Abstract
Background
The six-minute walking distance (6MWD) test has demonstrated validity and reliability to assess changes in functional capacity following pulmonary rehabilitation in patients with chronic obstructive lung disease. However, no attempt has been made to establish an iterative measurement of 6MWD during the overall period of pulmonary rehabilitation. Therefore, the aim of this study was to evaluate the impact of a twelve-week rehabilitation program on the iterative weekly measurement of 6MWD in chronic obstructive pulmonary disease (COPD) patients and healthy subjects.
Methods
Twenty-six patients with COPD and nine age-matched healthy subjects were studied. Measurements were taken at baseline and after twelve weeks except for the 6MWD. The exercise measurements included a six-minute walking test (6MWT) and an incremental exercise test. Oxygen saturation, heart rate, and dyspnea will be monitored during all these tests.
Results
At baseline there were significant differences between groups, except in age, body mass index, and oxygen saturation. After 12 weeks, there was no significant change in lung function in patients with COPD and healthy subjects. The 6MWD, peak oxygen uptake V̇O2peak and anaerobic threshold increased significantly after training in both groups (P < 0.01). The averaged trace of the 6MWD of patients with COPD and healthy subjects was followed-up respectively by a logarithmic and linear fitting. 6MWD showed a plateau after eight weeks in patients with COPD, however, it increased continually overall in healthy subjects.
Conclusion
Both patients with COPD and healthy subjects demonstrated functional responses to training but with somewhat different patterns in quality of the improvement of the 6MWD.
Chronic obstructive pulmonary disease (COPD), characterized by chronic inflammation with irreversible airflow limitation, causes chronic morbidity and disability. COPD is predicted to be the fifth most frequent cause of death in the world.Citation1 Dyspnea, decrease of exercise capacity, and impairment of quality of life are common in patients with COPD.Citation2 Recently, it has been demonstrated that the decrease in exercise capacity is associated with mortality of these patients.Citation1,Citation2 Patients with COPD often report walking slower than people of the same age, having to stop walking to breathe, or not leaving the house because of breathlessness.Citation3
Pulmonary rehabilitation is strongly endorsed as an evidence-based intervention for the management of patients with COPD.Citation2 It is the recommended standard of care for patients with COPD as it has been shown to decrease the perception of dyspnea,Citation4 to enhance exercise capacity,Citation5 to reduce health care resource utilizationCitation5,Citation6 and to improve health status.Citation4 Reduction of lactic acidosis,Citation7 reduction in minute ventilation and heart rate for a given work rate and enhanced activity of mitochondrial enzymes and improved capillary density in the trained muscles,Citation8,Citation9 are among the underlying physiological changes that contribute to these improvements.
Timed walking tests such as the six-minute walking test (6MWT) have gained popularity for use in clinical practice and research settingCitation10–Citation12 to assess changes in functional capacity following pulmonary rehabilitation intervention.Citation11 Previous studies using the 6MWT were conducted in patients with COPD, but did not include healthy subjects.Citation13,Citation14
The aim of this study was to evaluate the impact of a twelve-week rehabilitation program on the iterative measurement of six-minute walking distance (6MWD) in COPD patients and healthy subjects.
Methods
Study subject
The study has been approved by the Ethical Committee of the University Hospital of Sousse. Thirty-two patients from the department of physiology of the Academic Hospital of Sousse, Tunisia, who had been diagnosed with moderate to severe COPD and twelve healthy subjects, were included in the study after giving their informed consent to participate. Diagnosis of COPD was made according to international recommendations.Citation1 At the start of the study, patients were clinically stable; they received regular treatment with inhaled bronchodilators and inhaled steroids according to current guideline for their disease stage. Patients with a significant response following bronchodilator use, defined as an increase in forced expiratory volume in one second (FEV1) of more than 12% and 200 mL, patients with congestive heart failure, ischemic heart disease, or neuromuscular problems; and patients who had participated in an earlier training program, were excluded from the study.
The healthy subjects were all nonsmokers and free of significant cardiovascular, metabolic, and musculoskeletal disorders that could limit exercise capacity.
Study design
Subjects were evaluated on three consecutive days at baseline and at the end of the three months training program. On the first day of the study, patients were informed of the purpose of the study and had agreed to participate. Pulmonary function test was performed using a body plethysmograph. On the second day a 6MWT test was performed. On the third day, the exercise capacity was assessed by using a cycle ergometer.
