Abstract
Insulin glulisine is appealing in principle, but the advantages of this drug over the other rapid-acting insulin analogs are still relatively unknown. The frequency of hypoglycemia, convenience in the timing of administration, and improvements in terms of HbA1c seem similar among the rapid-acting insulin analogs, including insulin glulisine. Only properly randomized long-term clinical studies with insulin glulisine will reveal the true value of this novel insulin analog.
Background
The discover of insulin in 1921 introduced a new era for the treatment of diabetes. After the DCCT study was reported in 1993Citation1 and the UKPDS was reported in 1998,Citation2,Citation3 it was assumed that tight glycemic control is important to prevent diabetic complications in both type 1 and type 2 diabetes. Because the ACCORD studyCitation4 showed the difficulties in achieving tight glycemic control without harmful hypoglycemic episodes and the ADVANCECitation5 and VADTCitation6 studies revealed the difficulties in preventing cardiovascular complications, patients with diabetes need more effective and safer treatment strategies.
Type 2 diabetes is a progressive disease characterized by relentless deterioration of pancreatic beta cell function,Citation7 and the incidence of type 2 diabetes is increasing, particularly in younger individuals.Citation8 These facts suggest that an increasing number of patients with type 2 diabetes will ultimately require insulin therapy. Therefore, insulin analogs have been developed to mimic physiological insulin action, which allow tighter glycemic control with reduced risk of severe hypoglycemic episodes and offer good quality of life (QOL) in the absence of complications.
Development of insulin analogs
shows the molecular structure of insulin, which has a molecular weight of about 6000 kDa and consists of an A chain with 21 amino acids and a B chain with 30 amino acids.Citation9
Figure 1 The amino acid sequence of human insulin and rapid-acting insulin analogs. Pink circles: amino acid residues involved in dimer formation. Blue circles: amino acid residues involved in hexamer formation. Arrow: amino acid residues involved in binding with the insulin receptor. A) human insulin, B) insulin lispro, C) insulin aspart, and D) insulin glulisine.
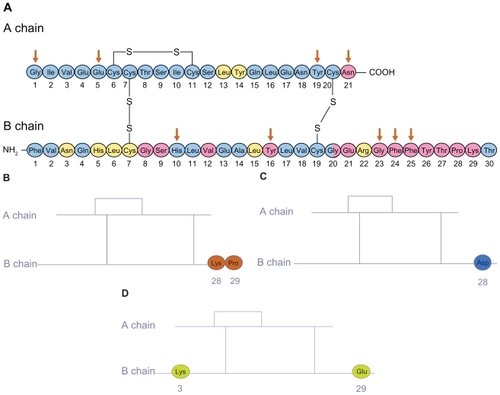
The N-terminal of the A chain and the C-terminal of the B chain are the sites that bind to the insulin receptor. Thus, substitution in these amino acids will alter the avidity to the insulin receptor and the activity of the analog as an insulin receptor agonist. In addition, insulin forms stabile hexamers centered on Zn in solution. When this hexamer is injected subcutaneously, at first it will be resolved to a dimer and then a monomer, which is the absorbable form. The C-terminal of the B chain is critical in the formation of the dimer. Thus, substitution of amino acids in this area affects the conversion from the hexamer to the monomer and may aid rapid absorption. So far, three kinds of rapid-acting insulin analog have been introduced, namely insulin lispro, insulin aspart and insulin glulisine.
In insulin lispro, the natural sequence of proline at position B28 and lysine at position B29 is reversed ().Citation10 In insulin aspart, the natural sequence of proline at position B28 is substituted by aspartic acid ().Citation11 As these changes suggest, position B28 is a locus involved in dimer formation.
Structure of insulin glulisine
In insulin glulisine, the natural sequence of asparagine at position B3 and lysine at position B29 are substituted by lysine and glutamic acid, respectively ().Citation12,Citation13 This structure of insulin glulisine affects not only self-association but also the isoelectric point, which is shifted lower (pH 5.1; human insulin, pH 5.5), which enhances its solubility at a physiologic pH. As a consequence, unlike other insulin analogs that lack proline at B28, insulin glulisine is more likely to self-associate into dimers in the absence of ligands. Thus, there are several important differences between insulin glulisine and the other rapid-acting insulin analogs, insulin lispro and insulin aspart (). The insulin glulisine solution does not contain hexamer-promoting Zn, but does include polysorbate 20 as a stabilizer and trometamol as a buffer. Polysorbate 20 is also known commercially as Tween 20. This is used as an excipient in pharmaceutical applications to stabilize emulsions and suspensions. Purified protein derivative (PPD) solution, which contains polysorbate 20, is used in skin testing for tuberculosis exposure. Trometamol is known as Tris or THAM and is extensively used in biochemistry and molecular biology. In a clinical setting, trometamol is used as an alternative to sodium bicarbonate for the treatment of metabolic acidosis. Although the clinical effects of long-term administration of polysorbate 20 and trometamol are unknown, no Zn must be helpful because this allows more rapid absorption.
