Abstract
The American Diabetes Association and The European Association for the Study of Diabetes recommend metformin as the initial agent of choice in the treatment of type 2 diabetes mellitus. Unfortunately, most patients require multiple medications to obtain glycemic control. One of the newest additions to the antidiabetic armamentarium is the class of drugs known as dipeptidyl-peptidase IV (DPP-IV) inhibitors. This novel approach focuses on harnessing the beneficial effects of GLP-1, an incretin hormone released from the gut postprandially. The first DPP-IV inhibitor approved in the United States was sitagliptin. It has been studied in both monotherapy and combination therapy. Combination studies with metformin realize a hemoglobin A1c reduction of 0.65%–1.1%. The combination of the two has a modest positive effect on body weight with the convenience of an oral route of administration. It has also been shown to be highly tolerable, efficacious and with little risk of hypoglycemia. This review will focus on combination therapy with sitagliptin with emphasis on combination with metformin.
Introduction
According to current estimates, type 2 diabetes mellitus (T2DM) affects approximately 21 million Americans.Citation1 Insulin resistance, the primary defect present in T2DM, is mainly due to genetic and lifestyle factors. Current treatment strategies focus on lifestyle changes, reducing hyperglycemia, and improving insulin sensitivity. Weight loss and oral medications improve insulin sensitivity and lower blood glucose by decreasing insulin resistance. Other agents including insulin secretagogues, biguanides, insulin analogs, and dipeptidyl peptidase (DPP-IV) inhibitors also reduce blood glucose, through diverse mechanisms. Despite this wide array of treatment options, most patients remain above goal.
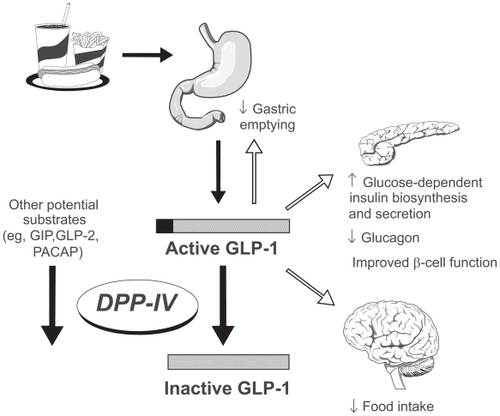
Sitagliptin, a DPP-IV inhibitor, helps the body take advantage of the incretin hormone glucagon-like peptide (GLP-1). GLP-1 is released from the gastrointestinal tract in response to a meal. When blood glucose is elevated, GLP-1 stimulates insulin secretion. In addition, GLP-1 reduces glucagon secretion, slows gastric emptying, and appears to regulate the growth of insulin producing β-cells ().Citation2 GLP-1 is rapidly inactivated by the DPP-IV enzyme.Citation3 By inhibiting DPP-IV, the positive effects of GLP-1 are prolonged. This article reviews publications and abstracts involving combination therapy with sitagliptin. These trials should provide greater insight into sitagliptin’s role in combination therapy.
Figure 1 The role of glucagon-like peptide (GLP-1) in glucose homeostasis. Reprinted with permission from Weber A. Dipeptidyl peptidase IV inhibitors for the treatment of diabetes. J Med Chem. 2004;47:4135–4141.Citation2 Copyright © American Chemical Society.
Pharmacology
Experts have identified multiple signals leading from the gastrointestinal tract to the pancreas.Citation4 An experiment first described in the 1960s compared the metabolic response to a glucose load delivered intravenously versus orally. Levels of serum glucose appeared similar; however the plasma insulin response evoked from the oral glucose load was far greater. In other words, the intravenous glucose load provided a suboptimal insulin response when compared to an oral glucose load. This has been termed the incretin effect; the majority of its effect modulated by the incretin hormones GLP-1 and glucose-dependent insulinotropic peptide (GIP).
