Abstract
Synchronous bilateral male breast cancer (MBC) is rare and only a few cases have been reported in the literature. The majority of MBC patients have no definable risk factors. We describe a case with Klinefelter’s syndrome, prior thymic irradiation, testicular surgery, and first degree family history in a 61-year-old male.
Introduction
Male breast cancer (MBC) is uncommon, accounting for <1% of all cases.Citation1 Bilateral male breast cancer is very rare and in two large series was reported in only 0.2%–2.7% of cases.Citation2,Citation3 It is recognized that hormonal, genetic, and environmental factors play a part in the pathogenesis of female breast cancer and also play a significant in role in MBC, particularly in cases with bilateral disease. Individuals with Klinefelter’s syndrome (KS), have at least one X chromosome added to the normal XY karyotype (usually 47XXY).Citation4 This is associated with testicular dysgenesis, gynecomastia, low testosterone levels, and increased gonadotropins. The prevalence of KS is 1 in 1000 newborn boys. There is a 20- to 50-fold increased risk of breast cancer in these individuals compared with 46XY men,Citation5 together with a highly increased standard mortality ratio.Citation6 We report bilateral breast cancer in such a case.
Case report
A 61-year-old male presented to the breast clinic with a two-week history of scaly, encrusted eczematous changes of the left nipple associated with an underlying lump. The left nipple had been inverted for two years. He was married but childless and had been diagnosed with KS following investigation for infertility many years previously. At the age of three years he had undergone radiotherapy for an enlarged thymus, right orchidectomy for an undescended testis at the age of 27 years and a left-sided inguinal hernia repair at the age of 39 years. Other significant past medical history included hypothyroidism, managed with thyroxine, and osteoarthritis. The patient’s mother was reported to have breast cancer diagnosed in her forties but was alive and well at the age of 88 years.
On examination, the patient had bilateral gynecomastia with deformity of the left breast, a scaly left nipple and a 3 × 3.3 cm mass deep in it. The mass was not deeply fixed and there was no associated axillary lymphadenopathy. The left testis was atrophic. A clinical diagnosis of operable left breast cancer was made and core biopsy of the left breast mass confirmed an invasive ductal carcinoma.
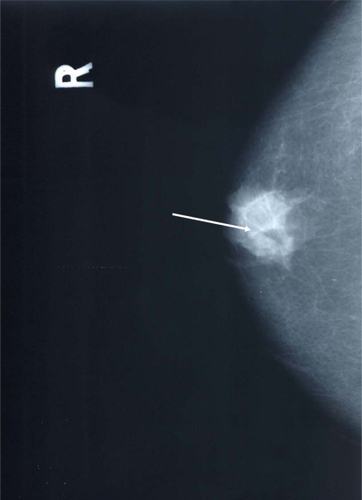
Bilateral mammography (see and ) showed a cluster of unusual macro and microcalcification supero-laterally, close to the posterior border of the right nipple, which had an indeterminate appearance (M3). Subsequent ultrasonography of the right breast showed echogenic changes consistent with calcification but no other specific features (U3). Fine needle aspiration cytology of that area was nondiagnostic. Staging showed no evidence of metastatic disease. The patient proceeded to have a left modified radical mastectomy with a simultaneous right simple mastectomy following review of the case, pathology, and images at a multidisciplinary meeting.
Figure 1 MLO view (arrow indicates microcalcification).

Figure 2 CC view (arrow indicates microcalcification).
Histology of the left breast confirmed a completely excised 18 mm Grade I invasive ductal carcinoma with no evidence of vascular invasion. There was direct extension into the overlying epidermis of the nipple with mimicry of Paget’s disease. The tumor was estrogen and progesterone receptor positive and there was weak expression of HER-2 receptors. The left auxiliary lymph nodes showed no evidence of metastases (0/7 nodes). Histology of the right breast revealed areas of intermediate-grade ductal carcinoma in-situ (DCIS), the largest focus being 4 mm in maximum diameter.
The patient received adjuvant tamoxifen. Although he developed mild lymphedema of the left arm he was able to resume a normal lifestyle. After five years of follow-up he remains well with no evidence of locoregional recurrence.