Table 1 Comparison of regular human insulin and rapid-acting insulin analogs
Pharmacokinetics and biologic actions of insulin glulisine
Pharmacokinetic studies with insulin glulisine have shown an absorption profile with a peak insulin concentration that is approximately twice that of regular human insulin, and which is reached in approximately half the time. Compared with insulin lispro, several studiesCitation14–Citation16 have shown a faster onset of action for insulin glulisine. So far, no study has directly compared the pharmacokinetics of insulin aspart and insulin glulisine. However, Homko et al described similar pharmacokinetics and metabolic effects of insulin lispro and insulin aspart.Citation17 Accordingly, insulin glulisine may have the most rapid onset of action of the rapid-acting insulin analogs. But, in terms of the metabolic effect, Horvath et al showed that insulin glulisine, insulin lispro, and regular insulin have similar effects on hepatic glucose production and glucose uptake.Citation18
According to a review of the clinical pharmacokinetics and pharmacodynamics of insulin glulisine,Citation12 dose proportionality in early, maximum and total exposure is observed for insulin glulisine over the therapeutic relevant dose range up to 0.4 U/kg. The pharmacodynamic profile of insulin glulisine reflects the absorption kinetics by demonstrating a greater rate of glucose utilization, which is completed earlier and at equipotency on a molar base compared with regular human insulin.Citation12 Dose proportionality in glucose utilization has been established for insulin glulisine in patients with type 1 diabetes in the dose range of 0.075 to 0.15 U/kg, and with less intra-subject variability compared with insulin lispro and regular human insulin.Citation12
Clinical studies of insulin glulisine
Glycemic control
In general, the history of insulin glulisine is short and clinical studies are few. First, therefore, the rapid-acting insulin analogs should be described. The effects of rapid-acting insulin analogs on HbA1c levels have been reviewed systematically and meta-analyzed.Citation19 In that review of 49 randomized clinical studies comparing rapid-acting insulin analogs with regular human insulin, a weighted mean difference in HbA1c of −0.1% was determined in favor of analogs in patients with type 1 diabetes. Among patients with type 2 diabetes, there was no difference in HbA1c between rapid-acting analogs and regular human insulin. But, only one study used insulin glulisine (37 studies used insulin lispro, 10 used insulin aspart, one used insulin lispro and insulin aspart).Citation20 In that study, Garg et al showed that injection of insulin glulisine 0–15 minutes before meals (n = 268) reduced HbA1c (−0.26%) more than the injection of regular insulin 30–45 minutes before meals (n = 257) (−0.13%) in type 1 diabetes.Citation20
Furthermore, Dailey et al reported that insulin glulisine (n = 435) provided a slightly greater reduction in HbA1c (−0.46%) than regular insulin (n = 441) (−0.30%) in type 2 diabetes.Citation21 There were no between-group differences in baseline-to-end point changes in insulin dose.
On the other hand, Dreyer et al reported similar reductions in HbA1c (−0.14%) with insulin glulisine and insulin lispro over a 26-week study in patients with type 1 diabetes (insulin glulisine, n = 339; insulin lispro, n = 333).Citation22 In that study, there was a significant difference in changes in daily dose of insulin; −0.86 U in the insulin glulisine group and + 1.01 U in the insulin lispro group.
Meanwhile, Hoogma et al described that insulin glulisine can be safely used in continuous subcutaneous insulin infusion (CSII) and does not have any adverse clinical implications compared with insulin aspart.Citation23 These data suggest that insulin glulisine may be useful in achieving glycemic control that is greater than that with regular insulin and similar to that with the other rapid-acting insulin analogs.