An incretin is a hormone that is released from the gut in response to nutrients (mainly carbohydrates), stimulates insulin release in response to a meal, and causes insulin release in a glucose dependent manner.Citation4 The gastrointestinal hormone GLP-1 is quickly inactivated by the DPP-IV enzyme. DPP-IV is found in the kidneys, intestines, and bone marrow with lower concentrations in the liver, pancreas, placenta, thymus, spleen, epithelial cells, vascular endothelium, and lymphoid and myeloid cells.Citation2,Citation5
Patients with T2DM have been shown to have reduced concentrations of intact GLP-1. Vilsboll et al conducted a study involving 12 subjects with T2DM and 12 healthy controls.Citation6 Blood samples were collected at 15, 30, 45, 60, 75, 90, 120, 150, and 180 minutes postprandially to determine intact GLP-1 concentrations. GLP-1 concentrations were lower in patients with diabetes 75, 90, and 120 minutes after meal ingestion (p = 0.056, 0.017, and 0.017, respectively). In addition, insulin and C-peptide concentrations were decreased during these same time periods, indicating an abnormal insulin response. The investigators concluded that in the absence of normal concentrations of intact GLP-1, the insulin response in patients with T2DM is blunted.
Kinetics
The oral bioavailability of sitagliptin is 87% with a terminal half-life of 10 to 12 hours. Median time to maximum concentration (Tmax) is 1 to 6 hours and varies across the dosing range; sitagliptin is excreted primarily by the kidneys.Citation7,Citation8 Neither the absorption, Tmax, nor the half-life are significantly altered when sitagliptin is administered with food. Although sitagliptin is a minor substrate for the CYP450 system, it is not an inhibitor or inducer of this system.Citation7 The apparent volume of distribution is 198 L and sitagliptin has been reported to be 38% bound to plasma proteins.Citation7
Clinical trials
Sitagliptin has been studied with metformin, glipizide, glimepiride and pioglitazone (). One of the first studies to address sitagliptin as add-on therapy to metformin in patients with inadequate glycemic control was conducted by Brazg and colleagues.Citation9 In this doubleblind, randomized, placebo-controlled, cross-over study, 28 patients (baseline HgbA1c [A1c] ranging from 6.5% to 9%) received sitagliptin 50 mg twice daily or placebo for 4 weeks followed by the opposite treatment for an additional 4 weeks. The primary endpoint analyzed was 24-hour weighted mean glucose (WMG); secondary endpoints included fasting plasma glucose (FPG) and fructosamine. There was a significant least-squares mean reduction in WMG, FPG and fructosamine (32.8 mg/dL, 20.3 mg/dL, and 33.7 mmol/L, respectively). The addition of sitagliptin did not lead to additional adverse events compared to metformin monotherapy. This short term study highlighted the efficacy and tolerability of combination therapy with metformin and sitagliptin.
Table 1 Pivotal combination studies with sitagliptin
A 24-week study conducted by Goldstein, et al assessed the effect of adding sitagliptin and metformin in 1091 patients inadequately controlled on diet and exercise alone.Citation10 This double-blind, placebo-controlled, parallel-group study randomized patients to one of six treatment groups: sitagliptin 100 mg + metformin 1000 mg, sitagliptin 100 mg + metformin 2000 mg, metformin 1000 mg, metformin 2000 mg, sitagliptin 100 mg, or placebo. The mean baseline A1c was 8.8%. The placebo subtracted changes in A1c after 24 weeks of treatment were 2.07%, 1.57%, 1.3%, 0.99%, and 0.83% for the sitagliptin 100 mg + metformin 1000 mg, sitagliptin 100 mg + metformin 2000 mg, metformin 1000 mg, metformin 2000 mg, and sitagliptin 100 mg groups, respectively (p < 0.001 for all comparisons versus placebo). The incidence of hypoglycemia reported was low (0.5% to 2.2%) and similar to placebo (0.6%); sitagliptin did not appear to increase gastrointestinal adverse events associated with metformin use. The authors concluded combination therapy with metformin and sitagliptin provides additive glycemic benefit and is generally well tolerated.
