Abstract
Inhibition of dipeptidyl peptidase-4 (DPP-4) prevents the inactivation of glucagonlike peptide-1 (GLP-1). This increases circulating levels of active GLP-1, stimulates insulin secretion and inhibits glucagon secretion, which results in lowering of glucose levels and improvement of the glycemic control in patients with type 2 diabetes. This review summarizes experiences with DPP-4 inhibition in the treatment of type 2 diabetes, with a focus on sitagliptin. Sitagliptin has in several clinical studies been shown to improve metabolic control in type 2 diabetes, both when used as monotherapy and when used in combination with metformin, sulfonylurea, thiazolidinediones or insulin. The reduction in HbA1c is ≈ 0.6% to 1.0% from baseline levels of 7.5% to 8.7% over 6 to 12 months therapy. Sitagliptin has a favorable safety profile, is highly tolerable, and there is a minimal risk of hypoglycemia. Furthermore, sitagliptin is body weight neutral or induces a slight body weight reduction. Sitagliptin may be used in the early stages of type 2 diabetes in combination with metformin or other treatments in subjects with inadequate glycemic control on these treatments alone. Sitagliptin may also be used in monotherapy and, finally, sitagliptin may be used in combination with insulin in more advanced stages of the disease.
Introduction
Hyperglycemia is a key factor underlying complications of type 2 diabetes, and, therefore, reducing hyperglycemia is a critical aim of treatment of the disease. Improving hyperglycemia has thus been shown to reduce the risk of microvascular complications and may also reduce macrovascular complications.Citation1,Citation2 The basis for treatment is lifestyle changes with increased physical activity and dietary modifications. If these treatments are not sufficient, pharmacological treatment with metformin is recommended.Citation3 However, due to the progressive nature of the disease, additional pharmacological treatment is often required. Several options exist: sulfonylureas, thiazolidinediones, meglitinides, α-glucosidase inhibitors and insulin.Citation3,Citation4 There are, however, limitations with these pharmacological treatments, such that even with aggressive treatment using these approaches, glycemic control often deteriorates. Furthermore, current therapy is often associated with adverse events. These adverse events include hypoglycemia with sulfonylureas and insulin, gastrointestinal discomfort with biguanides (such as metformin), and increased body weight, edema and cardiac insufficiency with thiazolidinediones.Citation5–Citation8 Furthermore, the current therapies do not target all pathophysiological aspects of type 2 diabetes. Thus, dysregulation of glucose metabolism in type 2 diabetes is caused by a combination of insulin resistance, impaired insulin secretion, augmented glucagon secretion and reduced β-cell mass.Citation9–Citation12 Whereas insulin resistance is treated by biguanides and thiazolidinediones, and insulin secretion is treated by sulfonylureas, no therapy treats the hypersecretion of glucagon and the reduced β-cell mass. There are thus several unmet needs in the treatment of diabetes which urge the development of novel treatment.
Recently, several new approaches have emerged to meet these challenges. These novel therapies include the amylin analog pramlintide and the GLP-1 receptor agonists, including exenatide and liraglutide.Citation13–Citation15 Another novel class of compounds is inhibitors of the enzyme dipeptidyl peptidase- 4 (DPP-4). The DPP-4 inhibitors, which prevent the inactivation of the incretin hormones glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP), increase the endogenous concentrations of these hormones which prolongs their actions and improves glycemia. Citation16–Citation20 Several DPP-4 inhibitors have been developed and are in various stages of clinical development. Sitagliptin, vildagliptin and saxagliptin are approved for use in several countries.Citation20 This article reviews evidence for clinical use of DPP-4 inhibitors, with a focus on sitagliptin.
Incretin-based therapy
GLP-1 is released from the gut following meal ingestion and GLP-1 in turn stimulates insulin secretion and inhibits glucagon secretion, which reduces glucose levels.Citation16,Citation17 GLP-1 is, however, rapidly inactivated by the enzyme DPP-4, which cleaves the two N-terminal amino acids of the hormone making it largely inactive.Citation16 This process is efficient; the half-life of active GLP-1 is less than 2 minutes. Inhibition of DPP-4 prevents therefore the rapid inactivation of GLP-1. A major mechanism underlying the antidiabetic action of the DPP-4 inhibitors is thus the increased concentrations of active GLP- 1 as has been demonstrated by vildagliptin following meal ingestion.Citation21 As a consequence, DPP-4 inhibition increases insulin secretion and inhibits glucagon secretion, which results in inhibition of hepatic glucose production, as demonstrated for vildagliptin.Citation21–Citation23 These actions reduce both fasting and prandial glucose levels and the 24-hour glucose profile, as has been shown for NVP-DPP728 and sitagliptin.Citation24,Citation25 Rodent studies have also shown that DPP-4 inhibitors (vildagliptin and sitagliptin) increase islet mass and normalize islet cell topography in diabetes models in mice.Citation26,Citation27 This would suggest that DPP-4 inhibition targets the important islet dysfunctions in type 2 diabetes. It should be emphasized, however, that no evidence of increased β-cell mass by DPP-4 inhibitors exists in humans.
DPP-4 inhibition has been shown to be efficient in improving glycemia both as monotherapy and as add-on to metformin, sulfonylurea and thiazolidinediones in subjects with inadequate glycemic control. DPP-4 inhibition has also been shown to be safe, highly tolerated and body-weight neutral.Citation18–Citation20 In fact, DPP-4 inhibition meets several of the challenges of the treatment of today – it improves glycemia with little risk for hypoglycemia, it does not increase body weight, it is safe with very little risk for adverse events, and, due to its targeting of the key islet defects, it has the potential to modify the disease process.
Sitagliptin – pharmacokinetics and mechanisms of action
Structure and pharmacokinetics
Sitagliptin is a triazolopiperazine derivative ().Citation10 It is orally active and it selectively and reversibly inhibits DPP-4 compared to inhibition of other members of the DPP family. Thus, in vitro studies have shown that at 18 nmol/L, sitagliptin inhibits DPP-4 by 50% whereas 48 μmol/L is required to inhibit DPP-8 by 50% and >100 μmol/L is required to inhibit DPP-9 by 50%Citation28 The pharmacokinetics of sitagliptin have been examined in both healthy subjectsCitation29 and in subjects with type 2 diabetesCitation30 with no difference between these groups. Sitagliptin is rapidly absorbed after oral ingestion with an 87% bioavailability after intake of a single 100 mg tablet.Citation31 Cmax is observed within 1 to 2 hours and the half-life of the compound is ≈12 hours.Citation31 Sitagliptin is minimally metabolized and ≈80% of the compound is excreted unchanged in the urine.Citation32 Renal excretion is achieved through a combination of active secretion and glomerular filtration.Citation29 Renal insufficiency increases circulating levels of sitagliptin in that plasma levels of sitagliptin are increased by 2-fold in patients with moderate renal impairment (creatinine clearance 30–50 mL/min) and by 4-fold in patients with severe renal impairment (creatinine clearance <30 mL/min), making dose adjustements recommended in these patients.Citation33 Hepatic insufficiency, obesity and old age do not seem to alter the pharmacokinetics of sitagliptin and no drug interactions have been observed for the compound.
