Abstract
Hyponatremia is an electrolyte disorder frequently observed in several clinical settings and common in hospitalized patients with decompensated heart failure (HF). It is caused by deregulation of arginine vasopressin (AVP) homeostasis associated with water retention in hypervolemic or in euvolemic states. While hypervolemic hypotonic hyponatremia is also seen in advanced liver cirrhosis, renal failure, and nephrotic syndrome, the bulk of evidence associating this electrolyte disorder to increasing morbidity and mortality can be found in the HF literature. Hospitalized HF patients with low serum sodium concentration have lower short-term and long-term survival, longer hospital stay and increased readmission rates. Conventional therapeutic approaches, ie, restriction of fluid intake, saline and diuretics, can be effective, but often the results are unpredictable. Recent clinical trials have demonstrated the effectiveness of nonpeptide AVP receptor antagonists (vaptans) in the treatment of hyponatremia. The vaptans induce aquaresis, an electrolyte-sparing excretion of free water resulting in the correction of serum sodium concentrations and plasma osmolality, without activation of the renin-angiotensin-aldosterone system (RAAS) or changes in renal function and blood pressure. Further prospective studies in a selected congestive HF population with hyponatremia, using clinical-status titrated dose of tolvaptan, are needed to determine whether serum sodium normalization will be translated into a better long-term prognosis. This review will focus on recent clinical trials with tolvaptan, an oral V2 receptor antagonist, in HF patients. The ability of tolvaptan to safely increase serum sodium concentration without activating the RAAS or compromising renal function and electrolyte balance makes it an attractive agent for treating hyponatremic HF patients.
Introduction
Sodium homeostasis is vital to the normal physiologic function of the cells. Sodium concentration is regulated by stimulation of thirst, secretion of antidiuretic hormone (ADH), feedback mechanisms of the renin-angiotensin-aldosterone system (RAAS), and variations in renal handling of filtered sodium.
Hyponatremia is defined as serum sodium level of <135 mEq/L and is considered severe when the serum sodium level is <125 mEq/L. It is an important and common electrolyte abnormality that can be seen in isolation or, as most often is the case, as a complication of other medical illnesses associated with hypervolemia such as heart failure (HF), liver cirrhosis and the syndrome of inappropriate antidiuretic hormone secretion (SIADH).Citation1
The clinical manifestations depend on the severity and duration of hyponatremia and rapidity of decrease in sodium levels. Signs and symptoms of acute (<48 hours) severe hyponatremia are primarily related to the central nervous system as the osmotic pressure gradient promotes water movement into brain cells, resulting in life-threatening cerebral edema and encephalopathy.Citation2 Patients with chronic hyponatremia or a serum sodium level from 125 to 134 mmol/L may be asymptomatic or have less severe symptoms (fatigue, nausea, vomiting, and anorexia).
However in spite of a less serious clinical manifestations, hyponatremia is a predictor of poor outcomes in patients with HF, and the pathogenesis of this disorder reflects the underlying severity of HF, as well as attempts to manage fluid overload.Citation3 This review will focus on hyponatremia in HF setting and the role of the V2 receptor antagonist tolvaptan in its management.
Hyponatremia in heart failure
Pathogenesis
Hyponatremia is a common electrolyte disorder in patients with decompensated HF (19 to 25%)Citation4,Citation5 and is frequently a complication of diuretic therapy.Citation6 Its pathogenesis is multi-factorial. Neurohormonal activation, in response to decreased cardiac output, plays an important role in the pathophysiology of HF and hyponatremia. One of the most important etiologies of hyponatremia in this setting is an inappropriate secretion of AVP, making vasopressin receptors antagonism as a target for therapy for HF patients.Citation7 The decrease of effective circulating volume and consequently the sympathetic nervous system (SNS) and RAAS activation lead to an increase in nonosmotically released AVP. The non-osmotic release of AVP might override the hypo-osmolality negative feedback on AVP production.Citation8
Diuretic therapy induces hyponatremia because of the impairment of the kidney’s capability to reabsorb solute in the absence of water, the reduction of glomerular filtration rate due to volume depletion and the activation of the AVP system due to effective circulating volume decrease. Furthermore, the activation of the RAAS and SNS in response to diuretics contributes to the development of electrolyte disturbances and blunts the kidney response to diuretics in an effort to compensate for the changes in sodium and water balance.Citation8
Vasopressin through stimulation of V1 and V2 receptors aggravates the progression of HF, adversely affecting ventricular remodeling, worsening clinical congestion and contributing to hyponatremia. The V1a receptor is a G protein-coupled receptor which, when activated, increases intracellular calcium through the inositol-triphosphate pathway.Citation9 Prolonged V1a receptor stimulation causes both arterial and venous constriction increasing myocardial preload and afterload. Direct myocardial V1a receptor stimulation also contributes to left ventricular hypertrophy and adverse remodeling.