Hypoglycemia
In terms of hypoglycemia, the Cochrane review of clinical studies found a lower incidence of severe hypoglycemic episodes with rapid-acting insulin analogs (median 21.8 episodes per 100 person-years in type 1 diabetes and 0.3 in type 2 diabetes) compared with regular insulin (median 46.1 episodes per 100 person-years in type 1 diabetes and 1.4 in type 2 diabetes).Citation19 Although only one study using insulin glulisine was included in that review, the study by Garg et al showed a non-significant reduction in severe hypoglycemic episodes in the insulin glulisine groups (8.4% with premeal insulin glulisine and 8.4% with postmeal insulin glulisine vs 10.1% with premeal regular insulin).Citation20
Dailey et al reported that the proportion of patients with serious hypoglycemia was comparable between the insulin glulisine (n = 15, 3.4%) and regular insulin (n = 11, 2.5%) groups. The adjusted mean change in body weight was also similar in both treatment groups (glulisine, 1.8 kg; regular insulin, 2.0 kg).Citation21
In Dreyer’s study, the hypoglycemic episodes were comparable between insulin glulisine and insulin lispro; 3.64 ± 4.49 symptomatic hypoglycemic events per patient-month with insulin glulisine and 3.48 ± 4.38 with insulin lispro; the respective rates for severe hypoglycemia were 0.03 ± 0.12 and 0.02 ± 0.11 events per patient-month and for nocturnal hypoglycemia were 0.55 ± 0.94 and 0.53 ± 0.84 events per patient-month.Citation22
These data suggest that, at least, insulin glulisine does not increase hypoglycemia compared with the other short-acting insulin products.
Quality of life
I searched Medline for published articles with terms related to “glulisine” and “quality-of-life”. Although this search provided 8 articles, there was no original research article. Therefore, I describe the rapid-acting insulin analogs on quality-of life. In terms of quality of life and treatment satisfaction, only 12 of the 49 studies assessed in the Cochrane review included reported these data. Of these 12 studies, 7 used the Diabetes Treatment Satisfaction Questionnaire (DTSQ);Citation19 3 studies found no significant difference in DTSQ between the treatment arms,Citation24–Citation26 and 4 studies showed an improvement in the analog group.Citation27–Citation30
Immunogenicity and safety
Because the history of insulin glulisine is still limited, I cannot describe its immunogenicity. For insulin lispro and insulin aspart, the structural changes were initially reported to result in decreased immunogenicity in in vivo studies.Citation9,Citation31 However, recent studies of insulin allergy demonstrated the existence of clinical allergy to these new insulin analogs and to regular insulin.Citation32–Citation34 Because insulin glulisine contains polysorbate 20 and trometamol as well as structural changes, one may anticipate different immunogenicity profiles compared with regular insulin.
Use of insulin glulisine in clinical settings
So far, there are few clinical studies of insulin glulisine. Firm conclusions cannot therefore be made on the utility of this new insulin analog. However, as mentioned above, insulin glulisine appears to have the most rapid onset of action of the insulin analogs and, in addition, may provide better glycemic control and reduced risk of hypoglycemia compared with regular insulin. This new insulin analog may be particularly useful in patients with high risk of hypoglycemia or insulin allergy and could also be a useful insulin to be considered for insulin pump therapy. In the future, more clinical use and good randomized long-term clinical studies with insulin glulisine will reveal the true value of this novel insulin analog.
Disclosures
The author declares no conflicts of interest.
References
- The Diabetes Control and Complications Trial (DCCT) Research GroupThe effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitusN Engl J Med1993329149779868366922
- UK Prospective Diabetes Study (UKPDS) GroupIntensive blood-glucose control with sulphonylureas of insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS33)Lancet199835291318378539742976
- UK Prospective Diabetes Study (UKPDS) GroupEffect of intensive blood-glucose control with metformin on complications in overweight patients with type 2 diabetes (UKPDS34)Lancet199835291318548659742977
- The Action to Control Cardiovascular Risk in Diabetes Study GroupEffects of intensive glucose lowering in type 2 diabetesN Engl J Med2008358242545255918539917
- The ADVANCE Collaborative GroupIntensive blood glucose control and vascular outcomes in patients with type 2 diabetesN Engl J Med2008358242560257218539916
- DuckworthWAbrairaCMoritzTGlucose control and vascular complications in veterans with type 2 diabetesN Engl J Med2009360212913919092145