Figure 1 Structure of sitagliptin.
Mechanisms of action
Sitagliptin rapidly inhibits DPP-4 after oral ingestion, and within 1 hour, DPP-4 activity, as determined in plasma, is inhibited by more than 90%.Citation30 The duration of DPP-4 inhibition is such that the drug can be dosed once daily. The inhibition of DPP-4 activity is dose-dependent and is sustained after multiple dosages, as demonstrated in studies up to 28 days.Citation30,Citation33,Citation34 Active GIP and GLP-1 levels are increased by sitagliptin by approximately 2- to 3-fold after meal ingestion or oral glucose.Citation30,Citation33,Citation34 This results in increased insulin secretion as judged from increased insulinogenic indexCitation35–Citation40 and the homeostasis model of assessment of β-cell function (HOMA-β).Citation36–Citation46 Improved β-cell function is also evident from reduced proinsulin to insulin ratio.Citation38,Citation41–Citation44,Citation47 Sitagliptin also reduces glucagon levels,Citation25,Citation30 although this needs to be examined in more detail. The improved islet function by sitagliptin results in reduction of both fasting glucose and prandial glucose as revealed in different studies in subjects with type 2 diabetes.Citation25,Citation36,Citation48,Citation49 In fact, the entire 24-hour glucose profile is reduced by sitagliptin, as is evident from a study examining addition of sitagliptin to ongoing metformin therapy compared to metformin treatment alone ().Citation25
Figure 2 24-hour plasma glucose profile in patients with type 2 diabetes after four weeks treatment with sitagliptin (100 mg daily) added to ongoing treatment with metformin compared to patients continued with metformin alone. Reproduced with permission from Brazg R, Xu L, Dalla Man C, et al. Effect of adding sitagliptin, a dipeptidyl peptidase-4 inhibitor, to metformin on 24-h glycaemic control and beta-cell function in patients with type 2 diabetes. Diabet Obes Metab. 2007; 9:186–193.Citation25 Copyright © 2007 Wiley-Blackwell.

Sitagliptin – clinical effects in monotherapy
Placebo-controlled studies
Sitagliptin was initially evaluated as monotherapy for 12 weeks in dose-findings studies in drug-naïve patients with type 2 diabetes. At the dose of 100 mg, hemoglobin A1c (HbA1c) was reduced by sitagliptin by 0.6% from a baseline of 7.7% in one study comprising 555 subjectsCitation50 and by 0.8% from a baseline of 7.8% in another study of 743 subjects.Citation45 A subsequent placebo- controlled, multi-center 18-week study in 521 patients showed that sitagliptin at 100 mg or 200 mg once daily reduced HbA1c by 0.6% and 0.5%, respectively, from a baseline of 8.1%Citation42 and a 24-week study using sitagliptin at 100 mg or 200 mg daily in drug-naïve patients with a mean baseline HbA1c of 8.0% (n =741) showed a reduction of 0.8% and 0.9%, respectively.Citation41 The improved glycemia during monotherapy with sitagliptin is sustained over at least 2 years, as shown in a 52-week study with an open label extension for another 52 weeks: sitagliptin at 100 mg had after 2 years reduced HbA1c by 0.7% from a baseline of 7.5%.Citation51 Sitagliptin has also been shown to efficiently improve glycemic control when used in monotherapy in a study comprising 530 Asian patients. Thus, one study showed that sitagliptin at 100 mg daily reduced HbA1c by 1.4% in Indians, by 1.4% in Koreans and by 0.7% in Chinese subjects with type 2 diabetes from baseline levels of 8.7% during 18 weeks treatment.Citation35 Furthermore, in a study in 151 Japanese patients, sitagliptin at 100 mg daily reduced HbA1c by 0.7% from a baseline of 7.5% over a study period of 12 weeks in subjects with type 2 diabetes.Citation36
Since sitagliptin is cleared by the kidney, dose adjustments are required in subjects with moderate or severe renal insufficiency. One study examined the 54-week efficacy and safety of sitagliptin as monotherapy in subjects with type 2 diabetes with moderate (dose 50 mg daily) or severe (dose 25 mg daily) renal insufficiency. Mean baseline HbA1c was 7.7% and sitagliptin reduced HbA1c by 0.7%, ie, similar to those in other studies.Citation52 Furthermore, sitagliptin was safe and well tolerated in the subjects with renal insufficiency, with a lower risk of hypoglycemia relative to glipizide and with weight loss compared with weight gain with glipizide. Another study has examined the influence of sitagliptin in elderly patients. In this placebo-controlled study of 123 patients with type 2 diabetes above 65 years of age, sitagliptin at 100 mg over 24 weeks reduced HbA1c by 0.7% from a baseline of 7.8%.Citation53 Sitagliptin was well tolerated in the elderly with low degree of adverse events and hypoglycemia occurring only in one subject, compared to two subjects treated with placebo.
