Abstract
Prior studies have demonstrated the effectiveness of noninvasive transdermal insulin delivery using a cymbal transducer array. In this study the physiologic response to ultrasound mediated transdermal insulin delivery is compared to that of subcutaneously administered insulin. Anesthetized rats (350–550 g) were divided into four groups of four animals; one group representing ultrasound mediated insulin delivery and three representing subcutaneously administered insulin (0.15, 0.20, and 0.25 U/kg). The cymbal array was operated for 60 minutes at 20 kHz with 100 mW/cm2 spatial-peak temporal-peak intensity and a 20% duty cycle. The blood glucose level was determined at the beginning of the experiment and, following insulin administration, every 15 minutes for 90 minutes for both the ultrasound and injection groups. The change in blood glucose from baseline was compared between groups. When administered by subcutaneous injection at insulin doses of 0.15 and 0.20 U/kg, there was little change in the blood glucose levels over the 90 minute experiment. Following subcutaneous administration of insulin at a dose of 0.25 U/kg, blood glucose decreased by 190 ± 96 mg/dl (mean ± SD) at 90 minutes. The change in blood glucose following ultrasound mediated insulin delivery was −262 ± 40 mg/dl at 90 minutes. As expected, the magnitude of change in blood glucose between the three injection groups was dependant on the dose of insulin administered. The change in blood glucose in the ultrasound group was greater than that observed in the injection groups suggesting that a higher effective dose of insulin was delivered.
Introduction
Transdermal drug delivery has been studied as an alternative method for noninvasive drug administration. However, the use of this method has been limited because the superficial layer of the skin, the stratum corneum, is not sufficiently permeable to allow effective transfer of medication into the bloodstream. To enhance transportion of drugs through the skin, several approaches, including chemical enhancers (CitationJohnson et al 1996), iontophoresis (CitationWang et al 2005), microneedles (CitationNanda et al 2006), electroporation (CitationPrausnitz et al 1993, Citation2004) and ultrasound (CitationPitt et al 2004; CitationMitragotri and Kost 2004; CitationSmith 2007) have been studied as an alternative to needles. Currently, the transdermal transport of insulin is of interest due to the current 21 million Americans who have this disease (CitationCEDR 1999; CitationThe Whitaker Foundation 2004; CitationHussain et al 2007). Diabetes is one of the most costly ailments and its management often requires painful, repetitive insulin injections as often as four times each day.
Of the experiments using ultrasound, many were focused on the feasibility of the approach (CitationTachibana and Tachibana 1991; CitationBoucaud et al 2002; CitationLee et al 2004a). Some researchers have studied the effects of frequencies and intensities on the effectiveness of ultrasonic delivery in an effort to understand the mechanisms by which ultrasound enhances transdermal delivery (CitationMachet and Boucaud 2002; CitationMerino et al 2003; CitationSchlicher et al 2006). While ultrasound is effective, the relationship between the intensities and potential bioeffects has yet to be determined (CitationWu et al 1998; CitationDoukas and Kollias 2004). Additionally there is limited understanding as how the intensities relates to the amount of insulin transported via ultrasound (CitationLuis et al 2007) or to direct injections. To date, many ultrasound drug delivery experiments on enhanced transdermal drug delivery are performed using sonicators, ultrasonic baths, or commercially made (“off-the-shelf”) transducers (CitationTachibana and Tachibana 1991; CitationSantoianni et al 2004; CitationPitt et al 2004; CitationSmith 2007). The large sizes of these devices and the difficulty of transporting them have been significant disadvantages associated with their practical use for noninvasive drug delivery. Commercial sonicators are large, heavy, tabletop devices specially designed for lysis of cells or catalyzing reactions. In order to become a practical portable ultrasound device, there is the need for a smaller transducer which can work in the same frequency range (CitationPitt et al 2004). Additionally it is important to balance ultrasound safety (dosimetry) versus efficacy since large intensities can also cause damage (CitationWu et al 1998; CitationLee et al 2005).