Charbonnel et al conducted a 24-week randomized, double-blind, parallel-group study in 701 patients.Citation11 This study assessed the safety and efficacy of adding sitagliptin to ongoing metformin therapy (≥1500 mg/day) in patients with a mean A1c of 8.0%. Patients were randomized to receive sitagliptin 100 mg daily or placebo. At study end, sitagliptin treatment produced a significant reduction in A1c (0.65%, p < 0.001), and FPG (25.4 mg/dL, p < 0.001). No increase in the incidence of gastrointestinal events was noted and hypoglycemia rates between groups were similar. Nasopharyngitis, urinary tract infection, arthralgia, back pain and cough were all experienced at a higher incidence in the sitagliptin group compared to placebo. Body weight remained neutral. The authors concluded that sitagliptin 100 mg once daily was well tolerated and provided sustained improvements in A1c and FPG in patients inadequately controlled on metformin monotherapy. A 30-week extension was then conducted.Citation12 Patients initially treated with sitagliptin remained on the drug, while patients taking placebo were switched to glipizde 5 mg daily (titrated to a maximum dose of 15 mg/day). Of the original 701 patients randomized, 544 patients continued with this portion of the study (sitagliptin n = 387, glipizide n = 157). For patients already on sitagliptin, the A1c did not change significantly from week 24 to week 52 (−0.07%). The change in A1c from baseline was −0.7% (p-value not reported) in the sitagliptin arm and −0.9% (p-value not reported) in the glipizide arm. Hypoglycemia was reported more in the glipizide group compared to sitagliptin (16% versus <1%, respectively). The sitagliptin group experienced a weight reduction of 0.9 kg from baseline; conversely, patients in the glipizide arm recorded a weight gain of 1.5 kg.
In a long term trial, Nauck and colleagues conducted a non-inferiority study to compare the effects of adding sitagliptin or glipizide to patients uncontrolled on metformin monotherapy (mean baseline A1c 7.5%).Citation13 Patients were randomized to receive sitagliptin (n = 588) 100 mg daily or glipizide (n = 584) 5 mg daily (titrated to a maximum of 20 mg daily) for 52 weeks. The primary endpoint was defined as the change in A1c from baseline. A1c changes from baseline were −0.67% for both groups, confirming noninferiority of sitagliptin. Fasting plasma glucose decreased from baseline in the sitagliptin group (10.0 mg/dL, p-value not reported) as well as the glipizide group (7.5 mg/dL, p-value not reported). More patients in the glipizide group experienced hypoglycemia (32%, p < 0.001) compared to sitagliptin (5%, p < 0.001). Body weight was reduced with sitagliptin (1.5 kg, p < 0.001), compared with weight gain in the glipizide arm (1.1 kg, p < 0.001). The authors concluded that sitagliptin is comparable to glipizide in glycemic control but free from significant hypoglycemia and weight gain.
The safety and efficacy of sitagliptin addition was studied in a 24-week, randomized, double-blind trial in patients inadequately controlled on glimepride with or without metformin.Citation14 Patients were randomized to receive the addition of sitagliptin 100 mg daily or placebo (212 on glimepiride, 229 on glimepiride and metformin). After 24 weeks, sitagliptin reduced the A1c by 0.74% (p < 0.001) in the overall randomized cohort of patients. In the subset of patients receiving metformin and glimepiride, the largest A1c reduction was noted (0.89%, p-value not reported), compared to the subset of patients on glimepiride alone (−0.57%, p-value not reported). Fasting and postprandial blood glucose also improved with the addition of sitagliptin. Hypoglycemia was higher in the sitagliptin group compared to placebo (12% vs 2%, p < 0.001); however, no episodes required medical attention. At study end, the placebo-adjusted body weight was increased in the sitagliptin arm (1.1 kg, p < 0.001).