Sitagliptin – clinical effects when used in combination with metformin
Add-on to ongoing metformin
Sitagliptin has been shown to improve glycemic control when added to metformin in subjects with type 2 diabetes who are inadequately controlled when treated with metformin alone. One study showed that in patients with ongoing metformin treatment (n =701) with a mean baseline HbA1c of 8.0%, sitagliptin at 100 mg daily during 24 weeks, reduced HbA1c by 0.7% when compared to subjects who maintained treatment with metformin alone.Citation44 Sitagliptin progressively reduced HbA1c levels during the first 12 weeks of treatment, and a sustained level was established thereafter. Also in Japanese patients, sitagliptin improves glycemic control when added to ongoing metformin treatment; the placebo-adjusted reduction in HbA1c by sitagliptin was 0.7%; baseline HbA1c was 7.8%.Citation37
Comparison with active comparator
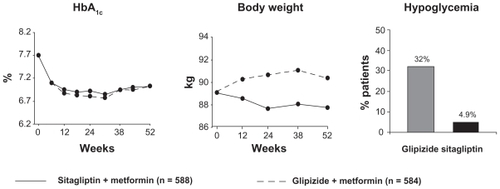
One study compared the effect of sitagliptin (100 mg daily) with that of glipizide (up to 20 mg daily) when added to ongoing treatment with metformin for a study period of 52 weeks in a total of 1172 patients with type 2 diabetes with a mean baseline HbA1c of 7.5%.Citation54 HbA1c was reduced similarly by 0.7% in both groups (). Sitagliptin (100 mg once daily) has also been compared with rosiglitazone (8 mg daily) when added to ongoing metformin in subjects with inadequate glycemic control with metformin alone (mean HbA1c 7.7%; n =273). After 18 weeks, HbA1c was reduced by 0.7% by sitagliptin and by 0.8% by rosiglitazone; the difference was not significant.Citation55
Figure 3 Mean HbA1c, mean body weight and percentage of patients with at least one event of hypoglycemia during 52 weeks treatment with sitagliptin (100 mg daily) or glipizide as add-on to metformin in patients with type 2 diabetes. Reproduced from Nauck MA, Meininger G, Sheng D, Terranella L, Stein PP. Efficacy and safety of the dipeptidyl peptidase-4 inhibitor, sitagliptin, compared with the sulfonylurea, glipizide, in patients with type 2 diabetes inadequately controlled on metformin alone: a randomized, doubleblind, non-inferiority trial. Diabet Obes Metab. 2007; 9:194–205.Citation54 Copyright © 2007 Wiley-Blackwell.
Initial combination with metformin
One study has examined the initial combination of sitagliptin (100 mg daily) and metformin (1 or 2 g daily) compared to monotherapy treatment with sitagliptin or metformin alone for 24 weeks (n =1091) in subjects with mean baseline HbA1c of 8.8%.Citation43 Approximately half of the patients were drugnaïve, whereas the other half had received oral agents before. There was a marked reduction in HbA1c after combination therapy (by 1.6% and 2.1% in the two groups differing in metformin dose, respectively).Citation43 This study continued as an open-label extension for 104 weeks, thus providing 2-year data on sitagliptin when given in combination with metformin. A total of 1091 patients were included at start of the study, 587 entered the extension and 402 were included in the final analysis. Reduction from baseline HbA1c was 1.4% and 1.7% in the two groups, respectively.Citation51
Sitagliptin – clinical effects in combination with agents other than metformin
Combination with pioglitazone
Sitagliptin has been evaluated as add-on to ongoing treatment with pioglitazone in one placebo-controlled, 6-month study.Citation47 The study evaluated addition of sitagliptin (100 mg daily) to pioglitazone at 30 or 45 mg daily versus continuation with pioglitazone alone in patients with a mean baseline HbA1c of 8.0% (n =353). Sitagliptin reduced HbA1c by 0.7% versus pioglitazone alone.Citation47 Similar results of improved glycemic control when sitagliptin was added to ongoing pioglitazone treatment were also demonstrated in Japanese patients.Citation39
Combination with glimepiride
Sitagliptin has as well been evaluated as add-on to ongoing treatment with glimepiride in a 6-month study of 441 patients with a mean baseline HbA1c of 8.3%. Sitagliptin (100 mg daily) reduced HbA1c by 0.7% when adjusted for changes in the group continuing with glimepiride alone.Citation46
Combination with insulin
One study evaluated the influence of sitagliptin (100 mg daily) when added to ongoing insulin therapy in a total of 617 patients with type 2 diabetes.Citation56 Mean baseline HbA1c was 8.7% and following addition of sitagliptin to the ongoing insulin therapy, HbA1c was reduced by 0.6% versus no change (0.0%) in patients who continued with insulin treatment alone.
Sitagliptin – clinical effects when used in triple therapy
Combination with metformin and sulfonylurea
A 6-month study evaluated addition of sitagliptin (100 mg daily) to a total of 441 patients with ongoing treatment with the combination of metformin and glimepiride with a baseline HbA1c of 8.3%.Citation46 It was found that HbA1c was reduced by 0.9% by sitagliptin compared to ongoing therapy with metformin and glimepiride.
Combination with metformin and thiazolidinediones
One study has examined the effect of addition of sitagliptin (100 mg daily) to ongoing therapy with metformin in combination with rosiglitazone in a total of 277 patients with type 2 diabetes with a mean baseline HbA1c of 8.8%.Citation57 The addition of sitagliptin reduced HbA1c by 0.9% versus a reduction by 0.2% in patients who continued on metformin and rosiglitazone.
Clinical effects of sitagliptin – summary
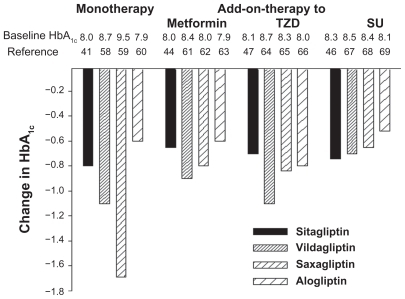
The clinical trials show efficient and sustained (up to 2 years) improvement of glycemic control of sitagliptin both in monotherapy and in combination with metformin, glimepiride, pioglitazone and insulin and also improved effect when used in triple therapy together with metformin plus glimepiride or metformin plus rosiglitazone. In general, HbA1c was reduced by sitagliptin by ≈0.6% to 1.0% from baseline levels of 7.5% to 8.8%. An active comparative study has shown similar effect as glipizide when added to metformin.Citation54 The effect of sitagliptin seems to be similar to other DPP-4 inhibitors, although head-to-headstudies have not been undertaken.Citation41,Citation44,Citation46,Citation47,Citation58–Citation69 shows the reduction in HbA1c during 24- to 26-week studies with four different DPP-4 inhibitors as monotherapy or in combination with metformin, a sulfonylurea or a thiazolidinedione. Initial HbA1c levels differed in the different studies; overall no clear difference between the various DPP-4 inhibitors is evident.
Figure 4 Changes in HbA1c during 24–26 weeks treatment with four different DPP-4 inhibitors in clinical trials, as monotherapy or as add-on to metformin, a thiazolidinedione (TZD) or a sulfonylurea (SU). Baseline HbA1c levels above column.
