Abstract
Objective:
To determine the use of spirometry in family practice, internal medicine, and pediatric outpatient settings.
Methods:
Data were collected from 45 outpatient offices in the central Pennsylvania area via phone survey that asked a set of four questions: 1) Do you have spirometry in your office? 2) Do you use spirometry for asthma patients? 3) In what situation do you use spirometry for? 4) Do you use spirometry more for chronic obstructive pulmonary disease (COPD) or asthma?
Results:
It was found that pediatricians used spirometry 66% of the time, family practitioners 47% of the time, and internal medicine practitioners 60% of the time. Of those who did not use spirometry, 94% stated that they refer to a hospital if they required spirometry and 6% referred to subspecialists if the patient required spirometry. 10% of pediatricians performed the test on each asthma visit, otherwise the others used it only for exacerbations or as a baseline. No internists used spirometry regularly for asthma patients, and 22% used it more for COPD. In family practice only 14% used spirometry routinely at each visit for asthma patients.
Conclusions:
Pediatricians used spirometry more often in the outpatient setting than other specialists, followed closely by internal medicine physicians. Family practice physicians were the least likely to use spirometry. Multiple barriers seemed to prevent routine use of spirometry, but no one barrier accounted for the majority.
Keywords:
Introduction
Spirometry has been an important part in asthma diagnosis, assessing risk of future adverse events, and guiding treatment because it is one of the few objective parameters used in asthma that can change the assessment and treatment of asthma.Citation1
“The expert panel recommends the following frequencies for spirometry measurements: at the time of initial assessment; after treatment is initiated and symptoms and PEF have stabilized, to document attainment of (near) “normal” airway function; during a period of progressive or prolonged loss of asthma control; and at least every 1–2 years to assess the maintenance of airway function. Spirometry may be indicated more often than every 1–2 years, depending on the clinical severity and response to management. These spirometry measures should be followed over the patient’s lifetime to detect potential for decline and rate of decline of pulmonary function over time.”Citation1
The use of spirometry could help detect cases at an early stage when intervention may prevent further progression of the disease.Citation2 Spirometry is also important because studies have shown poor correlation between subjective symptoms and the degree of obstruction on spirometry, and in one study, up to 27% of physicians using symptoms alone for diagnosis underestimated asthma severity.Citation3
A national survey eight years ago found that only a fifth of primary care providers used spirometry on a regular basis.Citation4 In one study, asthma specialists were more likely to have an office spirometer and use it than were primary care physicians.Citation5 In the same study, primary care physicians were more likely to use a spirometer if they agreed the data was necessary for accurate diagnosis and care, and if they believed they could be appropriately trained to perform and interpret the test correctly.Citation5 This study was conducted to assess the use of spirometry care in primary care, based on speciality, in order to help direct where education on this technique should be directed and to see if there is greater utilization of spirometry compared to almost a decade ago.
Methods
Sixty-nine primary care offices in central Pennsylvania were contacted by phone in 2008 to determine if they utilized spirometry and to assess barriers for the use of spirometry. Spirometry was differentiated from the use of peak expiratory flow meters. The survey was conducted by questioning the office manager of the practice. Forty-five offices answered the survey, 15 in each specialty. They were asked a series of questions as follows: Do you use spirometry in your office? If you do not use spirometry in the office do you refer them for spirometry? If you use a spirometer in your office do you use it more often to assess asthma or chronic obstructive pulmonary disease (COPD)? Do you use spirometry to establish a baseline, for exacerbations, both or at every visit? Questions regarding COPD were omitted in pediatrician offices.
Results
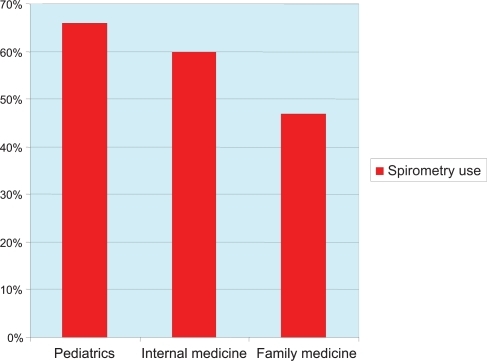
Pediatricians used spirometry 10% of the time on patients with asthma at every visit, 30% of the time to achieve a baseline, 10% of the time during an exacerbation only, 40% of the time for both baseline and exacerbation, and 10% of the time for reasons other than asthma, which they did not specify. None of the internal medicine physicians used spirometry at every asthma visit, but did use it 33% of the time to establish a baseline, 44% of the time during an exacerbation, 11% did not use it for asthma at all, and 11% owned a spirometer, but never used it. 22% of internists used spirometry more for COPD than asthma. Family medicine physicians used spirometry 14% of the time at every visit, 29% of the time for baseline, 29% of the time for exacerbations only, and 29% for both exacerbations and baselines. No family medicine physician used it for a reason other than asthma (). Pediatricians use spirometry the most at 66%, followed by internal medicine at 60%, and family medicine last at 47% (). Of those who did not use spirometry, 94% of these physicians referred to a hospital if they needed one, and 6% referred to a subspecialist.
Figure 1 Reasons for the use of spirometry in primary care based on specialty.
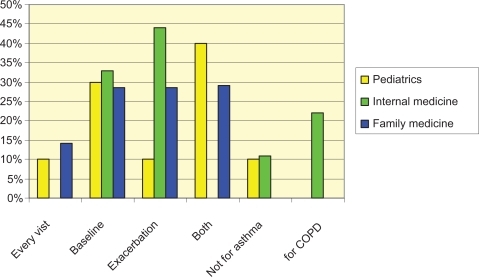
Figure 2 Percent usage of spirometry in the subspecialties of primary care.