The combination of sitagliptin and pioglitazone was explored in a 24-week, double-blind, placebo-controlled, parallel-group study.Citation15 In this study, 353 patients on pioglitazone monotherapy (30 or 45 mg/daily) were randomized to receive either the addition of sitagliptin 100 mg daily or placebo. The primary efficacy end point was change in A1c from baseline to study end. Fasting plasma glucose was a secondary end point. The addition of sitagliptin significantly reduced A1c with a between-treatment difference of 0.7% (p < 0.001). Fasting plasma glucose also decreased by 17.7 mg/dL (p < 0.001). The proportion of patients able to reach an A1c of <7% was 45.4% in the sitagliptin group versus 23.0% in the placebo group. The sitagliptin plus pioglitazone group experienced a higher incidence of gastrointestinal adverse effects than placebo (13.7% vs 6.2%, respectively). No significant difference in hypoglycemia was observed. Both groups experienced one episode of edema; no reports of congestive heart failure were observed. The authors concluded that the combination of sitagliptin plus pioglitazone is well tolerated and significantly improves glycemic control.
Clinical trial limitations
Findings discussed in the above trials are limited to specific populations enrolled in each trial. To date, most of the clinical trials involving sitagliptin combination therapy are limited to metformin. Additional studies involving combination therapy with sitagliptin and other antihyperglycemic agents are needed in order to make recommendations regarding optimal combination therapy. Also, the efficacy and safety of sitagliptin combination therapy has not been evaluated beyond one year; future trials of longer duration will be needed to define its role. Given sitagliptin’s potential to affect disease progression, effects on microvascular and macrovascular outcomes should also be explored.
Adverse events
The most common adverse events associated with sitagliptin include nasopharyngitis, upper respiratory tract infection, and headache. Other adverse events reported with sitagliptin include abdominal pain, nausea, diarrhea, and vomiting; however, the incidence of these adverse events are similar to placebo.Citation7 In clinical trials sitagliptin has not been associated with any significant changes in complete blood counts, transaminase and serum creatinine levels, vital signs, or electrocardiogram.Citation7 It is important to note, however, that hypersensitivity reactions such as anaphylaxis, angioedema, and Stevens-Johnson syndrome have been reported during post-marketing surveillance.Citation16
Hypoglycemia, an adverse event that plagues several of the other available treatments for T2DM, is not significant with sitagliptin therapy. In fact, a pooled analysis of four studies showed that the incidence of hypoglycemia was 1.2%, 0.9%, and 0.9% with sitagliptin 100 mg, sitagliptin 200 mg, and placebo, respectively.Citation8
Weight gain is another adverse event of concern to practitioners treating T2DM. Treatment with sitagliptin has shown variable results. Monotherapy studies with sitagliptin showed a small reduction in weight; however, a greater reduction was experienced by the placebo groups. When combined with metformin or pioglitazone, weight changes were similar relative to placebo. Sitagliptin in combination with sulfonylureas led to a significant weight increase when compared to the placebo groups.Citation8
Drug interactions
Sitagliptin appears to be well tolerated with a marginal drug interaction profile. It is a minor substrate of the CYP450 system, but is not an inhibitor or inducer of any of the isoenzymes.Citation7 Sitagliptin is not extensively bound to plasma proteins.Citation7 Subsequently, the probability of sitagliptin being involved in clinically meaningful drug-drug interactions mediated by protein plasma binding is quite low. The combination of sitagliptin and metformin when co-administered does not extensively alter the pharmacokinetics of either agent.Citation17 Sitagliptin has been found to increase the area under the curve (AUC) and plasma concentration of digoxin; however, no dosage adjustment is required.Citation18 When administered with cyclosporine, drug exposure and peak concentrations of sitagliptin are increased; therefore, a dose reduction of sitagliptin may be warranted and careful monitoring should be conducted.Citation18
Dosing and administration
The recommended starting dose for sitagliptin is 100 mg daily. Sitagliptin can be given without regards to meals. The dose should be reduced to 50 mg daily with a creatinine clearance (CrCl) of 30 to 50 mL/min and to 25 mg daily with CrCl less than 30 mL/min.Citation7 Patients with T2DM less than 18 years of age should not receive sitagliptin. Sitagliptin is considered pregnancy category B; it is unknown whether sitagliptin is excreted into breast milk. A dose adjustment is not required in geriatric patients; however, caution should be exercised when using sitagliptin in patients who are over 75 years of age.Citation18