Sitagliptin – safety and tolerability
Adverse events
The extensive experience with DPP-4 inhibition that now exists in clinical trials shows high tolerability and safety. This is evident from results in several studies with a number of different DPP-4 inhibitors, which show that the number of adverse events is not increased in study groups treated with DPP-4 inhibitors compared to placebo groups, and the drop out rates from studies due to adverse events are low. This is evident also for sitagliptin,Citation35–Citation57 and notably also in elderly patientsCitation53 and in patients with moderate or severe renal insufficiency.Citation52 A meta-analysis has been published in regard to adverse events with sitagliptin in 12 large, doubleblind studies with durations from 18 weeks to 2 years.Citation70 The meta-analysis comprised a total of 3415 patients treated with sitagliptin (100 mg daily) and 2724 controls, who were treated either with other antihyperglycemic agents or placebo. The overall incidence of adverse events in these studies was 63% in patients given sitagliptin versus 63% in controls, ie, the same degree of total number of events. Serious adverse events were also similar in the two groups (7%) as was the number of patients who discontinued therapy (35% vs 36%) or withdrew from the studies due to adverse events (3% vs 4%). Some adverse events occurred, however, during the treatment with sitagliptin, although the pattern differed between different studies. When used as add-on to metformin adverse events were absent more frequently with sitagliptin versus metformin alone. When used as initial combination with metformin or as add-on to thiazolidinedione, the most frequent adverse events occurring more commonly in the sitagliptin group were headache and upper respiratory tract infection (5%–6% vs 3%–5% with metformin or thiazolodinedione alone), and most frequent adverse events for sitagliptin when combined with sulfonylurea were hypoglycemia (12% vs 2%), nasopharyngitis (6% vs 5%) and headache (6% vs 2%). Furthermore, sitagliptin seems to be safe from a cardiovascular point of view, since adverse events suggestive of cardiac disorders (such as acute coronary syndrome, acute myocardial infarction or angina pectoris) were absent more frequently in patients treated with sitagliptin versus comparators or placebo.Citation70
Following the reports of acute pancreatitis in subjects treated with exenatide or sitagliptin, concern has been raised that incretin based therapy is associated with increased risk of acute pancreatitis. This is difficult to establish because there is a generalized increased risk of acute pancreatitis in patients with diabetes, obesity or hyperlipemia. A claims-based drug surveillance system has, however, shown that the risk for pancreatitis is not higher when patients are treated with sitagliptin (or exenatide) than when treated with metformin or sulfonylurea.Citation71 Also a few serious hypersensitivity reactions have been reported during treatment with sitagliptin. Therefore, although being extremely well tolerated in studies up to 2 years, long-term surveillance is of importance for the detection of potential adverse events that might occur at later stages or infrequently during treatment with sitagliptin.
Hypoglycemia
Hypoglycemia is rare (<3%) during treatment with DPP-4 inhibitors as monotherapy or in combination with metformin or thiazolidinediones.Citation35–Citation38,Citation41–Citation45,Citation47,Citation53 The low degree of hypoglycemia is especially seen when compared with the risk of hypoglycemia during treatment with sulfonylurea (). This is explained by the glucose-dependency of the islet effects of GLP-1; hence when glucose levels are reduced the effects of GLP-1 in stimulating insulin secretion and inhibiting glucagon secretion vanish. In contrast, hypoglycemia was shown to be more common when sitagliptin was added to ongoing glimepiride; the incidence of hypoglycemia was 12% versus 2% in the group given glimepiride alone.Citation46 The potential risk for hypoglycemia when combining sitagliptin and sulfonylureas may be due to an uncoupling mechanism of sulfonylureas of the glucose dependency of the islet actions by GLP-1.Citation72 This risk needs, however, to be evaluated in more detail. If increased frequency of hypoglycemia when combining sitagliptin with a sulfonylurea is confirmed, a clinical consequence is that the dose of sitagliptin or sulfonylureas should be reduced when these are used in combination. Similarly, when combined with insulin, there was an increased risk for hypoglycemia by sitagliptin.Citation56
In spite of the very low risk of hypoglycemia during treatment with DPP-4 inhibition, a concern might be that if hypoglycemia nevertheless evolves, DPP-4 inhibition might compromise the counterregulation, if it is associated with inhibition of glucagon secretion also under these conditions. A recent study addressed this by examining the glucagon response to hypoglycemia in patients treated with the DPP- 4 inhibitor vildagliptin.Citation73 It was found that contrary to the inhibition of glucagon secretion after meal ingestion by vildagliptin, ie, when glucose levels are elevated, the glucagon response to hypoglycemia was not inhibited.Citation72 This preserved glucagon secretion during hypoglycemia in patients treated with vildagliptin suggests that DPP-4 inhibition prevents hypoglycemia. This prevention may be due to improved glucose sensing in the α-cells such that DPP-4 inhibition, through GLP-1, restores and improves the action of glucose on glucagon secretion, ie, it augments the inhibition of glucagon secretion at high glucose but exaggerates the stimulation of glucagon secretion at low glucose. A similar study with sitagliptin is warranted to examine whether sitagliptin, like vildagliptin, would prevent hypoglycemia.
Sitagliptin – other potential effects
Body weight
Many studies show that sitagliptin is body weight neutral. Citation41–Citation47,Citation51,Citation54,Citation57 Therefore, when compared to thiazolidinediones, sulfonylureas and insulin, DPP-4 inhibition shows advantage compared to the increase in body weight which is associated with these other treatments. This is clearly evident when compared with glipizide, which increased body weight, whereas sitagliptin was body weight neutral over a study period of 52 weeks ( Citation54).
Lipids
In clinical studies with sitagliptin, there has been either no significant change in lipidsCitation42,Citation47 or small beneficial effects on blood lipids.Citation44,Citation45 The two studies reporting effects showed that when sitagliptin was added to metformin, total cholesterol was reduced by 3% to 6%, triglycerides were reduced by 17%, non-high-density lipoptrotein (HDL)-cholesterol was reduced by 10% to 19% and HDL-cholesterol was increased by 2%.Citation44,Citation45 Potential long-term effects of sitagliptin on lipids remain to be established.
Sitagliptin – regulatory aspects
Sitagliptin (Januvia®; Merck) was approved by the Food and Drug Administration (FDA) in October 2006 and by the European Medicines Agency (EMEA) in April 2007. It is at present approved in 85 countries throughout the world. It is indicated for use as monotherapy and in combination therapy. As monotherapy, the indication in the US is as an adjunct to diet and exercise to improve glycemic control in patients with type 2 diabetes, whereas in the EU, it is indicated as monotherapy in patients who have inadequate glycemic control with diet and exercise and in whom metformin is inappropriate due to contraindications or intolerance. Sitagliptin is also indicated, both in the US and in EU, in combination therapy with metformin, a sulfonylurea or a thiazolidinedione in patients who have inadequate control with these agents used as single agents plus diet and exercise. Recently, sitagliptin was also approved to be used in combination with insulin. Sitagliptin is also indicated as triple therapy in combination with metformin plus a sulfonylurea or metformin plus a thiazolidinedione in patients who have inadequate glycemic control with the two agents.