Methods
Pulmonary function test
All participants underwent spirometry with determination of FEV1 and forced vital capacity (FVC). Spirometry was performed using the pneumotachograph of a constant volume plethysmograph (ZAN 500 Body II; ZAN Meßgreräte GmbH, Germany) according to European Respiratory Society recommendations.Citation15
Exercise testing
Subjects were evaluated before and after rehabilitation program. An exercise test was performed on a calibrated cycle ergometer (Ergoline, Bitz, Germany) according to the individualized and standardized exercise test protocol reported by the American Thoracic Society and American College of Chest Physicians.Citation16 The maximal predicted work load was calculated and adapted to the patient by multiplication of the percentage fall in FEV1 by comparison to the predicted value.
Prior to each experiment, the volume and the gas analysers were calibrated. The theoretical maximal oxygen uptake (V̇O2max Th) was calculated.Citation16 Subject wore a mask for gas exchange analysis using a breath-by-breath automated exercise metabolic system (ZAN 600 Ergotest; ZAN Meßgeräte GmbH). The three-minute warm-up was conducted at 20% of this maximal estimated workload. The workload was then increased every minute. The rate of increase was defined as 8% of maximal estimated workload, in order to obtain the maximal workload in about 10 minutes.
Oxygen saturation (SO2) was continuously monitored via a finger pulse oxymeter (Model 9847 Nonin Medical, Inc.; Minneapolis, MN, USA). Systolic blood pressure and dyspnea (Borg CR-10 scale) were recorded before and after exercise. The heart rate was continuously monitored using a 12-lead ECG (ZAN ECG, 800; ZAN Meßgeräte GmbH).
To ensure that peak oxygen uptake (V̇O2peak) was attained, at least three of the following criteria had to be met: an increase in V̇O2 < 5 mL with the last increase in work rate; attainment of age predicted maximal cardiac frequency; a respiratory exchange ratio >1.10 and an inability to maintain the required pedaling frequency (60 rev min−1) despite maximal effort and verbal encouragement. V̇O2peak was accepted as maximum V̇O2. The anaerobic threshold was determined by the V-slope method and confirmed by the traditional gas exchange.Citation17
Six-minute walking test
The 6MWT was performed before and every week during the three months of the rehabilitation program. The 6MWT was conducted according to international recommendations.Citation10 Reference values were calculated by Tunisian equations.Citation18 Subjects were instructed to walk at their own maximal pace along a 40 m long hospital corridor. They were asked to cover as much distance as they could within six minutes. Subjects were given feedback on time progression at each minute. Subjects were allowed to stop and rest during the test, but were instructed to resume walking as soon as they felt able to do so. Before the test, patients rested in a chair, located near the starting position, for ≥10 minutes. Heart rate and SO2 were measured for one minute at baseline, and during the first minute of recovery by a pulse oxymeter. Pre- and post-walk dyspnea was recorded using the Borg scale. At the end of the 6MWT, the participant was told to stop, and ambulatory distance was recorded.
Training program
The subjects were required to participate in the rehabilitation program three days/week during the three months. They received the same exercise training and education program. This consisted of two sessions of 30 minutes/week of seminars and discussions covering the following topics: relaxation, disease education, benefits advice, energy conversation, medication advice, chest clearance, and breathing control techniques. The training schedule was the same in the two groups, consisting of a five minute warm-up followed by 10 minutes of work and five minutes of active recovery, repeated over a 45 minute session. The exercise program was individualized according to the initial physical fitness assessment before intervention. Each subject was trained to its target heart rate corresponding to the gas exchange threshold. Subjects were instructed to perform a stationary bicycle exercise and the warm-up, cool-down, and upper extremity exercises. During training, heart rate was continuously monitored by means of a cardiofrequency meter (Polar, S810). The cardiofrequency meter was set in such a way that subject could exercise within ± 5 beats/minute of prescribed intensity. An alarm insured that the subject trained within the preselected range.
Analysis
The results of the study are presented as mean ± standard deviation (SD). The nonparametric Mann–Whitney U test was used to compare baseline characteristics and training-related changes in patients with COPD and healthy subjects, Wilcoxon’s matched pairs test was used to assess training-induced changes within the group. Repeated measures ANOVA was used to assess weekly changes of 6MWD overall of pulmonary rehabilitation. When the ANOVA F ratio was significant, the means were compared by using the post-hoc contrast test. The statistical program Statistica was used for the analysis (Statistica Kernel Version 6; Stat Soft, France). The level of significance was set as P < 0.05.
Results
Six patients and three healthy subjects were dropped out of the rehabilitation group due to an acute exacerbation of respiratory symptoms and lack of motivation or transport problems.