Numerous clinical trials with the combination of sitagliptin and metformin have led to the development of Janumet™ (Merck and Co., Inc.), the only commercially available combination product with the aforementioned agents.Citation19 Dosing with sitagliptin and metformin should be individualized as dictated by efficacy and tolerability. The maximum recommended daily dose for metformin is 2550 mg in divided doses; however, increasing the dose over 2000 mg provides marginal benefit.Citation20 The maximum recommended dose of sitagliptin is 100 mg daily in a single or divided dose.Citation21 Janumet™ should be started at the initial dose of 50/500 twice daily for patients with type 2 diabetes not adequately controlled on diet and exercise alone. Dosing may be titrated to Janumet™ 50/1000 twice daily if further glucose lowering is desired. For patients taking 850 mg of metformin twice daily, the manufacturer recommends starting Janumet™ at 50/1000 mg twice daily.Citation19 Due to the effects of metformin on the gastrointestinal system, the combination should be given with meals. Special consideration must be given to patients with renal insufficiency. The package insert of metformin suggests patients with renal disease or insufficiency as evidenced by a serum creatinine of >1.5 mg/dL in males or 1.4 mg/dL in females should not take metformin. The package insert of Janumet™ lists the same contraindications. In addition, patients undergoing radiologic studies involving intravascular administration of iodinated contrast materials should temporarily discontinue Janumet™.Citation19
Sitagliptin has not been approved in combination with other antidiabetic agents. However, in clinical trials sitagliptin has been given in combination with glimepiride, glipizide and pioglitazone. If initiating sitagliptin in patients on sulfonylureas, the dose of the sulfonylurea may need to be reduced to avoid the risk of hypoglycemia.Citation16 Sitagliptin has not been studied with concomitant insulin therapy.
Place in therapy
Lifestyle modifications are the cornerstone of treatment for T2DM and should be implemented early in the course of the disease. Weight loss may significantly improve glucose levels; unfortunately this cost effective approach is met with limited long-term success.Citation22 Consequently, the majority of patients with type 2 diabetes require the addition of pharmacotherapy ().
Table 2 Comparison of approved antidiabetic medications in the United StatesCitation7,Citation16,Citation23
The currently available treatment options target at least three core defects in diabetes by improving insulin sensitivity, improving insulin resistance, or impeding secretion of glucagon. Despite the large arsenal of drug therapies, choosing an appropriate treatment poses a challenge for the health care provider. This challenge is compounded when the initial therapy fails and a choice of adjunctive treatment must be chosen. The American Diabetes Association (ADA) and The European Association for the Study of Diabetes have developed an evidence based algorithm to guide the practitioner in initial as well as adjunctive treatment.Citation24 In combination with lifestyle modifications, metformin should be implemented first line. In addition to its glucose lowering ability, metformin is recommended for its lack of weight gain, high patient tolerability, and cost. To ensure patient compliance, metformin should be titrated slowly and increased to maximum doses over one to two months.
Patients unable to attain glycemic control (A1c < 7%) with maximum doses of metformin should receive an additional agent. Step 2 of the algorithm advocates adding either insulin or a sulfonylurea.Citation24 The A1c will determine which agent to add. If the A1c level is greater than 8.5%, consideration is given to the addition of insulin. Initiation of insulin can either be intermediate acting insulin at bedtime or longer acting insulin given at either bedtime or in the morning. Conversely, adding a sulfonylurea to metformin in patients with a lesser degree of hyperglycemia (ie, A1c < 8.5%) is recommended. If these choices do not produce target glycemic levels, the final step is to intensify insulin treatment or begin insulin if not done in the previous step.
In certain populations, the algorithm recognizes other alternatives. Particularly, if hypoglycemia becomes an issue, addition of pioglitazone or exenatide may be considered. Rosiglitazone is no longer recognized in the consensus algorithm. Several meta-analyses have suggested a relative increase in the risk of myocardial infarction.Citation25–Citation27 The panel decided unanimously to remove rosiglitazone while recognizing that the information currently available is not conclusive regarding the cardiovascular risk associated with rosiglitazone. Other agents are mentioned, but their greater expense and lack of evidence limits their use to special populations. This includes the class of DPP-IV inhibitors.
