Abstract
Hemivertebra is a rare congenital spinal malformation, where only one side of the vertebral body develops, resulting in deformation of the spine, such as scoliosis, lordosis, or kyphosis. We present the ultrasonographic features of a fetus with hemivertebra at 20 weeks’ gestation confirmed by post mortem radiography and pathological examination. The prenatal literature on this disorder is also reviewed. Useful background information is provided for both clinicians and other health professionals who are not familiar with this condition.
Introduction
Hemivertebra is a rare congenital malformation of the spine, where only one side of the vertebral body develops, resulting in a laterally-based wedge vertebra with half a vertebral body, a single pedicle, and hemilamina.Citation1 Other terms used for this lesion are congenital scoliosis, unilateral aplasia of the vertebral body, and complete unilateral failure of formation of the vertebral body.Citation2 Hemivertebra can be isolated or associated with defects of other organ systems. We describe our experience of a case of congenital scoliosis due to hemivertebra detected prenatally at 20 weeks’ gestation, including the ultrasonographic findings that led to the diagnosis and the post mortem radiological characteristics.
Case report
The patient was a 26-year-old woman, gravida 1 para 0, with an unremarkable medical history. The triple test at 16 weeks’ gestation was negative, ie, alpha-fetoprotein 42 ng/mL (multiples of the mean [MoM] = 0.992), estriol 3.8 nmol/L (MoM = 1.834), free beta- human chorionic gonadotropin 28 ng/mL (MoM = 2.806). No malformations were detected during ultrasound scanning at the sixteenth week of gestation. At the routine ultrasonographic anatomy scan of the fetus at 20 weeks’ gestation, the biparietal diameter was 46 mm, the abdominal circumference 145 mm, the fetal femur length 32 mm, and estimated fetal weight 348 g. Amniotic fluid was within normal limits. However, a distortion at the lumbar region of the spine was demonstrated in the longitudinal plane. A small triangular bony structure was wedged against the normal vertebral bodies ( and ). The overlying skin appeared intact and there were no intercranial findings suggestive of an open neural tube defect. No other abnormalities were detected. The initial diagnosis was single hemivertebra, and the parents opted for termination of pregnancy. Labour was induced using misoprostol. A 500 g stillborn female neonate was delivered with obvious deformation of the spine (), and the ultrasonographic findings were confirmed with a simple X-ray of the stillborn fetus ( and ) and with pathologic examination. No other skeletal anomalies of the spine, ribs, and limbs, or cardiac, renal, and gastrointestinal anomalies were found. The fetal karyotype was 46, XX.
Figure 1 Longitudinal ultrasonographic scans of the spine of a second trimester fetus with hemivertebra.
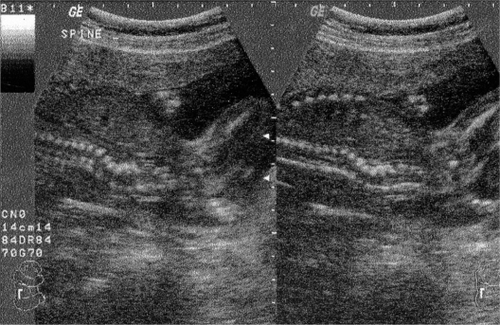
Figure 2 Longitudinal ultrasonographic scan of the spine of a second trimester fetus with hemivertebra.
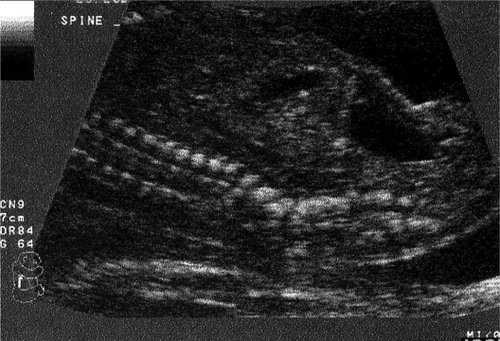
Figure 3 The stillborn female neonate presents obvious deformation of the spine (arrow).

Figure 4 Post mortem lateral radiograph of the spine shows lumbar hemivertebra.