To meet the demand for a practical portable device, a small-sized, low-profile, and lightweight cymbal transducer has been used for the transdermal delivery of insulin. This flextensional transducer has a thickness of less than 2 mm, weighs less than 3 grams and resonates between 1 and 100 kHz (CitationNewnham et al 1991; CitationMaione et al 2002). The cymbal transducer array has previously demonstrated enhancement in transport of insulin for in vitro human skin (CitationSmith et al 2003a), in vivo rats (CitationSmith et al 2003b), rabbits (CitationLee et al 2004b; CitationSnyder et al 2006), and large pigs (CitationPark et al 2007). One of the many questions with this approach is the relationship between the levels of glucose decrease from ultrasound versus a direct subcutaneous injection of insulin. Therefore the purpose of this research is to examine the blood glucose response from direct injections of insulin against the ultrasound intensity from a cymbal array.
Materials and methods
Ultrasound transducer array
Details regarding the design and construction of the cymbal transducer and the multi-element array have been described elsewhere (CitationNewnham et al 1991, Citation1994; CitationMaione et al 2002). Briefly, the cymbal transducer is a novel flextensional transducer capable of producing very low frequencies (). A cymbal transducer has a compact, lightweight structure with an adjustable resonance frequency. In the cymbal transducer design, the caps on the lead zirconate – titanate (PZT) ceramic contained a shallow cavity beneath the inner surface. The fundamental mode of vibration is the flexing of the end caps caused by the radial motion of the ceramic. Therefore, the overall displacement of the device is a combination of the axial motion of the disk plus the radial motion amplified by the end caps. Amplification factors can be as high as 40 times that of the ceramic by itself (CitationMeyer et al 2001). Specifically, the piezoelectric disc was made from PZT-4 (Piezokinetics, Inc., Bellefonte, PA), had a diameter of 12.7 mm, and was 1 mm thick. Caps were made of 0.25-mm thick titanium while the thin glue layer between the caps and the ceramic disk was made of Eccobond® (Emerson and Cuming, Billerica, MA) epoxy. For the array, four transducers were connected in parallel and encased in URALITE® polymer (FH 3550, H.B. Fuller, St. Paul, MN) to produce a transducer array arrangement.
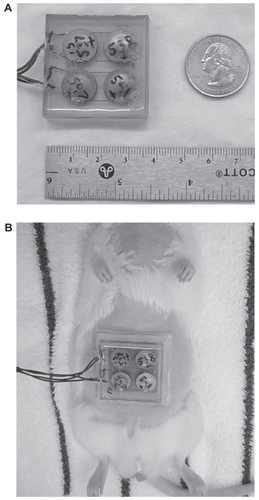
Figure 1 (A) For the cymbal array made up of four cymbal transducers, the cymbal elements were connected in parallel, encased in URALITE® polymer and arranged in a two-by-two elemental pattern. The dimensions of the array were 37 × 37 × 7 mm3 and it weighed less than 20 g. (B) Photograph of a transdermal insulin delivery experiment with a rat placed in a dorsal decubitus position with the array attached. A 1 mm thick water tight standoff was arranged between the abdominal area and the array. The reservoir within the standoff was filled with insulin through a small hole in the back of the array.
The array was driven by a radio frequency (RF) signal generated by a pulse/function generator (Model 393, Wavetek Inc., San Diego, CA) and amplified by an RF amplifier (Model 40A12, Amplifier Research, Souderton, PA). The electrical impedance of the array was matched to the output impedance of the amplifier by an external inductor-capacitor tuning network. Pulse period, duty cycle, and exposure time of the RF signal from the frequency generator was monitored using an oscilloscope (Tektronix 2213A, Beaverton, OR). For the ultrasound exposure experiments, the array was operated at 20 kHz with a pulse duration of 200 ms and a pulse repetition period of 1 second (ie, 20% duty cycle). Pulsed ultrasound was used to avoid damaging either the array or the animal’s skin by excessive heat generation.
Ultrasound exposimetry
The intensity was determined according to exposimetry guidelines established by the American Institute of Ultrasound in Medicine (CitationIEEE 1990; CitationAIUM 1998). For the acoustic field at a plane 1 mm from the transducer face, the ultrasonic intensities from the array were measured with a calibrated miniature (4 mm diameter) omnidirectional reference hydrophone (Model TC4013, S/N: 5199093, RESON, Inc., Goleta, CA). The cymbal array was submerged in a water tank (51 × 54 × 122 cm3) which was made almost anechoic by placing 1.27 cm thick rubber sound absorbing material around its wall. A custom made degasser, built in-house, reduced the dissolved oxygen content of the distilled water to 1–2 ppm to reduce cavitation effects. Pulse period, duty cycle and exposure time of the signal from the frequency generator and hydrophone was acquired using an Agilent 54622A 100 MHz digitizing oscilloscope (Agilent, Palo Alto, CA).