Anthropometric characteristics and pulmonary function parameters of patients with COPD and healthy subjects before and after the rehabilitation program are provided in . Age and body mass index (BMI) were similar in both groups. The main differences were observed in pulmonary function where the patients with COPD showed moderate to very severe airflow obstruction. There was no significant change in FEV1 and FVC in the two groups after rehabilitation program.
Table 1 Anthropometric characteristics and pulmonary function parameters of healthy subjects and patients with chronic obstructive pulmonary disease before and after rehabilitation program
shows exercise characteristics of patients with COPD and healthy subjects before and after the rehabilitation program. There are significant changes in V̇O2peak, the anaerobic threshold, dyspnea, and heart rate (P < 0.01). The SO2 did not change significantly after rehabilitation program in both groups.
Table 2 Exercise characteristics of healthy subjects and patients with chronic obstructive pulmonary disease before and after rehabilitation program
The 6MWD increased significantly after the rehabilitation program in both groups (P < 0.01), as shown in . The dyspnea and heart rate at the peak of 6MWT decreased significantly after the rehabilitation program (P < 0.05). Any change in SO2% was marked at the peak of 6MWT in both groups compared with values before rehabilitation program.
Table 3 Six-minute walking test parameters of healthy subjects and patients with chronic obstructive pulmonary disease before and after rehabilitation program
shows the averaged trace and the corresponding logarithmic and linear fitting of the dependant variables of 6MWD for patients with COPD and healthy subjects.
Figure 1 Logarithmic and linear fitting of the dependant variables for patients with COPD (–♦–) and healthy subjects (---▴---).
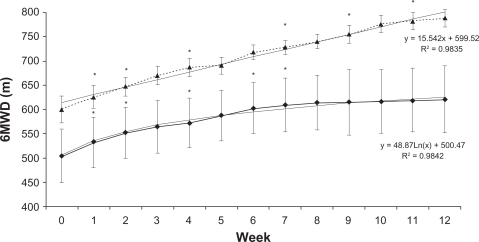
The average walking distance of both groups increased significantly during the first week of training (P < 0.05), and within two weeks all the subjects showed an increase in 6MWD. The mean walking distance in COPD patients increased according to a logarithmic curve (r = 0.98). The walking distance in healthy subjects increased linearly during the overall period of training (r = 0.98). However, in patients with COPD, it continued to improve and reaching 613.91 ± 56.06 m after eight weeks, after that the mean distance showed little change which presented as a plateau. On the last evaluation, the mean walking distance was 620.73 ± 69.71 m. However, the walking distance of healthy subjects increased continually overall period of the rehabilitation program.
Discussion
The aim of this study was to evaluate the impact of 12 weeks, rehabilitation program on the iterative measurement of 6MWD in COPD patients and healthy subjects.
The major finding of this study was that, for comparable training conditions and duration, while patients with COPD and healthy subjects presented a distinct 6MWD response during endurance training, these responses differed quantitatively and qualitatively.
Quantitatively, the increase of 6MWD was significantly higher in controls than patients with COPD. From a qualitative point of view, physical training induces, in COPD patients, a logarithmic increase of 6MWD. Whereas, healthy controls showed a linear increase in the same period of training.
Assessment of cardiopulmonary function and V̇O2peak during exercise stress reveals valuable insights with respect to the disease process and limitations imposed.Citation17 Exercise training programs were individualized. They were adapted to the individual limitations of the patient, taking cardiovascular, pulmonary, and skeletal muscle limitations into account and can be demonstrated to show overall benefit for each patient.Citation19
As demonstrated in other studies,Citation7 no significant modification of pulmonary function was marked after a training program. Indeed, respiratory muscles are affected by multiple factors related to both the presence and severity of COPD which may impair their structure and function.Citation20 Pulmonary rehabilitation causes modification in peripheral myopathy but not ventilator limitation. The airflow limitation in most cases is both progressive and associated with an abnormal inflammatory response of the lungs to noxious particles or gases.Citation19
The effect of individualized training on dyspnea peak and the maximal heart rate after 6MWT and exercise test, after rehabilitation program, was significantly important in both groups. This could be explained, firstly by improved physical conditions and a very good response to exercise, which supports a decreased sensation of dyspnea.Citation21 Secondly, by some physiological changes, like better cardiac adaptation, decrease in lactic acid production and reduction in metabolic cost of exercise.Citation7 This also explains the significant improvement of V̇O2peak (13%) for patients with COPD. This result was similar to some studies which showed 10% improvement of V̇O2peakCitation20 and differs from other studies which showed 20% improvement.Citation22 This difference could be due to the variation in the length of training periods or to the intensity of training.
