162311719299
- WilsonRColePJThe effect of bacterial products on ciliary functionAm Rev Respir Dis1988138S49S533202522
- MollerLVTimensWvan der BijWHaemophilus influenzae in lung explants of patients with end-stage pulmonary diseaseAm J Respir Crit Care Med19981579509569517616
- BandiVApicellaMAMasonENontypeable haemophilus influenzae in the lower respiratory tract of patients with chronic bronchitisAm J Respir Crit Care Med20011642114211911739144
- DaviesJCBiltonDBugs, biofilms, and resistance in cystic fibrosisRespir Care20095462864019393107