The V2 receptor, located in the renal collecting tubular cells, is linked to the adenylate cyclase signaling pathway, with intracellular cyclic adenosine monophosphate (cAMP) acting as the second messenger. V2 receptor mediates the ADH-induced stimulation of water permeability thereby permitting osmotic equilibration with the renal interstitium.Citation10 The inappropriate activation of the renal V2 receptors contributes to excessive water retention, volume expansion, increase of cardiac preload and dilutional hypo-osmolality with hypotonic hyponatremia. All these mechanisms perpetuate a vicious circle that can lead to disease progression and a worsening of the clinical status and prognosis of HF patients.Citation11
Prognostic significance
Low serum sodium concentration in the setting of congestion may be a marker of increased neurohormonal activation and greater severity of disease. The prognostic importance of hyponatremia in patients with severe chronic HF was first described by Lee and Packer.Citation12 Five variables including serum sodium concentration, left ventricular stroke work index, serum creatinine concentration, serum bilirubin, and age were found to predict survival and pretreatment hyponatremia was the most powerful predictor of long term prognosis.
Several later studies demonstrated that hyponatremia at the time of admission is related to poor outcomes in patients hospitalized for acute heart failure syndrome (AHFS). A randomized trial on 282 patients on the effect of nurse-directed, multidisciplinary intervention in comparison with usual care on 90-day readmission rates after AHFS hospitalization found that a decreasing plasma sodium level was one of the five independent predictors of readmission.Citation13 Another study of 4031 community-based patients hospitalized for worsening HF has shown that hyponatremia is one of the multivariable predictors of mortality at both 30 days and 1 year.Citation1
Similar results emerged from retrospective analyses of several large randomized clinical trials. Investigators explored the relationship between admission serum sodium concentration and short term mortality in the OPTIME-CHF trial.Citation14 There were 949 patients with AHFS randomized to receive 48 to 72 hours of intravenous milrinone or placebo in addition to standard therapy. In this study population, 27% of patients were in the lowest sodium quartile (ie, serum sodium concentration <135 mEq/L). The number of hospitalization days for cardiovascular causes was 33% higher in this group and they also had a 2-fold higher in-hospital and 60-day mortality compared to those in the other plasma sodium quartiles. Similar results were also noted in another study among HF patients with preserved systolic function and hyponatremia.Citation15
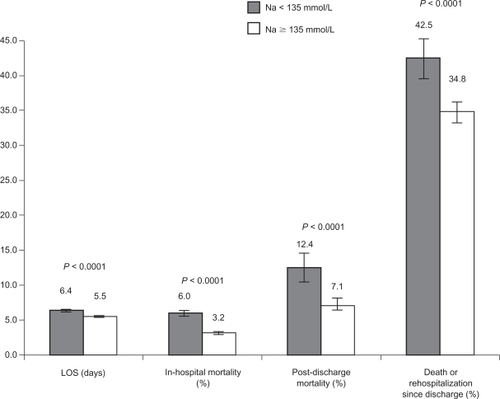
An analysis from the OPTIMIZE-HF registry of 48,612 patients with AHFS showed a relationship between admission serum sodium concentration and clinical outcomes.Citation16 Hyponatremia was present in 20% of the OPTIMIZE-HF cohorts with similar prevalence in patients with reduced or preserved ejection fraction. Lower admission serum sodium levels were associated with higher in-hospital mortality and longer mean hospital length of stay. In the follow up cohort, admission hyponatremia was associated with higher 60- to 90-day mortality. Admission serum sodium concentration remained a significant independent predictor of outcomes after adjustment for other prognostic factors ().
Figure 1 Hyponatremia and prognosis in heart failure patients.
A post-hoc analysis of the ESCAPE trial evaluated the correlation of hyponatremia with hemodynamic status in patients hospitalized with severe HF.Citation17 This study was designed to evaluate the utility of pulmonary artery catheter in 433 patients hospitalized with severe HF (NYHA IV and LVEF < 30%). Patients were followed up for 180 days after discharge. Hyponatremia was initially present in 23.8% of study population and persisted during hospitalization in 68.9% of these patients. After covariate adjustment, results confirmed that baseline serum sodium levels were an independent predictor of 6 month mortality. Persistent hyponatremia was also associated with a significant increase of HF readmission rate as well as a composite endpoint of death and readmission rate. Moreover, the higher event rate associated with hyponatremic patients persists even after symptomatic and clinical improvement.