Compared to the healthy controls, COPD patients had significantly less walking distance during 6MWT. The magnitude of the overall increase in walking distance is in agreement with previous findings.Citation23 In our study, patients showed a mean increase in the 6MWT of 117 m or 23% in COPD patients and of 189 m in healthy subjects or 32% after 12 weeks. The percentage of walking distance improvement in patients with COPD was similar to those reported by Troosters et al.Citation24 In this study, patients with moderate to severe COPD, who tolerate exercise, presented an increase of 25% in their 6MWD.
Quantitatively, the largest difference in 6MWD between COPD patients and healthy subjects can be explained by the more fatigability of the quadriceps in patients with COPD than in healthy subject. Indeed, as shown in another study,Citation25 which compared patients with COPD to normal subjects, peripheral muscle strength was not completely corrected after training in COPD patients,Citation26,Citation27 suggesting that factors others than chronic inactivity are involved in explaining muscle atrophy and weakness in patients with COPD.Citation22 In young and older normal subjects, muscle hypertrophy and improved neural recruitment patterns account for the increase in muscle strength following program training.Citation24,Citation28 Both mechanisms could play an important role in the improvement of walking distance after training the participants.
Qualitatively, the progress of 6MWD presented a linear and a logarithmic improvement respectively for patients with COPD and healthy subjects during program training. The above linear increase could be explained by a linear rise of V̇O2peak after program training.Citation28,Citation29 In contrast, COPD patients reached a plateau after eight weeks which may be due to many factors such as baseline structure and biochemical status in COPD musclesCitation6,Citation8 or oxidative stress induced by exercise.Citation23 Evidence show that the exercise intolerance in patients with COPD is related to muscular dysfunction, that includes low muscle mass and strength,Citation5 low muscle aerobic enzymes and capillarity,Citation6 early onset of lactic acidosis,Citation7 among other effects.Citation24
Oxidative stress have also been suggested as a potential mechanism in the pathogenesis of COPD and can explain a plateau observed after eight weeks in patients with COPD.Citation30 Evidence for increased oxidative stress in obstructive airway diseases is emerging and several studies have suggested that it can play an important role in their evolution and pathogenesis.Citation23
Opposed to the benefits of the physical exercise on patient with COPD, evidences indicate that physical exercise, especially aerobic, generate reactive oxygen species such as superoxide anion and hydrogen peroxide, capable of causing muscular damage and inflammation.Citation30 This process is known as oxidative damage and could limit the 6MWD progress in patients with COPD.Citation31
These qualitative changes could also be explained by the effect of training on muscle gene expression in COPD and healthy subjects. Indeed, different patterns in muscle gene expression were described, potentially reflecting the specific molecular response of the muscle to exercise in patients with COPD and suggesting additional mechanisms for exercise limitation in COPD.Citation24
In conclusion, the findings of this study demonstrate that an individualized training is more likely to produce optimal benefit for patients with COPD like healthy subjects but with some differences. Rehabilitation program, over 12 weeks, induces a linear improvement of 6MWD in healthy subjects, and a logarithmic improvement for patients with COPD.
Acknowledgements
The authors thank Professor Mohamed Shamssain and Bechir Jarrar for correction of the English. They also wish to thank the participants for their co-operative attitude and dedicated performance.
Disclosure
The authors report no conflicts of interest in this work.