Precise, computer-controlled positioning of the hydrophone was performed by a Velmex Positioning System (Velmex Inc., East Bloomfield, NY). Pressure waves detected by the hydrophone were recorded by a digitizing oscilloscope. A computer-controlled exposimetry positioning system was used for automated scanning. The scanning step size for each device was 1 mm and the scanning area was 40 × 40 mm2. Spatial peak-temporal peak (Isptp) intensity were determined over a plane 1 mm from the array face using the hydrophone based on three scannings of the array for a mean and standard deviation of the intensity results. The intensity of cymbal transducer array was Isptp = 102.2 ± 2.3 mW/cm2.
Animal experiments
All procedures described in this report involving live animals were approved by the Institutional Animal Care and Use Committee (IACUC) at the Pennsylvania State University. A total of 16 experiments using eight Sprague-Dawley rats (350–550 g) were performed in four experimental groups with four rats in each group: one ultrasonic transdermal delivery and three subcutaneous injection groups. Rats were anesthetized with a combination of ketamine hydrochloride (60 mg/kg intramuscularly, Ketaject®, Phoenix, St. Joseph, MO) and xylazine hydrochloride (10 mg/kg intramuscularly, Xyla-Ject®, Phoenix, St. Joseph, MO). In addition to its role in general anesthesia, xylazine was used to induce a temporary, but sustained (up to 12 hrs), hyperglycemia in rats (CitationPavlovic et al 1996; CitationKawai et al 1999).
For the ultrasonic transdermal delivery, the abdominal area of the rat was shaved using an electric shaver and a depilatory agent was applied to the skin to eliminate any remaining hair. After shaving, a 1-mm thick, water-tight standoff was attached () between the skin and the array. With the rat in the dorsal decubitus position, a reservoir within the standoff was filled with insulin (Humulin® R, rDNA U-100, Eli Lilly and Co., Indianapolis, IN) through a small hole in the array. Care was taken to remove all bubbles from the solution in the reservoir to prevent disruption of ultrasound transmission. The elapsed time from the initial injection of the anesthetic until the start of ultrasound exposure was no longer than 25 minutes. For the ultrasound exposure, the cymbal array was operated at 20 kHz with an Isptp = 100 mW/cm2 for 60 minutes. After the 60 minutes ultrasound exposure, the array was removed and the skin examined for visible lesions.
The dose of insulin selected for the injection groups was based on published insulin doses used to control diabetes mellitus in other species and on pilot experiments (not reported). Humulin® R Insulin (100 U/ml) was diluted with a 0.9% saline solution (Phoenix Pharmaceutical, Inc., St. Joseph, MO) to 0.5 U/ml and delivered subcutaneously (under the skin of the ventral abdomen) at 0.15, 0.20, or 0.25 U/kg.
Blood was collected from the tail vein of each rat to obtain a baseline glucose level and, following insulin administration, additional samples were collected every 15 minutes for 90 minutes. For the ultrasonic transdermal delivery, the base line glucose level was measured at the beginning of the ultrasound exposure. The blood glucose level (mg/dl) for each sample was determined using the ACCU-CHEK™ blood glucose monitoring system (Roche Diagnostics Co., Indianapolis, IN). Each sample was tested at least twice to confirm the accuracy of the reading.
The data was corrected by subtracting the baseline glucose for each animal from each data point such that only changes in blood glucose were compared. Statistical analysis was performed using Microsoft Excel® (Microsoft Corp., Redmond, WA) and the data of blood glucose versus time were pooled for each group and analyzed as the mean and standard deviation. A t-test was used to analyze the statistical significance of the differences among the means of groups. The p-value was used to determine if the between-group differences are significantly greater than chance.
Results
Results of the ultrasound delivery compared with injection doses for the four groups are graphed as the decrease in the blood glucose level during the 90 minute experiment (). Data were graphed and reported as the mean ± standard deviation (x ± SD) of each group. Due to the anesthesia, the average initial glucose level at the beginning of the experiment was 340 ± 69 mg/dl for the 16 experiments. Rats not anesthetized with xylazine would have a blood glucose closer to a normal level of ~100 mg/dl (CitationHarkness and Wagner 1995; CitationHillyer and Quesenberry 1997).