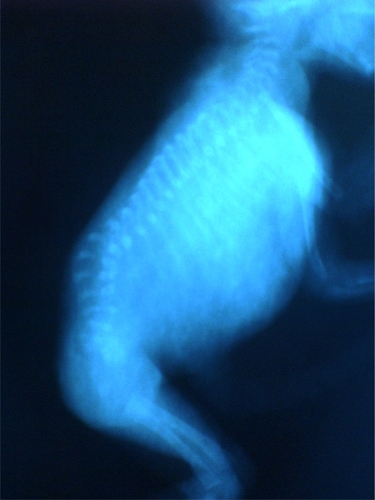
Figure 5 Post mortem plain radiograph of the spine shows lumbar hemivertebra.

Discussion
The incidence of hemivertebra is estimated at 0.5–1.0 per 1000 births, with a male to female ratio of 0.31 for multiple vertebral anomalies and 0.68 for solitary vertebral anomalies.Citation1,Citation3 In our case, the affected fetus was female, and this is in agreement with the described higher incidence for females compared with males. The English literature contains only few cases of vertebral malformation which were diagnosed prenatally.Citation2,Citation4–Citation10
Gastrulation occuring in the embryonic period converts the bilaminar embryonic disc to a trilaminar structure containing ecto-, endo-, and mesoderm. Spinal development involving the formation of mesodermal-derived somites culminates in the formation of primitive vertebrae.Citation11 The vertebrae develop during the sixth week of gestation, when two lateral chondrification centers arise in the developing vertebral bodies. These chondrification centers then fuse by seven to eight weeks’ gestational age to form the primary ossification center of the vertebral body, transiently separated into anterior and posterior aspects by the notochord remnant. Lateral hemivertebrae result from lack of development of one of the paired chondral centers. Less commonly, posterior hemivertebrae result from failed anterior ossification.Citation10,Citation12,Citation13 The defective vertebra acts as a triangular wedge-shaped ossified structure within the vertebral column, causing contralateral spine deviation at the level of the abnormal vertebra.Citation2,Citation8,Citation10,Citation14 There are four different types of hemivertebrae characterized by the presence or absence of a normal disk space adjacent above and below the affected segment, ie, fully segmented (the most common), semisegmented, nonsegmented, and incarcerated (the least common).Citation1
The cause of hemivertebra is unknown. One hypothesis has suggested that hemivertebra may result from abnormal distribution of the intersegmental arteries of the vertebral column.Citation15,Citation16 The distribution pattern of the anomaly does not implicate a specific environmental or genetic factor. Hemivertebrae may be isolated or may occur in multiple areas within the spine and is frequently associated with other congenital anomalies.Citation9,Citation17,Citation18 Hemivertebra is commonly associated with other skeletal anomalies of the spine, ribs, and limbs.Citation9,Citation10,Citation17,Citation18 Combination of diastematomyelia and hemivertebra has also been observed.Citation19,Citation20 Cardiac and genitourinary tract anomalies are the most common extramusculoskeletal anomalies seen with hemivertebra. Anomalies of the central nervous system and gastrointestinal tract have also been reported. Citation9,Citation10,Citation17,Citation18 Approximately one-sixth of patients with vertebral body anomalies have associated anomalies unrelated to the axial skeleton and spinal cord.Citation1,Citation3 Hemivertebra may be part of syndromes including Jarcho-Levin syndrome, Klippel-Fiel syndrome, VATER syndrome (vertebral anomalies, imperforate anus, tracheoesophageal fistula, and renal anomalies), VACTERL syndrome (VATER with cardiac and limb anomalies), OEIS (omphalocele, bladder extrophy, imperforate anus, and spine anomalies), the Potter sequence, and open spina bifida.Citation13 The incidence of karyotypic abnormalities in fetuses with isolated vertebral anomalies is thought to be small.Citation2,Citation10
The gestational age at diagnosis of hemivertebra is usually 20–28 weeks.Citation1 However, because the ossification centers of the vertebrae can be initially visualized by ultrasound examination after 12 weeks’ gestation, the defect of ossification can be visible on early scans.Citation1 The diagnosis of fetal hemivertebra on prenatal ultrasound requires meticulous examinations. The sonographic findings associated with fetal hemivertebra include a distortion in the shape of the spine that can be assessed by both sagittal and coronal scans. The deformity manifests as a triangular bony structure, smaller than a vertebra, that acts as a wedge against the normal vertebral bodies ().Citation8,Citation10 A careful assessment for associated cardiac, renal, and gastrointestinal anomalies needs to be performed. Hemivertebra may have a similar ultrasonic appearance to other vertebral abnormalities (wedge vertebra, butterfly vertebra, bloc vertebra, bar vertebra, or