- MaedlerKDonathMYBeta-cells in type 2 diabetes: a loss of function and massHorm Res200462Suppl 3S67S73
- ZimmetPAlbertiKGMMShawJGlobal and societal implications of the diabetes epidemicNature2001414686578278711742409
- BrangeJOwensDRKangSVolundAMonomeric insulins and their experimental and clinical implicationsDiabetes Care19901399239542226110
- WildeMIMcTavishDInsulin lispro: a review of its pharmacological properties and therapeutic use in the management of diabetes mellitusDrugs19975445976149339963
- LindholmAJacobsenLVClinical pharmacokinetics and pharmacodynamics of insulin aspartClin Pharmacokinet200140964165911605714
- BeckerRHFrickADClinical pharmacokinetics and pharmacodynamics of insulin glulisineClin Pharmacokinet200847172018076215
- BeckerRHInsulin glulisine complementing basal insulins: a review of structure and activityDiabetes Technol Ther20079110912117316105
- BeckerRHFrickADBurgerFPotgieterJHScholtzHInsulin glulisine, a new rapid-acting insulin analogue, displays a rapid time-action profile in obese non-diabetic subjectsExp Clin Endocrinol Diabetes2005113843544316151977
- HeiseTNosekLSpitzerHInsulin glulisine: a faster onset of action compared with insulin lisproDiabetes Obes Metab20079574675317593235
- LuzioSPeterRDunseathGJMustafaLOwensDRA comparison of preprandial insulin glulisine versus insulin lispro in people with type 2 diabetes over a 12-h periodDiabetes Res Clin Pract200879226927518164094
- HomkoCDeluzioAJimenezCKolaczynskiJWBodenGComparison of insulin aspart and lisproDiabetes Care20032672027203112832307
- HorvathKBockGRegittnigWInsulin glulisine, insulin lispro and regular human insulin chow comparable end-organ metabolic effects: an exploratory studyDiabetes Obes Metab200810648449117764465
- SiebenhoferAPlankJBergholdAShort acting insulin analogues versus regular human insulin in patients with diabetes mellitusCochrane Database Syst Rev2006192CD00328716625575
- GargSKRosenstockJWaysKOptimized basal-bolus insulin regimens in type 1 diabetes: insulin glulisine versus regular human insulin in combination with basal insulin glargineEndocr Pract2005111111716033730
- DaileyGRosenstockJMosesRGWaysKInsulin glulisine provides improved glycemic control in patients with type 2 diabetesDiabetes Care200427102363236815451901
- DreyerMPragerRRobinsonAEfficacy and safety of insulin glulisine in patients with type 1 diabetesHorm Metab Res2005371170270716308840
- HoogmaRPLSchumickiDSafety of insulin glulisine when given by continuous subcutaneous infusion using an external pump in patients with type 1 diabetesHorm Metab Res200638642943316823727
- JohanssonUBAdamsonUCLinsPEWredlingRAImproved blood glucose variability, HbA1c insuman infusat and less insulin requirement in IDDM patients using insulin lispro in CSII. The Swedish Multicenter lispro insulin studyDiabetes Metab200026319219610880892
- GaleEAA randomized, controlled trial comparing insulin lispro with human soluble insulin in patients with type 1 diabetes on intensified insulin therapyDiabet Med200017320921410784225
- FergusonSCStrachanMWJanesJMFrierBMSevere hypoglycaemia in patients with type 1 diabetes and impaired awareness of hypoglycaemia: a comparative study of insulin lispro and regular human insulinDiabetes Metab Res Rev200117428529111544612
- RennerRPfutznerATrautmannMHarzerOSauterKLandgrafRUse of insulin lispro in continuous subcutaneous insulin infusion treatment. Results of a multicenter trialDiabetes Care199922578478810332682
- HomePDLindholmARiisAInsulin aspart vs human insulin in the management of long-term blood glucose control in type 1 diabetes mellitus: a randomized controlled trialDiabet Med2000171176277011131100
- BottUEbrahimSHirschbergerSSkovlundSEEffect of the rapid-acting insulin analogue insulin aspart on quality of life and treatment satisfaction in patients with type 1 diabetesDiabet Med200320862663412873289
- AnnuzziGDel PratoSArcariRPreprandial combination of lispro and NPH insulin improves overall blood glucose control in type 1 diabetic patients: a multicenter randomized crossover trialNutr Metab Carciovasc Dis2001113168175
- OttesenJLNilssonPJamiJThe potential immunogenicity of human insulin and insulin analogues evaluated in a transgenic mouse modelDiabetologia19943712117811857895946
- FinebergNSFinebergSEAndersonJHBirkettMAGibsonRGHufferdSImmunologic effects of insulin lispro [(Lys(B28), Pro(B29) human insulin)] in IDDM and NIDDM patients previously treated with insulinDiabetes19964512175017548922361
- FinebergSEHuangJBrunelleRGulliyaKSAndersonJH JrEffect of long-term exposure to insulin lispro on the induction of antibody response in patients with type 1 or type 2 diabetesDiabetes Care2003261899612502663
- LindholmAJensenLBHomePDRaskinPBoehmBORastamJImmune responses to insulin aspart and biphasic insulin aspart in people with type 1 and type 2 diabetesDiabetes Care200222587688211978684