Figure 2 Over a period of 90 minutes, the blood glucose level of rats decreased to −262 ± 40 mg/dl at 90 minutes for ultrasound mediated transdermal insulin delivery (▪) while there was less than 32 mg/dl change for both 0.15 U/kg (●) and 0.20 U/kg (▴) injection groups. For the 0.25 U/kg (♦) injection group, the glucose level decreased to and −190 ± 96 mg/dl at 90 minutes.
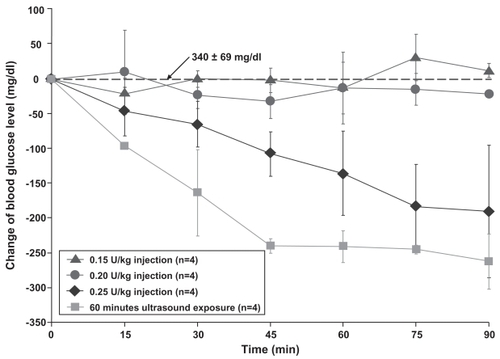
For direct subcutaneous injections with the dose of 0.15 U/kg and 0.20 U/kg, the blood glucose level deviated little from the baseline value. Overall the glucose level varied no greater than 32 mg/dl from the initial value over a 90 minute experimental period for both doses. Yet for a subcutaneous insulin injection of 0.25 U/kg, the blood glucose decreased by 190 ± 96 mg/dl after 90 minutes. In comparison, the ultrasound produced a blood glucose decrease of 263 ± 40 mg/dl at 90 minutes. A t-test analysis at 90 minutes indicated that all the groups were statistically different from each other at a p-level less than 0.01. Visual examination of the skin exposed to ultrasound did not indicate any damage or significant change to the skin.
Discussion
For humans to regulate their blood glucose level, the required insulin injection dose is 0.5–1 U/kg/day for adults and children and 0.8–1.2 U/kg for adolescents experiencing growth spurts (CitationLance et al 2002; CitationHodgson and Robert 2006). Direct subcutaneous injection doses for animals range from 0.1–0.4 U/kg subcutaneous (SC) for dogs and 0.1–0.5 U/kg (SC) for ferrets (CitationPlumb 2005). Ranges are given since physiological variables have a direct effect on the specific blood glucose decrease from injections. As many clinicians and diabetes patients know, the body’s glucose response to direct injections varies according to a host of variables such as body weight, fat percentage, exercise level, and composition of the most recent meal. Consistency of diet and exercise along with routine dose-glucose recording aids in the control of blood glucose. Without proper glucose control, diabetic complications may include renal failure, peripheral vascular disease, and limb amputation (CitationSuetsugu et al 2007; CitationMeeuwisse-Pasterkamp et al 2008).
To facilitate the ability of a diabetic patient to avoid repeated painful daily injections of insulin, a safe, lightweight, low-profile, inexpensive and potentially portable ultrasonic device is proposed. The goal was to develop an approximate relationship between dose levels from direct subcutaneous injections and noninvasive ultrasound at a Isptp ~100 mW/cm2 for 60 minutes. While an exact mathematical relationship was not determined, the results in indicate that the ultrasound dose appears to be greater than an injection dose of 0.25 U/kg for rats. Not included in the results was a single rat experiment which used a direct injection dose of 0.44 U/kg which resulted in a rapid blood glucose decrease of 290.5 ± 8 mg/dl after only 60 minutes. Given the rapid glucose decrease, the animal was removed from the experiment and this dose was determined to be too high for the rats. Yet the single point result can indicate that the ultrasound dose would be somewhere between injection dose levels of 0.25–0.44 U/kg. Nevertheless the results are the first steps in determining a relationship between ultrasound intensity levels and insulin dose responses. Further experiments should explore the use of larger animals with a similar size and weight as humans or animal which are truly diabetic such as pancreatectomized pig.