Sitagliptin was the first DPP-IV approved in 2006. Unlike other newer agents, pramlintide and exenatide, sitagliptin offers the advantage of oral administration. Clinical trials indicate sitagliptin is effective in both monotherapy and combination therapy. It has been studied extensively with metformin. This combination does not cause increased side effects or alter the pharmacokinetics of either agent.
Sitagliptin does not cause hypoglycemia or weight gain which has plagued other classes of antihyperglycemics. The A1c lowering of the DPP-IV inhibitor class is approximately 0.6% to 0.9%, which is less than the first tier agents recommended by the ADA. Several factors must be considered when deciding upon adjunctive therapy including side effects, route of administration, cost, and patient preference. Clinicians should also assess the risks versus benefits when selecting optimal treatment. DPP-IV inhibitors may be most appropriate for patients experiencing hypoglycemia or in patients already on dual oral therapy (sulfonylurea and metformin) with an A1c close to goal. Although sitagliptin is not associated with greater glucose control compared with conventional therapy, it is effective, well tolerated, and provides sustainable reductions in A1c.
Conclusion
Type 2 diabetes mellitus is a chronic, progressive disease often requiring two or more medications to obtain optimal glucose control. With the discovery of the incretin effect came the emergence of a new class of drugs, the DPP-IV inhibitors. The exact role of sitagliptin, the prototype DPP-IV inhibitor, remains to be explored. Currently, the ADA recommends metformin as the initial agent of choice, followed by sulfonylureas and insulin as preferred adjunctive therapy. Patients experiencing hypoglycemia on conventional therapy, or remaining above the desired A1c goal, may be candidates for sitagliptin. Evidence suggests that combining metformin and sitagliptin provides a positive effect on body weight and A1c with the convenience of oral administration. It is also proven to be safe, efficacious and well tolerated. Although the combination of sitagliptin and metformin appears effective, the use of this combination may be restricted by its relatively high cost and lack of long term safety data. Also, information on sitagliptin in combination with other antidiabetic agents is lacking.
Disclosures
The authors have no conflicts of interest to disclose.
References
- Centers for Disease Control and PreventionDiabetesaccessed January 18 2006 Available at http://www.cdc.gov/diabetes/pubs/pdf/ndfs_2005.pdf
- WeberADipeptidyl peptidase IV inhibitors for the treatment of diabetesJ Med Chem2004474135414115293982
- DooseopKWangLBeconiMEiermannGJFisherMHHeH(2R)-4-oxo-4-[3-(trifluoromethyl)-5,6-dihydro[1,2,4]triazolo[4,3-a]pyrazin-7(8H)-yl]-1-(2,4,5-trifluorophenyl)butan-2-amine: a potent, orally active dipeptidyl peptidase IV inhibitor for the treatment of type 2 diabetesJ Med Chem200548114115115634008
- CreutzfeldtWThe [pre-] history of the incretin conceptRegul Pept2005128879115780427
- McIntoshCDemuthHPospisilikJPedersonRDipeptidyl peptidase IV inhibitors: how do they work as new antidiabetic agents?Regul Pept200512815916515780435
- VilsbollTKrarupTDeaconCMadsbadSHolstJReduced postprandial concentrations of intact biologically active glucagons-like peptide 1 in type 2 diabetic patientsDiabetes20015060961311246881
- LangleyAKSuffolettaTJJenningsHRDipeptidyl peptidase IV inhibitors and the incretin system in type 2 diabetes mellitusPharmacotherapy20072781163118017655515
- KarasikAAschnerPKatzeffHDaviesMSteinPSitagliptin, a dpp-4 inhibitor for the treatment of patients with type 2 diabetes: a review of recent clinical trialsCurr Med Res Opin200824248949618182122
- BrazgRXuLManCEffect of adding sitagliptin, a dipeptidyl peptidase-4 inhibitor, to metformin on 24-h glycemic control and β-cell function in patients with type 2 diabetesDiabetes Obes Metab2007918619317300594