The recommended dose for sitagliptin is 100 mg daily as a single tablet. When used as add-on to metformin or thiazolidinediones, the doses of these agents can be maintained, whereas when added to a sulfonylurea it is recommended that the dose of the sulfonylurea is reduced. Sitagliptin exists also as a combination tablet with metformin. The tablets contain 50 mg sitagliptin and 850 mg metformin (Janumet®). The recommended dose of these tablets is twice daily, which is equivalent to 100 mg sitagliptin daily.
In the US the dose of sitagliptin is recommended to be lowered in subjects with renal insufficiency: 50 mg daily in moderate renal insufficiency (creatinine clearance 30-50 mL/min), and 25 mg daily in severe renal insufficiency (creatinine clearance <30 mL/min). In the EU, sitagliptin is not recommended in subjects with renal insufficiency.
Conclusions and clinical positioning of sitagliptin
DPP-4 inhibition as a novel therapy of type 2 diabetes improves islet function due to the increased concentrations of active GLP-1, which stimulates insulin secretion and inhibits glucagon secretion. Since these effects target main pathophysiologic defects in type 2 diabetes, DPP-4 inhibition is a treatment targeting pathophysiologically relevant aspects of the disease. The therapy therefore holds the promises of improving basis of the disease and may therefore be the solution to several of the currently unmet needs for treatment of the disease. Clinical trials also show the efficacy of the strategy, and the safety profile shows low risk for adverse events or hypoglycemia. DPP-4 inhibition is therefore a novel and promising paradigm for treatment of type 2 diabetes.
Sitagliptin is a DPP-4 inhibitor which has shown good clinical effect in reducing glycemia both as monotherapy and in combination with other oral agents and with insulin. Sitagliptin may be of greatest value as add-on to ongoing metformin in patients with inadequate glycemic control when treated with metformin alone or as monotherapy in subjects in whom metformin is contraindicated or in subjects with adverse events from metformin. Initial combination with DPP-4 inhibitors and metformin in drug-naïve patients requiring pharmacological treatment for glycemic control, would be another place of the therapy. The reason for this is that sitagliptin improves pathophysiological defects which are seen early during the progression of diabetes, mainly the islet dysfunction, in association with safety and high tolerability. In particular, the occurrence of hypoglycemia is rare, which makes it of special interest in early stages as well as in elderly patients.
DPP-4 inhibition may be of greatest impact as add-on to metformin in patients with inadequate control of glycemia when treated with metformin alone. The clinician may in such a situation select between a DPP-4 inhibitor and a sulfonylurea. It is therefore of interest that when directly comparing sitagliptin versus glipizide when added to metformin in such patients, the reduction in HbA1c was the same over a 6 month but yet important differences existed.Citation54 Thus, whereas glipizide increased body weight, sitagliptin reduced body weight, and whereas glipizide resulted in several events of hypoglycemia, this was rare with sitagliptin ( Citation54). A similar finding was recently reported also for vildagliptin after 1 year of treatment when added to metformin versus glimepiride.Citation74 Hence, although long term comparisons are required, DPP-4 inhibition offers a better outcome than sulfonylurea when added to metformin over a duration of 6 months to 1 year.
Sitagliptin may also be exchanged for sulfonylurea or thiazolidinediones in combination with metformin in subjects with intolerance to sulfonylurea or thiazolidindediones or with inadequate glycemic control with these combinations. This might also be a useful indication, considering the limitation when using sulfonylureas or thiazolidinediones in terms of adverse events. Furthermore, DPP-4 inhibition has also an important place as add-on to sulfonylurea or thiazolidinediones in subjects with inadequate glycemic control when treated with these agents alone. A potential future combination is DPP-4 inhibition plus insulin, in more advanced stages of the disease. Hence, DPP-4 inhibition may be used both in early stages of the diseases, as monotherapy or in combination therapy, as well as in more advanced stages of the disease. This is in line with a recent algorithm for glycemic control as stated by an American Association of Clinical Endocrinologists/American College of Endocrinology Consensus Panel.Citation75
The evidence for the beneficial effect of sitagliptin is its efficacy in improving glycemic control in studies over 6 to 12 months in association with safety and low risk of adverse events. The long-term durability is now important to consider and of high importance for the future long-term value of this class of compounds. Whether sitagliptin may have additional beneficial effects on islet mass, as has been shown in rodents,Citation26 remains to be established in humans.
In the clinical context, sitagliptin offers similar indication as the other DPP-4 inhibitors and the GLP-1 receptor agonists. Sitagliptin is very similar to the other DPP-4 inhibitors on the market, vildagliptin and saxagliptin,Citation20 and no long-term head-to-head study exists yet for these; it is therefore not possible yet to differentiate between them. Of the GLP-1 receptor agonists (GLP-1 mimetics), exenatide (Byetta®; Amylin and Eli Lilly) and liraglutide (Victoza®; Novo Nordisk) have been approved for therapy and several others are in clinical development, such as lixisenatide, albiglutide and taspoglutide. They are DPP-4 resistant compounds which are based either on modification of the GLP-1 molecule or based on the peptide exendin-4.Citation76 The GLP-1 mimetics are given through the subcutanoues route either once or twice daily or with longer intervals, such as once weekly. The efficacy of these compounds seems to be similar as that of the DPP-4 inhibitors. The main differences are that GLP-1 receptor agonists reduce body weight, whereas DPP-4 inhibitors are body weight neutral; that GLP-1 mimetics are injectables, whereas DPP-4 inhibitors are active after oral administration; and that DPP-4 inhibitors are virtually free from adverse events, whereas GLP-1 mimetics are associated with nausea.
Sitagliptin, like the other DPP-4 inhibitors, has a higher cost per day of clinical use than sulfonylureass, which is an economic drawback for the DPP-4 inhibitors. However, a health economic model analysis has shown that addition of sitagliptin to metformin was cost saving compared to sulfonylurea or a thiazolidinedione in patients with inadequate glycemic control on metformin alone.Citation77 Nevertheless, more studies are required on this issue.