Discussion
Primary care physicians provide care to about 66% of asthmatics in the US, but seem to underutilize spirometry as a tool to diagnose and serially follow the course of asthma. Despite recommendations about optimal care for patients with asthma by the National Asthma Education and Prevention Program, spirometry is still not being used to assess the majority of patients with asthma. Our data suggest that pediatricians utilize spirometry to the greatest extent, and this is likely secondary to the past efforts to teach pediatricians about spirometry, how to utilize spirometry to optimize care of patients with asthma and how to interpret the results.Citation4,Citation6–Citation12 While the usage of spirometry still seems low, our study shows increased frequency of its use over what has been demonstrated previously. This suggests that the NHLBI Guidelines for Management of Asthma have influenced care for patients with asthma. The increase utilization of inhaled corticosteroids and decreasing mortality associated with asthma are other factors that seem to suggest that guidelines do have an impact on asthma care.
Studies in the past have shown that interpretation of spirometry by family physicians following training was almost equivalent to that of pulmonologists.Citation6 Appropriate interpretation also impacted the change in therapy in as much as 30% of patients. When the treatment was changed the provider increased therapy approximately 75% of the time.Citation6 This data suggests that that the use of spirometry may improve asthma outcomes, and that utilization of this technique should increase. This is especially true for family medicine physicians who seem to be utilizing it the least.
This study’s main limitation is limited sample size. We also failed to elicit the barriers that prevented the use of in office spirometry. In addition, we did not query as to what prompted an outside referral for spirometry. We suspect that one barrier to its use is that there is a concern about proper interpretation. Another potential barrier is the concern that adequate technique will limit the benefit of spirometry. This latter concern is somewhat supported by prior literature that suggests spirometry results are more accurate when the technician performing them has more experience. A study in Spain showed that a mere 48% of spirometry tests were considered acceptable.Citation13 Nonetheless, newer spirometers, with user friendly software and patient friendly soft ware, improve the results even when the spirometer is not being used multiple times a day.
It appears that education on spirometry would enhance its utilization in primary care if it focused on how to purchase and maintain a spirometer, perform spirometry, interpret the results, correctly invoice for the services, and how the results can be used to improve asthma management. There also appears to be an opportunity for allergists to perform spirometry in their offices as a service for primary care physicians. This may decrease cost and improve availability both which may increase utilization of the procedure by primary care physicians.
Disclosures
The authors report no conflicts of interest in this work.
References
- National Asthma Education and Prevention ProgramExpert Panel Report 3 (EPR-3): Guidelines for the Diagnosis and Management of Asthma-Summary Report 2007J Allergy Clin Immunol20071205 SupplS94S13817983880
- CelliBRThe importance of spirometry in COPD and asthmaChest200011715S19S10673468
- YawnBPEnrightPLLemanskeRFJrSpirometry can be done in family physicians’ offices and alters clinical decisions in management of asthma and COPDChest200713241162116817550939
- FinkelsteinJALozanoPShulruffRSelf-reported physician practices for children with asthma: are national guidelines followed?Pediatrics200010688689611044140
- O’DowdLCFifeDTenhaveTPanettieriRAJrAttitudes of physicians toward objective measures of airway function in asthmaAm J Med2003114539139612714129
- HoltEWTanJHosgoodHDThe impact of spirometry on pediatric asthma diagnosis and treatmentJ Asthma200643748949316939987
- CabanaMSlishKKNanBLeoHBrattonSLDombkowskiKJOutcomes associated with spirometry for pediatric asthma in a managed care organizationPediatrics20061181e151e15616769797
- NairSJDaigleKLDeCuirPLapinCDSchrammCMThe influence of pulmonary function testing on the management of asthma in childrenPediatrics20051476797801
- ZanconatoSMeneghelliGBragaRZacchelloFBaraldiEOffice spirometry in primary care pediatrics: a pilot studyPediatrics20051166e792e79716322136
- PoelsPJSchermerTRJacobsAVariation in spirometry utilization between trained general practitioners in practices equipped with a spirometerScand J Prim Health Care2006242818716690555
- LucasAESmeenkFWSmeeleIJvan SchayckCPOvertreatment with inhaled corticosteroids and diagnostic problems in primary care patients, an exploratory studyFam Pract2008252869118304973
- GrantENMoyJNTurner-RoanKDaughertySRWeissKBAsthma care practices, perceptions, and beliefs of Chicago-area primary-care physicians. Chicago Asthma Surveillance Initiative Project TeamChest1999116145S154S10532476
- Martínez EizaguirreJMIrizar AranburuMIEstirado VeraCBerraondo ZabaleguiISan Vicente BlancoRAguirre CanflancaEQuality of spirometry tests done in primary care units in the province of GipuzkoaAten Primaria2008540523525918482542
- ShimCSWilliamsMHJrEvaluation of the severity of asthma: patients versus physiciansAm J Med19806811137350797
- TsuyukiRTSinDDSharpeHMCowieRLNilssonCManSFAlberta Strategy to Help Manage Asthma (ASTHMA) InvestigatorsManagement of asthma among community-based primary care physiciansJ Asthma200542316316715962871
- GharagozlouMAbdollahpourHMoinfarZBemanianMHSedaghatMA survey of pediatricians’ knowledge on asthma management in childrenIran J Allergy Asthma Immunol200872859018552410
- CowenMKWakefieldDBCloutierMMClassifying asthma severity: objective versus subjective measuresJ Asthma200744971171517994399