In terms of human diabetes, a person is considered diabetic if their blood sugar level is above 126 mg/dl after eight hours of fasting. People without diabetes have fasting sugar levels that generally run between 70–110 mg/dl. A glucose of 110–126 mg/dl is classified as impaired fasting glucose. In the oral glucose tolerance test, 140–200 mg/dl is impaired glucose tolerance and greater than 200 mg/dl is considered diabetic (CitationRifkin and Porte 1990; CitationShaw et al 1999; CitationCarnevale Schianca et al 2003). For the last situation a diabetic person would need to inject enough insulin to reduce their blood glucose by about 100 mg/dl. Both the ultrasound and direct injection of 0.25 U/kg achieve blood glucose level decreases of 190 mg/dl or greater.
Use of transdermal drug delivery techniques has practical clinical application to medications which need to be injected multiple times either daily or weekly. A recent review on ultrasound drug delivery states that “small-sized low-frequency transducers need to be developed so that patients can wear them” (CitationPitt et al 2004). As with diagnostic ultrasound imaging, drug delivery using therapeutic ultrasound requires a delicate balance between safety and efficacy and requires careful scientific study. For a transdermal device to replace conventional needles, the bioeffects and safety of each device needs to be carefully evaluated since it will not matter how much of any drug can be transported if the skin is damaged or the procedure is painful.
Acknowledgments
This work was supported by the Department of Defense Technologies for Metabolic Monitoring Award Number W81XWH-05-1-0617. There are no conflicts of interest to report.
References
- [AIUM] American Institute of Ultrasound in Medicine1998Acoustic output labeling standard for diagnostic ultrasound equipmentLaurel, MDAmerican Institute of Ultrasound in Medicine
- BoucaudAGarrigueMAMachetL2002Effect of sonication parameters on transdermal delivery of insulin to hairless ratsJ Control Release811131911992684
- Carnevale SchiancaGPRossiASainaghiPP2003The significance of impaired fasting glucose versus impaired glucose tolerance: importance of insulin secretion and resistanceDiabetes Care261333712716784
- [CEDR] Congressionally Established Diabetes Research Working Group1999Conquering Diabetes: A Strategic Plan for the 21st Century NIH Publication No. 99–4398
- DoukasAGKolliasN2004Transdermal drug delivery with a pressure waveAdv Drug Deliv Rev565597915019746
- HarknessJEWagnerDJ1995The Biology and Medicine of Rabbits and RodentsBaltimore MDWilliams and Willkins
- HillyerEQuesenberryKE1997Ferrets, Rabbits, and Rodents: Clinical Medicine and SurgeryPhiladelphia PAW.B. Saunders Co
- HodgsonBBRobertJ2006Saunders Nursing Drug Handbook 2006St. Louis, MissouriElsevier Saunders
- HussainAClaussenBRamachandranA2007Prevention of type 2 diabetes: a reviewDiabetes Res Clin Pract763172617069920
- [IEEE] Institute of Electrical and Electronics Engineers1990IEEE Guide for Medical Ultrasound Field Parameter MeasurementsNew YorkInstitute of Electrical and Electronics Engineers, Inc
- JohnsonMEMitragotriSPatelA1996Synergistic effects of chemical enhancers and therapeutic ultrasound on transdermal drug deliveryJ Pharm Sci8567098818988
- KawaiNStummerWEnnisSR1999Blood-brain barrier glutamine transport during normoglycemic and hyperglycemic focal cerebral ischemiaJ Cereb Blood Flow Metab1979869886358
- LanceLLLacyCFGoldmanMP2002Quick Look Drug BookPhiladelphia, PALippincott Williams and Wilkins
- LeeSNayakVDoddsJ2005Glucose measurements with sensors and ultrasoundUltrasound Med Biol31971715972203
- LeeSNewnhamRESmithNB2004aShort ultrasound exposure times for noninvasive insulin delivery in rats using the light weight cymbal arrayIEEE Transactions on Ultrasonics, Ferroelectrics and Frequency Control5117680
- LeeSSnyderBNewnhamRE2004bNoninvasive ultrasonic transdermal insulin delivery in rabbits using the light-weight cymbal arrayDiabetes Technol Ther68081515684633