References
- CelliBRMacNeeWAgustiAStandards for the diagnosis and treatment of patients with COPD: a summary of the ATS/ERS position paperEur Respir J20042393294615219010
- NiciLDonnerCWoutersEATS/ERS Pulmonary Rehabilitation Writing CommitteeAmerican Thoracic Society/European Respiratory Society statement on pulmonary rehabilitationAm J Respir Crit Care Med20061731390141316760357
- HoneymanPBarrPStubbingDGEffect of a walking aid on disability, oxygenation, and breathlessness in patients with chronic airflow limitationJ Cardiopulm Rehabil19961663678907444
- RiesALKaplanRMLimbergTMPrewittLMEffects of pulmonary rehabilitation on physiologic and psychosocial outcomes in patients with chronic obstructive pulmonary diseaseAnn Intern Med1995122118238327741366
- SalaERocaJMarradesRMEffects of endurance training on skeletal muscle bioenergetics in chronic obstructive pulmonary diseaseAm J Respir Crit Care Med19991591726173410351910
- SattaAMiglioriGBSpanevelloAFiber types in skeletal muscles of chronic obstructive pulmonary disease patients related to respiratory function and exercise toleranceEur Respir J199710285328609493673
- CasaburiRPatessioAIoliFReductions in exercise lactic acidosis and ventilation as a result of exercise training in patients with obstructive lung diseaseAm Rev Respir Dis19911439181986689
- WuyamBPayenJFLevyPMetabolism and aerobic capacity of skeletal muscle in chronic respiratory failure related to chronic obstructive pulmonary diseaseEur Respir J199251571621559579
- MaltaisFJobinJSullivanMJMetabolic and hemodynamic responses of lower limb during exercise in patients with COPDJ Appl Physiol199884157315809572801
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function LaboratoriesATS statement: guidelines for the six-minute walk testAm J Respir Crit Care Med200216611111712091180
- Kesten1SCasaburiRKukafkaDCooperCImprovement in self-reported exercise participation with the combination of tiotropium and rehabilitative exercise training in COPD patientsInternational Journal of COPD20083112713618488436
- KervioGVilleNSLeclercqCDaubertJ-CCarréFIntensity and daily reliability of the six-minute walk test in moderate chronic heart failure patientsArch Phys Med Rehabil2004851513151815375827
- SolanesIGüellRCasanPDuration of pulmonary rehabilitation to achieve a plateau in quality of life and walk test in COPDRespir Med2009103572272819117744
- LiuJDrutzCKumarRUse of the six-minute walk test poststroke: is there a practice effectArch Phys Med Rehabil2008891686169218760152
- QuanjerPHTammelingGJCotesJEPedersenOFPeslinRYernaultJCLung volumes and forced ventilatory flows: report Working Party Standardization of Lung Function Tests, European Community for Steel and Coal; official statement of the European Respiratory SocietyEur Respir J Suppl1993165408499054
- RossRMATS/ACCP statement on cardiopulmonary exercise testingAm J Respir Crit Care Med200316710145112738602
- BeaverWLWassermanKWhippBJA new method for detecting anaerobic threshold by gas exchangeJ Appl Physiol1986606202020273087938
- Ben SaadHPrefautCTabkaZ6-minute walk distance in healthy North Africans older than 40 years: influence of parityRespir Med20091031748419041233
- MerckenEMHagemanGJScholsAMRehabilitation decreases exercise-induced oxidative stress in chronic obstructive pulmonary diseaseAm J Respir Crit Care Med2005172994100116040783
- KillianKJLeblancPMartinDHSummersEJonesNLCampbellEJMExercise capacity and ventilatory, circulatory, and symptom limitation in patients with chronic airflow limitationAm Rev Respir Dis19921469359401416421
- ValletGAhmaidiSSerresIComparison of two training programmes in chronic airway limitation patients: standardized versus individualized protocolsEur Respir J1997101141229032502
- GosselinkRTroostersTDeCramerMPeripheral muscle weakness contributes to exercise limitation in COPDAm J Respir Crit Care Med19961539769808630582
- Radom-AizikSKaminskiNHayekSHalkinHCooperDMBen-DovIEffects of exercise training on quadriceps muscle gene expression in chronic obstructive pulmonary diseaseJ Appl Physiol2007102519768417483440
- TroostersTGosselinkRDecramerMExercise training in COPD: how to distinguish responders from nonrespondersJ Cardiopulm Rehabil2001211101711271652
- BernardSWhittomFLeblancPAerobic and strength training in patients with chronic obstructive pulmonary diseaseAm J Respir Crit Care Med1999159389690110051269
- MaltaisFLeBlancPSimardCSkeletal muscle adaptation to endurance training in patients with chronic obstructive pulmonary diseaseAm J Respir Crit Care Med19961542 Pt 14424478756820
- ShahinBGermainMKazemAAnnatGBenefits of short inspiratory muscle training on exercise capacity, dyspnea, and inspiratory fraction in COPD patientsInt J Chron Obstrct Pulmon Dis200833423427
- FronteraWRMeredithCNO’ReillyKPKnuttgenHGEvansWJStrength conditioning in older men: skeletal muscle hypertrophy and improved functionJ Appl Physiol1988643103810443366726
- HicksonRCBomzeHAHolloszyJOLinear increase in aerobic power induced by a strenuous program of endurance exerciseJ Appl Physiol1977423372376838658
- StevensonCSKochLGBrittonSLAerobic capacity, oxidant stress, and chronic obstructive pulmonary disease: a new take on an old hypothesisPharmacol Ther2006110718216343638
- GerritsenWBAsinJZanenPvan den BoschJMHaasFJMarkers of inflammation and oxidative stress in exacerbated chronic obstructive pulmonary disease patientsRespir Med2005991849015672854