AVPV2-receptor selective antagonist: tolvaptan
Mechanism of action, pharmacokinetic and pharmacodynamic profile
Tolvaptan, also known as OPC-41061, is an orally active nonpeptide AVP antagonist. It selectively blocks the binding of AVP to V2 receptor and inhibits the AVP-induced production of cyclic AMP in human cells expressing V2 receptors. V2 receptor antagonism promotes free water clearance (aquaresis), decrease in urine osmolality, and rise of serum sodium concentration without disturbing plasma potassium and magnesium levels. Tolvaptan metabolites have none or minimal activity for human V2 receptors compared with active drug.Citation18
The pharmacokinetic, pharmacodynamic and drug interactions between tolvaptan and furosemide or hydrochlorothiazide (HCTZ) were studied in 12 healthy white men.Citation19 In subjects receiving 60 mg of tolvaptan, the onset of the aquaretic and sodium increasing effects occurs within 2 to 4 hours post-dose. A peak effect is observed between 4 and 8 hours post-dose. Tolvaptan resulted in a greater 24-hour urine volume/excretion rate than furosemide or HCTZ. However, concomitant administration of tolvaptan with furosemide or HCTZ resulted in a similar 24-hour urine volume/excretion rate compared with tolvaptan administration alone. In clinical studies on CHF patients, the addiction of tolvaptan to standard therapy, included furosemide, induced an increase in urine output compared to placebo plus diuretic. To confirm this possible synergic effect in HF patients, studies comparing tolvaptan alone versus tolvaptan plus diuretic effects are necessary.
Tolvaptan is metabolized by CYP3A system and concomitant use of strong CYP3A inhibitors such as clarithromycin or ketoconazole is cautioned.Citation20 Tolvaptan administration does not affect steady-state amiodarone concentration, an antiarrhythmic drug commonly prescribed for patients with congestive heart failure and a known inhibitor of other drugs metabolized by CYP3A4. Potent CYP3A inducers such as rifampicin reduced tolvaptan plasma concentrations by 85%. Tolvaptan is also a substrate for P-glycoprotein and administration with P-glycoprotein inhibitors such as cyclosporine requires a dose reduction.Citation21
Treatment with tolvaptan is associated with a reduction of the extracellular fluid volume which could result in increased serum potassium. Serum potassium levels should be monitored after initiation of tolvaptan treatment in patients with a serum potassium >5 mEq/L and in those who are receiving drugs known to increase serum potassium levels. Although specific interaction studies were not performed in CHF clinical studies tolvaptan was used concomitantly with standard therapy (including beta-blockers, angiotensin receptor blockers, angiotensin converting enzyme inhibitors and potassium sparing diuretics) and plasma potassium concentrations are not significantly changed.
Tolvaptan in experimental studies, human studies and clinical trials
Preclinical studies, conducted on animals and in healthy subjects, showed that V2 receptor antagonist administration produced aquaretic effect (increase in free water excretion) without sodium loss, without activation of the RAAS and changes of renal function.Citation22,Citation23 These favorable results appeared to be consistent among several clinical trials on HF patients ().
Table 1 Tolvaptan clinical trials in heart failure
Gheorghiade et al was the first to conduct a double-blind, randomized trial to evaluate the ability of tolvaptan to remove excess fluid when added to a diuretic therapy in patients with symptomatic chronic HF.Citation24 In this study, 254 outpatients with NYHA 2 or 3 HF were randomly assigned to receive placebo or one of three doses of tolvaptan (30, 45, or 60 mg/day) for 25 days in addition to standard therapy. The tolvaptan group demonstrated a significant decrease in body weight at day 1 that was maintained throughout the 25 days. Moreover, there was a significant improvement of clinical signs and symptoms observed. There was also an increase in urine output with significantly lower urine osmolality and urinary sodium concentration compared to placebo group. More hyponatremic patients in the tolvaptan group (80% vs 40% in placebo) had normalization in serum sodium levels. The increase in serum sodium starts at day 1 and maintained throughout the study. There were no changes in renal function or blood pressure.