- LuisJSmithNBMeyerRJ2007Rectangular cymbal arrays for improved ultrasonic transdermal insulin deliveryJ Acoust Soc Am12220223017902839
- MachetLBoucaudA2002Phonophoresis: efficiency, mechanisms and skin toleranceInt J Pharm2431–211512176291
- MaioneEShungKKMeyerRJ2002Transducer design for a portable ultrasound enhanced transdermal drug delivery systemIEEE Transactions on Ultrasonics, Ferroelectrics and Frequency Control4914306
- Meeuwisse-PasterkampSHvan der KlauwMMWolffenbuttelBH2008Type 2 diabetes mellitus: prevention of macrovascular complicationsExpert Rev Cardiovasc Ther63234118327994
- MerinoGKaliaYNDelgado-CharroMB2003Frequency and thermal effects on the enhancement of transdermal transport by sonophoresisJ Control Release88859412586506
- MeyerRJDoganAYoonC2001Displacement amplification of electroactive materials using the cymbal flextensional transducerSensors Actuators8715762
- MitragotriSKostJ2004Low-frequency sonophoresis: a reviewAdv Drug Deliv Rev5658960115019748
- NandaANandaSGhilzaiNM2006Current developments using emerging transdermal technologies in physical enhancement methodsCurr Drug Deliv32334216848725
- NewnhamREXuQCYoshikawaS1994Metal-electroactive ceramic composite actuatorsJ Acoust Soc Am973215
- NewnhamREXuQCYoshikawaS1991Transformed stress direction acoustic transducerJ Acoust Soc Am9111989
- ParkEJWernerJSmithNB2007Ultrasound mediated transdermal insulin delivery in pigs using a lightweight transducerPharm Res24139640117443398
- PavlovicMWroblewskiKManevichY1996The importance of choice of anesthetics in studying radiation effects in the 9L rat gliomaBr J Cancer Suppl27S22258763885
- PittWGHusseiniGAStaplesBJ2004Ultrasonic drug delivery – a general reviewExpert Opin Drug Deliv1375616296719
- PlumbDC2005Plumb’s Veterinary Drug HandbookStockholm, WisconsinPharma Vet Inc
- PrausnitzMRBoseVGWeaverJ1993Electroporation of mammalian skin: A mechanism to enhance transdermal drug deliveryProc Natl Acad Sci USA901050488248137
- PrausnitzMRMitragotriSLangerR2004Current status and future potential of transdermal drug deliveryNat Rev Drug Discov31152415040576
- RifkinHPorteD1990Ellenberg and Rifkin’s DiabetesNew York, NYElsevier Science
- SantoianniPNinoMCalabroG2004Intradermal drug delivery by low-frequency sonophoresis (25 kHz)Dermatol Online1024
- SchlicherRKRadhakrishnaHTolentinoTP2006Mechanism of intracellular delivery by acoustic cavitationUltrasound Med Biol329152416785013
- ShawJEZimmetPZde CourtM1999Impaired fasting glucose or impaired glucose tolerance. What best predicts future diabetes in Mauritius?Diabetes Care2239940210097917
- SmithNB2007Perspectives on Transdermal Ultrasound Mediated Drug DeliveryInt J Nanomed258594
- SmithNBLeeSMaioneE2003aUltrasound mediated transdermal transport of insulin through in vitro human skin using novel transducer designsUltrasound Med Biol293111712659919
- SmithNBLeeSShungKK2003bUltrasound-mediated transdermal in vivo transport of insulin with low-profile cymbal arraysUltrasound Med Biol2912051012946523
- SnyderBLeeSNewnhamRE2006Ferroelectric transducer arrays for transdermal insulin deliveryJ Mater Sci4121116
- SuetsuguMTakebayashiKAsoY2007Association between diabetic microangiopathy and vascular endothelial function evaluated by flow-mediated vasodilatation in patients with type 2 diabetesInt J Clin Pract61920617343657
- TachibanaKTachibanaS1991Transdermal delivery of insulin by ultrasonic vibrationJ Pharm Pharmacol4327011676740
- The Whitaker Foundation2004Biomedical Engineering and the Fight Against Diabetes, 2003 Annual ReportArlington, VAThe Whitaker Foundation
- WangYThakurRFanQ2005Transdermal iontophoresis: combination strategies to improve transdermal iontophoretic drug deliveryEur J Pharm Biopharm601799115939232
- WuJChappelowJYangJ1998Defects generated in human stratum corneum specimens by ultrasoundUltrasound Med Biol24705109695274