Discussion
There are a multitude of recognized risk factors for male breast cancer, such as advancing age, KS, testicular disease, childlessness, cirrhosis of the liver, exogenous estrogen administration in transsexuals and patients with prostate cancer, obesity, previous radiation exposure, and a family history of male or female cancer especially those associated with BRCA2 mutation.Citation7–Citation9 shows the major risk factors together with the associated relative risk, if known.
Table 1 Risk factors for male breast cancer
It is probably the relative hyperestrogenization in KS that is responsible for the 50-fold increased risk of developing breast cancer in this syndrome relative to normal males.Citation5 While it is most likely that Klinefelter’s was responsible for the cancers in our patient, he also had several other known risk factors; orchidectomy, inguinal hernia repair, radiation exposure, and a family history of maternal premenopausal breast cancer. The latter two factors are independent of Klinefelter’s. Hildreth and colleagues studied the incidence of breast cancer prospectively in a cohort of 1,201 women who received X-ray treatment in infancy for an enlarged thymus gland and in their 2,469 nonirradiated sisters. They concluded that exposure of the female breast to ionizing radiation in infancy increases the risk of breast cancer later in life with an adjusted rate ratio of 3.6.Citation10
The clinical presentation of the invasive cancer is typical for male breast cancer: a centrally located (70%–90%), painless mass (75%–90%) in a 61-year-old male (mean age of presentation, 60–65 years) that on histology was confirmed as an infiltrating ductal carcinoma (70%–90% of cases).Citation7 Breast cancer in females occurs more frequently on the left side (1:1.2) and the same phenomenon has been observed in MBC with the presenting cancer being left-sided In our case.
DCIS in men is a rare disease representing only 5% of MBC which also occurs more commonly on the left side (71%).Citation7 Whilst bilateral male breast cancers have been reported before, only a few cases occurring in men with Klinefelter’s syndrome.Citation11–Citation13 To the best of our knowledge this is the first case of a synchronous infiltrating ductal carcinoma of the breast with contralateral DCIS in a KS patient reported in the literature. This case highlights the importance of investing the apparently normal contralateral breast in MBC cases.
Disclosures
The authors report no conflicts of interest in this work.
References
- SascoAJLowenfelsABPasker-de JongPReview article: epidemiology of male breast cancer. A meta-analysis of published case-control studies and discussion of selected aetiological factorsInt J Cancer1993535385498436428
- GiordanoSHCohenDSBuzdarAUPerkinsGHortobagyiGNBreast carcinoma in men. A population-based studyCancer2004101515715221988
- CutuliBFLacrozeMDilhuydyJMBreast cancer in men: incidence and types of associated previous synchronous and metachronous cancersBull Cancer1992796896961467595
- KlinefelterHGReifenteinECJrAlbrightFSyndrome characterized by gynaecomastia, aspermatogenesis without a-Leydigism and increased secretion of follicle-stimulation hormoneJ Clin Endocrinol Metab19422615627
- HultbornRHansonCKopfIVerbienéIWarnhammarEWeimarckAPrevalence of Klinefelter’s syndrome in male breast cancer patientsAnticancer Res198717429342979494523
- SwerdlowAJSchoemakerMJHigginsCDWrightAFJacobsPAUK Clinical Cytogenetics GroupCancer incidence and mortality in men with Klinefelter syndrome: a cohort studyJ Natl Cancer Inst2005971204121016106025
- FentimanISFourquetAHortobagyiGMale breast cancerLancet200636759560116488803
- WeissJRMoysichKBSwedeHEpidemiology of male breast cancerCancer Epidemiol Biomarkers Prev200514202615668471
- MabuchiKBrossDSKesslerIIRisk factors for male breast cancerJ Natl Cancer Inst1985743713753856050
- HildrethNGShoreREDvoretskyPMThe risk of breast cancer after irradiation of the thymus in infancyN Engl J Med1989321128112842797100
- RobsonMCSantiagoQHuangTWBilateral carcinoma of the breast in a patient with Klinefelter’s syndromeJ Clin Endocrinol Metab1968288979024297793
- ColeyGMOtisRDClarkWEMultiple primary tumors including bilateral breast cancers in a man with Klinefelter’s syndromeCancer197127147614814325988
- SanchezAGVillanuevaAGRedondoCLobular carcinoma of the breast in a patient with Klinefelter’s syndrome. A case with bilateral, synchronous, histologically different breast tumorsCancer198657118111833002597