For future studies, it is important to examine the durability and long-term effects and safety of sitagliptin. Studies are also required to compare the long-term effects in head-to-head studies with other DPP-4 inhibitors and with GLP-1 mimetics. Moreover, outcome studies in relation to co-morbidity, such as cardiovascular diseases, are required. Recently, Merck and Co. has initiated a clinical cardiovascular study with sitagliptin entitled “A randomized placebo controlled clinical trial to evaluate cardiovascular outcomes after treatment with sitagliptin in patients with type 2 diabetes mellitus and inadequate glycemic control on mono- or dual combination oral antihyperglycemic therapy” (TECOS).Citation78 This is a long-term event-driven study with the primary objective of evaluating cardiovascular endpoints in high-risk populations; results are expected in 2014. Furthermore, more mechanistic studies are required to establish more detailed information on how sitagliptin affects islet function, including effects on glucagon secretion, and also effects on incretin hormone secretion and metabolism; most mechanistic studies on DPP-4 inhibition exist for vildagliptin.Citation79 Studies directed at establishing potential contribution of the incretin hormone GIP, the level of which also is increased by DPP-4 inhibition. Finally, since sitagliptin relies on incretins which are released after meal ingestion, it is important to study their effects in relation to ingestion of various meal ingredients, since it is known that macronutrients have different effects on the release and concentrations of incretin hormones.Citation80 Therefore, although much information exists on clinical effects and mechanisms of DPP-4 inhibition, more information is required for a fuller understanding of this promising concept to treat subjects with type 2 diabetes.
Disclosure
The author has received consulting fees from Merck, Novartis, AstraZeneca, GSK, Roche, Sanofi-Aventis and Servier.
References
- Fonseca V Clinical significance of targeting postprandial and fasting hyperglycemia in managing type 2 diabetes mellitus Curr Med Res Opin 2003 19 635 641 14606987
- Skyler JS Bergenstal R Bonow RO Intensive glycemic control and the prevention of vardiovascular events: implications of the ACCORD, ADVANCE, and VA Diabetes Trials: a position statement of the American Diabetes Association and a Scientific Statement of the American College of Cardiology Foundation and the American Heart Association J Am Coll Cardiol 2009 53 298 304 19147051
- Nathan DM Buse JB Davidson MB Medical management of hyperglycemia in type 2 diabetes: a consensus statement of the American Diabetes Association and the European Association for the Study of Diabetes Diabetes Care 2009 32 193 203 18945920
- Owens DR Zinman B Bolli GB Insulins today and beyond Lancet 2001 358 739 746 11551598
- Hsia SH Davidson MB Established therapies for diabetes mellitus Curr Med Res Opin 2002 18 Suppl 1 S13 21 12365815
- Rendell M The role of sulphonylureas in the management of type 2 diabetes mellitus Drugs 2004 64 1339 1358 15200348
- Diamant M Heine RJ Thiazolidinediones in type 2 diabetes mellitus: current clinical evidence Drugs 2003 63 1373 1405 12825962
- Hussein Z Wentworth JM Nankervis AJ Effectiveness and side effects of thiazolidinediones for type 2 diabetes: real-life experience from a tertiary hospital Med J Austr 2004 181 536 539
- Dunning BE Foley JE Ahrén B Alpha cell function in health and disease: influence of glucagon-like peptide-1 Diabetologia 2005 48 1700 1713 16132964
- Lehy JL Pathogenesis of type 2 diabetes mellitus Arch Med Res 2005 36 197 209 15925010
- Wajchenberg BL β-cell failure in diabetes and preservation by clinical treatment Endocr Rev 2007 28 187 218 17353295
- Inzucchi S Oral antihyperglycemic therapy for type 2 diabetes JAMA 2002 287 360 372 11790216
- Bailey CJ Drugs on the horizon for diabesity Curr Diab Rep 2005 5 353 359 16188170
- Ahrén B Exenatide: a novel treatment of type 2 diabetes Therapy 2005 2 207 222
- Croom KF McCormack PL Liraglutide: a review of its use in type 2 diabetes Drugs 2009 69 1985 2004 19747013
- Drucker DJ Nauck MA The incretin system: glucagon-like peptide-1 receptor agonists and dipeptidyl peptidase-4 inhibitors in type 2 diabetes Lancet 2006 368 1696 1705 17098089
- Ahrén B Glucagon-like peptide-1 (GLP-1): a gut hormone of potential interest in the treatment of diabetes Bioessays 1998 20 642 651 9780839
- Ahrén B DPP-4 inhibitors Best Pract Res Clin Endocrinol Metab 2007 21 517 533 18054733
- Ahrén B Dipeptidyl peptidase-4 inhibitors: clinical data and clinical implications Diabetes Care 2007 30 1344 1350 17337494
- Ahrén B Clinical results of treating type 2 diabetic patients with sitagliptin, vildagliptin or saxagliptin – diabetes control and potential adverse events Best Pract Res Clin Endocrinol Metab 2009 23 487 498 19748066
- Ahrén B Landin-Olsson M Jansson PA Inhibition of dipeptidyl peptidase- 4 reduces glycemia, sustains insulin levels and reduces glucagon levels in type 2 diabetes J Clin Endocrinol Metab 2004 89 2078 2084 15126524
- Ahrén B Pacini G Foley JE Schweizer A Improved meal-related beta-cell function and insulin sensitivity by the dipeptidyl peptidase-IV inhibitor vildagliptin in metformin-treated patients with type 2 diabetes over 1 year Diabetes Care 2005 28 1936 1940 16043735
- Balas B Baig MR Watson C The dipeptidyl peptidase IV inhibitor vildagliptin suppresses endogenous glucose production and enhances islet function after single dose administration in type 2 diabetic patients J Clin Endocrinol Metab 2007 92 1249 1255 17244786
- Ahrén B Simonsson E Larsson H Inhibition of dipeptidyl peptidase IV improves metabolic control over a 4 week study period in type 2 diabetes Diabetes Care 2002 25 869 875 11978683
- Brazg R Xu L Dalla Man C Effect of adding sitagliptin, a dipeptidyl peptidase-4 inhibitor, to metformin on 24-h glycaemic control and beta-cell function in patients with type 2 diabetes Diabet Obes Metab 2007 9 186 193
- Mu J Petrov A Eiermann GJ Woods J Zhou YP Li Z Inhibition of DPP-4 with sitagliptin improves glycemic control and restores islet cell mass and function in a rodent model of type 2 diabetes Eur J Pharmacol 2009 623 148 154 19765579