- GoldsteinFeinglosMLuncefordJEffect of initial combination therapy with sitagliptin, a dipeptidyl peptidase-4 inhibitor, and metformin on glycemic control in patients with type 2 diabetesDiabetes Care20073081979198717485570
- CharbonnelKarasikALiuJEfficacy and safety of the dipeptidyl peptidase-4 inhibitor sitagliptin added to ongoing metformin therapy in patients with type 2 diabetes inadequately controlled with metformin aloneDiabetes Care200629122638264317130197
- KarasikAWuMWilliams-HermanDSitagliptin added to ongoing metformin therapy provides sustained glycemic control over 54 weeks, with a low incidence of hypoglycemia and with weight loss (abstract 0523-P)Diabetes Care2005281083109115855571
- NauckMMeiningerGShengDEfficacy and safety of the dipeptidyl peptidase-4 inhibitor, sitagliptin, compared with the sulfonylurea, glipizide, in patients with type 2 diabetes inadequately controlled on metformin alone: a randomized, double-blind, noninferiority trialDiabetes Obes Metab2007919420517300595
- HermansenKKipnesMLuoEEfficacy and safety of the dipeptidyl peptidase-4 inhibitor, sitagliptin, in patients with type 2 diabetes mellitus inadequately controlled on glimepiride alone or on glimepiride and metforminDiabetes Obes Metab2007973374517593236
- RosenstockJBrazgRAndryukPEfficacy and safety of the dipeptidyl peptidase-4 inhibitor sitagliptin added to ongoing pioglitazone therapy in patients with type 2 diabetes: a 24-week, multicenter, randomized, double-blind, placebo-controlled, parallel-group studyClin Ther200628101556156817157112
- VanDeKoppelSChoeHMSweetBVManaged care perspective on three new agents for type 2 diabetesJ Manag Care Pharm200814436338018500914
- HermanGABergmanAYiBKipnesMfor the sitagliptin study 012 groupTolerability and pharmacokinetics of metformin and the dipeptidyl peptidase-4 inhibitor sitagliptin when co-administered in patients with type 2 diabetesCurr Med Res Opin200622101939194717022853
- FlorentinMLiberopoulosENMikhailidisDPElisafMSSitagliptin in clinical practice: a new approach in the treatment of type 2 diabetesExpert Opin Pharmacother20089101705172018570604
- Janumet package insertWhitehouse Station, NJMerck and company2008 http://www.merck.com/product/usa/pi_circulars/j/janumet/janumet_pi.pdf
- Glucophage (metformin), package insertPrinceton, NJBristol-Myers Squibb Company2008 http://packageinserts.bms.com/pi/pi_glucophage.pdf
- Januvia package insertWhitehouse Station, NJMerck and company2008 http://www.merck.com/product/usa/pi_circulars/j/januvia/januvia_pi.pdf
- NathanDMBuseJBDavidsonMBManagement of hyperglycemia in Type 2 Diabetes: A consensus algorithm for the initiation and adjustment of therapy. A consensus statement from the American Diabetes Association and the European Association for Study of DiabetesDiabetes Care20062981963197116873813
- KrentzAJBaileyCJOral antidiabetic agents current role in type 2 diabetesDrugs200565338541115669880
- NathanDMBuseJBDavidsonMBMedical management of hyperglycemia in Type 2 Diabetes: A consensus algorithm for the initiation and adjustment of therapy. A consensus statement from the American Diabetes Association and the European Association for Study of DiabetesDiabetes Care20083112111
- NathanDMBuseJBDavidsonMBManagement of hyperglycemia in Type 2 Diabetes: A consensus algorithm for the initiation and adjustment of therapy. Update regarding thiazolidinediones: a consensus statement from the American Diabetes Association and the European Association for Study of DiabetesDiabetes Care200831117317518165348
- NissenSEWolskiKEffect of rosiglitazone on the risk of myocardial infarction and death from cardiovascular causesN Engl J Med200735611517202448
- SinghSLokeYKFurbergCDLong-term risk of cardiovascular events with rosiglitazone: a meta-analysisJAMA2007298101189119517848653