any combination of these) that cause congenital scoliosis, open neural tube defects, and diastematomyelia.Citation2,Citation8,Citation21 Diastematomyelia is a rare form of spinal dysraphism, characterized by a sagittal cleft in the spinal cord, conus medullaris, and/or filum terminale with splaying of the posterior vertebral elements.Citation22–Citation24 Diastematomyelia is subdivided into Type I and Type II. Type I consists of two hemicords, contained within two separate dural sheaths, and separated by a rigid, osseocartilaginous median septum.Citation22–Citation24 Type II is characterized by two hemicords housed in a single dural sheath and separated by a nonrigid, fibrous median septum.Citation22–Citation24 Diastematomyelia may be isolated, or it may be associated with other spinal anomalies such as spina bifida, kyphoscoliosis, butterfly vertebra, or hemivertebra.Citation22 Diastematomyelia usually occurs as a nonsyndromal sporadic disorder. However, a few familial cases have been reported and Bacli et al suggested that X-linked dominant inheritance, with limitations to females because of lethality in homozygous males, could not be excluded.Citation25
Ultrasonographic features of diastematomyelia include widening of the spinal canal in the coronal section, with extraechogenic foci located in the midline between localized widenings of the posterior ossification centers of the vertebral column.Citation24 Echogenic foci in the posterior aspect of the vertebral column in axial section are highly specific for diastematomyelia.Citation22
Obstetric counseling and management for fetal hemivertebra depends on the time of diagnosis, the presence of isolated hemivertebra or of multiple vertebral abnormalities, and the identification of other associated malformations. The option of pregnancy termination should be offered when involvement of several vertebrae or of additional organ systems is observed. If only one vertebra is affected and no other fetal malformations are detected, conservative management of pregnancy could be offered.Citation10 In our case, pregnancy termination was performed at the parents’ request. The prognosis of hemivertebra is partially determined by the site of the affected vertebra, the number of affected vertebrae, and the associated anomalies.Citation1 The prognosis of isolated hemivertebra is good. Left untreated, 25% of patients with congenital scoliosis show no progression, 50% progress slowly, and 25% progress rapidly during growth.Citation2,Citation26 When the prenatal diagnosis of hemivertebrae is made, a meticulous search for associated anomalies should be performed. Chromosomal analysis can be offered, especially in the presence of associated anomalies because an increased risk of aneuploidy may exist. Alpha-fetoprotein concentration in amniotic fluid can be assessed if there is a question of an open neural tube defect and the fetus is of appropriate gestational age. Serial ultrasonic evaluation is recommended to follow fetal growth and evaluate for signs of an open neural tube defect that may not be present at an initial early ultrasound.Citation2,Citation8 Fetuses with hemivertebra have high rates of cesarean delivery and growth restriction. Neonates with nonisolated hemivertebrae are more often delivered before term and have higher mortality rates.Citation13 If there are no other complicating factors, standard management of labor and delivery is recommended. A careful neonatal assessment for associated cardiac and genitourinary anomalies needs to be performed.Citation2,Citation8 The surgical treatment of congenital scoliosis is aimed at producing a straight and balanced spine at skeletal maturity. There are three key factors in achieving an optimal spine at maturity, ie, early diagnosis, anticipation of scoliosis, and prevention of deterioration.Citation1 Risk of neural tube defects in siblings is increased.Citation8 Therefore, it would be reasonable to offer genetic counseling and prenatal diagnosis for neural tube defects to those patients with a previous child with vertebral anomalies.Citation2
Conclusion
Prenatal diagnosis of hemivertebra is feasible. The characteristic ultrasonographic findings in the fetus allow the early detection of hemivertebra, providing parents with valuable information in order to make their decision regarding the fate of the pregnancy. When the parents opt to continue with the pregnancy, early postnatal evaluation and frequent follow-up will optimize treatment and reduce the risk of serious scoliosis and its complications.