- Ahrén B Sörhede Winzell M Wierup N DPP-4 inhibition improves glucose tolerance and increases insulin and GLP-1 responses to gastric glucose in association with normalized islet topography in mice with beta-cell specific overexpression of human islet amyloid polypeptide Regul Pept 2007 143 97 103 17482289
- Kim D Wang L Beconi M (2R)-4-oxo-4-[3-(trifluoromethyl-5,6-dihy dro[1,2,4]triazolo[4,3-a]pyrazin-7(8H)-yl]-1-(2,4,5-trifluorophenyl)butan- 2-amine: a potent, orally active dipeptidyl peptidase IV inhibitor for the treatment of type 2 diabetes J Med Chem 2005 48 141 151 15634008
- Herman GA Stevens C van Dyck K Pharmacokinetic and pharmacodynamics of sitagliptin, an inhibitor of dipeptidyl peptidase IV, in healthy subjects: results from two randomized, double-blind, placebo-controlled studies with single oral doses Clin Pharmacol Ther 2005 78 675 688 16338283
- Herman GA Bergman A Stevens C Effect of single oral doses of sitagliptin, a dipeptidyl peptidase-4 inhibitor, on incretin and plasma glucose levels following an oral glucose tolerance test in patients with type 2 diabetes J Clin Endocrinol Metab 2006 91 4612 4619 16912128
- Bergman A Ebel D Liu F Absolute bioavailability of sitagliptin, an oral dipeptidyl peptidase-4 inhibitor, in an oral dipeptidyl peptidase-4 inhibitor, in healthy volunteers Biopharm Drug Dispos 2007 28 315 322 17575559
- Vincent SH Reed JR Bergman AJ Metabolism and excretion of the DPP-4 inhibitor [14C] sitagliptin in humans Drug Metab Dispos 2007 35 533 538 17220239
- Bergman AJ Steven C Zhou Pharmacokinetic and pharmacodynamic properties of multiple oral doses of sitagliptin, a dipeptidyl peptidase IV inhibitor: a double-blind randomized, placebo-controlled study in healthy male volunteers Clin Ther 2006 28 55 72 16490580
- Herman GA Bergman A Liu F Pharmacokinetics and pharmacodynamic effects of the oral DPP-4 inhibitor sitagliptin in middle-aged obese subjects J Clin Pharmacol 2006 46 876 886 16855072
- Mohan V Yang W Son HY Efficacy and safety of sitagliptin in the treatment of patients with type 2 diabetes in China, India and Korea Diab Res Clin Pract 2009 83 106 116
- Nonaka K Kakikawa T Sato A Efficacy and safety of sitagliptin monotherapy in Japanese patients with type 2 diabetes Diabet Res Clin Pract 2008 79 291 298
- Kadowaki T Tajima N Odawara M Nishi M Nonaka K Stein PP Sitagliptin added to ongoing treatrment with metformin improved glycemic control and was well tolerated in Japenese patients with type 2 diabetes Diabetes 2008 Suppl 1 A589 590
- Nonaka K Tsubouchi H Okuyama K Fukao Y Johnson-Levonas AO Amatruda JM Effects of once-daily sitagliptin on 24-h glucose control following 4 weeks of treatment in Japanese patients with type 2 diabetes mellitus Horm Metab Res 2009 41 232 237 19253204
- Kashiwagi A Tajima N Kadowaki T Sitagliptin added to ongoing treatment with pioglitazone improved glycemic control and was well tolerated in Japanese patients with type 2 diabetes Diabetes 2008 Suppl 1 A590
- Tajima N Kadowaki T Odawara M Nishi M Nonaka K Stein PP Sitagliptin added to ongoing treatment with glimepiride improved glycemic control and was well tolerated in Japanese patients with type 2 diabetes Diabetes 2008 57 Suppl 1 A589
- Aschner P Kipnes MS Lunceford JK Sanchez M Mickel C Williams-Herman DE Effect of the dipeptidyl peptidase-4 inhibitor sitagliptin as monotherapy on glycemic control in patients with type 2 diabetes Diabetes Care 2006 29 2632 2637 17130196
- Raz I Hanefeld M Xu L Caria C Williams-Herman D Khatami H Efficacy and safety of the dipeptidyl peptidase-4 inhibitor sitagliptin as monotherapy in patients with type 2 diabetes mellitus Diabetologia 2006 49 2564 25671 17001471
- Goldstein BJ Feinglos MN Lunceford JK Johnson J Williams- Herman DE Effect of initial combination therapy with sitagliptin, a dipeptidyl peptidase-4 inhibitor, and metformin on glycemic control in patients with type 2 diabetes Diabetes Care 2007 30 1979 1987 17485570
- Charbonnel B Karasik A Liu J Wu M Meininger G Efficacy and safety of the dipeptidyl peptidase-4 inhibitor sitagliptin added to ongoing metformin therapy in patients with type 2 diabetes inadequately controlled with metformin alone Diabetes Care 2006 29 2638 2643 17130197
- Scott R Wu L Sanchez M Stein P Efficacy and tolerability of the dipeptidyl peptidase- 4 inhibitor sitagliptin as monotherapy over 12 weeks in patients with type 2 diabetes Int J Clin Pract 2007 61 171 180 17156104
- Hermansen K Kipnes M Luo E Fanurik D Khatami H Stein P Efficacy and safety of the dipeptidyl peptidase-4 inhibitor, sitagliptin, in patients with type 2 diabetes mellitus inadequately controlled on glimepiride alone or on glimepiride and metformin Diabet Obes Metab 2007 9 733 745
- Rosenstock J Brazg RG Andryuk PJ Lu K Stein P Efficacy and safety of the dipeptidyl peptidase-4 inhibitor sitagliptin added to ongoing pioglitazone therapy in patients with type 2 diabetes: a 24-week, multicenter, randomized, double-blind, placebo- controlled, parallel-group study Clinical Ther 2006 28 1556 1568 17157112
- Alba M Sheng D Guan Y Sitagliptin 100 mg daily effect on DPP-4 inhibition and compound-specific glycemic improvement Curr Med Res Opin 2009 25 2507 2514 19691426
- Aaboe K Vilsbøll T Knop FK Twelve weeks treatment with the DPP-4 inhibitor, sitagliptin, improves the insulin secreting capacity of the β-cells in subjects with type 2 diabetes mellitus: a randomized trial Diabetes 2009 Suppl 1 A163
- Hanefeld M Herman GA Wu M Mickel C Sanchez M Stein PP Once-daily sitagliptin, a dipeptidyl peptidase-4 inhibitor, for the treatment of patients with type 2 diabetes Curr Med Res Opin 2007 23 1329 39 17559733
- Qi DS Teng R Jiang M Two-year treatment with sitagliptin and initial combination therapy of sitagliptin and metformin provides substantial and durable glycaemic control in patients with type 2 diabetes Diabetologia 2008 51 Suppl 1 S36
- Chan JCN Scott R Arjona Ferreira JC Safety and efficacy of sitagliptin in patients with type 2 diabetes and chronic renal insufficiency Diabetes Obes Metab 2008 10 545 555 18518892