Disclosure
The authors report no conflict of interest in this research.
References
- WeiszBAchironRSchindlerAEisenbergVHLipitzSZalelYPrenatal sonographic diagnosis of hemivertebraJ Ultrasound Med20042385385715244311
- GauthierDWMeyerWJ Hemivertebra. The-Fetus.net Central nervous system. 199316 Available from: http://www.thefetus.net Accessed on May 14, 2010.
- Wynne-DaviesRCongenital vertebral anomalies: Aetiology and relationship to spina bifida cysticaJ Med Genet1975122802881100836
- ZelopCMPretoriusDHBenacerrafBRFetal hemivertebrae: Associated anomalies, significance, and outcomeObstet Gynecol1993814124168437797
- BenacerrafBRGreeneMFBarssVAPrenatal sonographic diagnosis of congenital hemivertebraJ Ultrasound Med198652572593517372
- BroekmanBADorrJPCongenital kyphosis due to absence of two lumbar vertebral bodiesJ Clin Ultrasound1991193033051651348
- HenryRJNortonSPrenatal ultrasound diagnosis of fetal scoliosis with termination of the pregnancy: Case reportPrenat Diagn198776636663321026
- PiluJL Hemivertebra. Thefetus.net 199913 Available at: (http://www.thefetus.net). Accessed on May 14, 2010.
- McMasterMJDavidCVHemivertebra as a cause of scoliosisJ Bone Joint Surg198668588595
- GoldsteinIMakhoulIRWeissmaanADruganAHemivertebra: Prenatal diagnosis, incidence and characteristicsFetal Diagn Ther20052012112615692206
- LeungYLBuxtonNCombined diastematomyelia and hemivertebra. A review of the management at a single centreJ Bone Joint Surg200587B13801384
- MooreKLPeraudTVNThe Developing Human5th edPhiladelphia, PAW.B. Saunders1993
- WaxJRWatsonWJMillerRCPrenatal sonographic diagnosis of hemivertebrae – associations and outcomesJ Ultrasound Med2008271023102718577665
- HeftiFCongenital anomalies of the spineOrthopade200231344311963467
- TanakaTUhthoffHKThe pathogenesis of congenital vertebral malformations. A study based on observations made in 11 human embryos and fetusesActa Orthop Scand1981524134256797230
- ForresterMBMerzRDDescriptive epidemiology of hemivertebrae, Hawaii, 1986–2002Congenit Anom20064617246176
- ConnorJMConnerANConnorRACTolmieJLYeungBGoudieDGenetic aspects of early childhood scoliosisAm J Med Genet1987274194243300334
- DavidCVHemivertebra as a cause of scoliosisJ Bone Joint Surg198668588595
- LeugYLBuxtonNCombined diastematomyelia and hemivertebra. A review of the management at a single centreJ Bone Joint Surg200587-B13801384
- DabraAGuptaRSidhuRKochharSKaurLSinghJSonographic diagnosis of diastematomyelia in utero: A case report and literature reviewAustral Radiol200145222224
- ChenMChanBLamTPShekTLeeCPTangMHSonographic features of hemivertebra at 13 weeks’ gestationJ Obstet Gynecol Res200733747717212670
- HasRYukselABuyukkurtSKaleliogluITatliBPrenatal diagnosis of diastematomyelia: Presentation of eight cases and review of the literatureUltrasound Obstet Gynecol20073084584917726726
- KaraşahimKEGezginçKAlanbayIUlubayMBaşerIUltrasonographic diagnosis of diastematomyelia during the 14th week of gestationTaiwan J Obstet Gynecol20094816316619574180
- AllenLMSilvermanRKPrenatal ultrasound evaluation of fetal diastematomyelia: Two cases of type I split cord malformationUltrasound Obstet Gynecol200015788210776019
- BalciSCaglarKEryilmazMDiastematomyelia in two sistersAm J Med Genet19998618018210449657
- WinterRBCongenital scoliosisOrthop Clin North Am1988193954083357687