- Barzilai N Mahoney EM Guo H Sitagliptin is well tolerated and leads to rapid improvement in blood glucose the first days of monotherapy in patients aged 65 years and older with TDM Diabetes 2009 Suppl 1 A158
- Nauck MA Meininger G Sheng D Terranella L Stein PP Efficacy and safety of the dipeptidyl peptidase-4 inhibitor, sitagliptin, compared with the sulfonylurea, glipizide, in patients with type 2 diabetes inadequately controlled on metformin alone: a randomized, double-blind, non-inferiority trial Diabet Obes Metab 2007 9 194 205
- Scott R Loeys T Davies MJ Engel SS Efficacy and safety of sitagliptin when added to ongoing metformin therapy in patients with type 2 diabetes Diabetes Obes Metab 2008 10 959 969 18201203
- Vilsbøll T Rosenstock JM Yki-Järvinen H Efficacy and safety of sitagliptin when added to insulin therapy in patients with type 2 diabetes Diabetes Obes Metab 2010 12 167 177 20092585
- Arjona Ferreira JC Dobs A Goldstein BJ Triple combination therapy with sitagliptin, metformin and rosiglitazone improves glycaemic control in patients with type 2 diabetes Diabetologia 2008 51 Suppl 1 S365
- Rosenstock J Baron MA Dejager S Mills D Schweizer A Comparison of vildagliptin and rosglitazone monotherapy in patients with type 2 diabetes: a 24-week double-blind, randomized trial Diabetes Care 2007 30 217 223 17259484
- Jadzinsky M Pfützner A Paz-Pacheco E Xu Z Allen E Chen R Saxagliptin given in combination with metformin as initial therapy improves glycaemic control in patients with type 2 diabetes comperaed with either monotherapy: a randomized controlled trial Diabetes Obes Metab 2009 11 611 622 19515181
- DeFronzo RA Fleck PR Wilson CA Mekki Q Efficacy and safety of the dipeptidyl peptidase-4 inhibitor alogliptin in patients with type 2 diabetes and inadequate glycemic control: a randomized, double-blind, placebo-controlled study Diabetes Care 2008 31 2315 2317 18809631
- Bolli G Dotta F Rochotte E Cohen SE Efficacy and tolerability of vildagliptin vs pioglitazone when added to metformin: a 24-week randomized, double-blind study Diabet Obes Metab 2008 10 82 90
- DeFronzo RA Hissa MN Garber AJ The efficacy and safety of saxagliptin when added to metformin therapy in patients with inadequately controlled type 2 diabetes with metformin alone Diabetes Care 2009 32 1649 1655 19478198
- Nauck MA Ellis GC Fleck PR Wilson CA Mekki Q Efficacy and safety of adding the dipeptidyl peptidase-4 inhibitor alogliptin to metformin therapy in patients with type 2 diabetes inadequately controlled with metformin monotherapy: a multicentre, randomized, double-blind, placebo-controlled study Int J Clin Pract 2009 63 46 55 19125992
- Garber AJ Schweizer A Baron MA Rochotte E Dejager S Vildagliptin in combination with pioglitazone improves glucaemic control in patients with type 2 diabetes failing thiazolidinedione monotherapy: a randomized, placebo-controlled study Diabet Obes Metab 2007 9 166 174
- Hollander P Li J Allen E Chen R Saxagliptin added to a thiazolidinedione improves glycemic control in patients with type 2 diabetes and inadequate control on thiazolidinedione alone J Clin Endocrinol Metab 2009 94 4810 4819 19864452
- Pratley RE Reusch JE Fleck PR Wilson CA Mekki Q Efficacy and safety of the dipeptidyl peptidase-4 inhibitor alogliptin added to pioglitazone in patients with type 2 diabetes: a randomized, double-blond, placebo-controlled study Curr Med Res Opin 2009 25 2361 2371 19650752
- Garber AJ Foley JE Banerhi MA Effects of vildagliptin on glucose control in patients with type 2 diabetes inadequately controlled with a sulphonylurea Diabet Obes Metab 2008 10 1047 1056
- Chacra AR Tan GH Apanovitch A Ravichandran S List J Chane R Saxagliptin added to submaximal dose of sulphonylurea improves glucaemic control compared with uptitration of sulphonylurea in patients with type 2 diabetes: a randomized controlled trial Int J Clin Pract 2009 63 1395 1406 19614786
- Pratley RE Kipnes MS Fleck PR Wilson C Mekki Q Efficacy and safety of the dipeptidyl peptidase-4 inhibitor alogliptin in patients with type 2 diabetes inadequately controlled by glyburide monotherapy Diabet Obes Metab 2009 11 167 176
- Williams-Herman D Round E Swern A Safety and tolerability of sitagliptin in patients with type 12 diabetes: a pooled analysis BMC Endocr Disord 2008 8 14 18954434
- Dore DD Seeger JD Arnold Chan K Use of claims-based active drug safety surveillance system to assess the risk of acute pancteatitis with exenatide or sitagliptin compared to metformin or glyburide Curr Med Res Opin 2009 25 1019 1027 19278373
- de Heer J Holst JJ Sulphonylurea compounds uncouple the glucose dependence of the insulinotropic effect of glucagon-like peptide 1 Diabetes 2007 56 438 443 17259389
- Ahrén B Schweizer A Dejager S Vildagliptin enhances islet responsiveness to both hyper- and hypoglycemia in patients with type 2 diabetes J Clin Endocrinol Metab 2009 94 11236 1243
- Ferrannini E Fonseca V Zinman B Fifty-two-week efficacy and safety of vildagliptin vs glimepiride in patients with type 2 diabetes mellitus inadequately controlled on metformin monotherapy Diabetes Obes Metabol 2009 11 157 166
- Rodbard HW Jellinger PS Davidson JA Statement by an American association of clinical endocrinologists/American college of endocrinology consensus panel on type 2 diabetes mellitus: an algorithm for glycemic control Endocr Pract 2009 15 541 559
- Ahrén B Islet G protein-coupled receptors as potential targets for treatment of type 2 diabetes Nat Rev Drug Discov 2009 8 369 385 19365392
- Schwarz B Gouveia M Chen J Cost-effectiveness of sitagliptinbased treatment regimens in European patients with type 2 diabetes and haemoglobin A1c above target on metformin monotherapy Diabetes Obese Metab 2008 10 Suppl 1 43 55
- www.clinicaltrials.gov (NCT00790205) Accessed February 18, 2010
- Ahrén B Foley JE The islet enhancer vildagliptin: mechanisms of improved glucose metabolism Int J Clin Pract 2008 62 Suppl 159 8 14 18173812
- Carr RD Larsen MO Sörhede Winzell M Incretin and islet hormonal responses to fat and protein ingestion in healthy men Am J Physiol 2008 295 E779 E784