The Acute and Chronic Therapeutic Impact of Vasopressin antagonist in congestive HF (ACTIV in CHF prospective trial) evaluated the clinical effects of tolvaptan in 319 patients hospitalized with worsening heart failure. All doses (30, 60, 90 mg/day) of tolvaptan resulted in significant body weight reduction over placebo.Citation25 Tolvaptan also improved serum sodium levels in patients with hyponatremia. There were no differences in worsening heart failure at 60 days between the tolvaptan and placebo groups (P = 0.88). However, while bodyweight declined on tolvaptan, there were no statistically significant differences in the signs and symptoms of clinical congestion, except for dyspnea (P = 0.04). Of note, patients randomized to tolvaptan used less furosemide and maintained a lower body weight, without differences in heart rate, blood pressure, potassium level or renal function. Retrospective analyses showed that patients with hyponatremia (21.3%) had a threefold increase in 60-day mortality compared with normonatremic patients and the improvement in hyponatremia during hospitalization, even if modest, was associated with improved outcomes.Citation26 Particularly a lower 60-day mortality in all tolvaptan groups compared to placebo group (P < 0.05) among patients with severe congestion and elevated blood urea nitrogen levels at baseline was detected.Citation27
The Study of Ascending Levels of Tolvaptan in hyponatremia 1 and 2 (SALT-1 and SALT-2) evaluated the effect of tolvaptan in patients with either euvolemic or hypervolemic hyponatremia due to SIADH, chronic HF or cirrhosis.Citation28 Tolvaptan was started at 15 mg/day, increased to 30 mg/day and then to 60 mg/day, if necessary, based on serum sodium concentration. Tolvaptan was more effective than placebo in increasing the average daily area under the curve for serum sodium concentrations during the first 4 days and after the full 30 days of therapy. Within 8 hours of the first administration of tolvaptan (first observation point), the serum sodium concentration was significantly higher in the tolvaptan group for both the total population and the subgroups stratified according to the degree of hyponatremia.
A multicenter, double-blind, placebo-controlled study, demonstrated that long term (1 year) administration of the tolvaptan (30 mg/day), have no significant effect on reducing left ventricular end-diastolic and end-systolic volume in 120 patients with stable CHF (NYHA II/III).Citation29 In this study there were no significant differences in serum sodium or potassium between groups across the year of therapy. A post hoc analysis showed a significant reduction in mortality and worsening HF over 1 year in patients treated with tolvaptan in comparison with placebo group (P = 0.027). These outcome findings were hypothesis generating of EVEREST program.
The EVEREST trial is a program of pivotal trials designed to investigate the effect of tolvaptan administration (30 mg/day) in addition to standard therapy in 4133 patients hospitalized for AHFS with signs and symptoms of volume overload. EVEREST consisted of three studies: 2 identical studies (A and B) designed to investigate short-term effects on clinical status and symptoms and an outcome study consisting of all randomized patients designed primarily to investigate long-term clinical outcomes of all cause mortality and combined cardiovascular mortality or HF readmissions.Citation30 The median follow-up period was 9.9 months. The short-term trials demonstrated a significant improvement in primary composite clinical end point (patient-assessed global clinical features and body weight loss at 7 day or discharge if earlier), and in secondary clinical end points (bodyweight loss at day 1 and day 7, patient-assessed dyspnea at day1, edema score at day 7) in patients treated with tolvaptan.Citation31
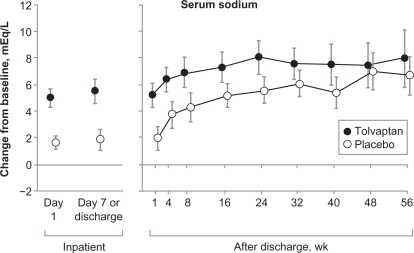
Among patients with baseline serum sodium levels <134 mEq/L (8% of total), the mean serum sodium concentration significantly increased in the tolvaptan group compared to placebo group. This effect was observed since day 1 and persisted throughout the follow-up period (). In spite of the significant improvement in short-term clinical status outcomes and in increasing sodium serum concentration among hyponatremic patients, tolvaptan administration in addition to standard therapy did not affect long term mortality or heart failure-related morbidity.Citation32 However dose titration of treatment considering clinical status (entity of dyspnea, peripheral edema, pulmonary congestion, body weight) and a dose adjustment based on clinical response could lead to better results in term of symptoms and outcomes.
Figure 2 Changes in serum sodium level (EVEREST trial).
Further prospective studies in a selected congestive HF population with hyponatremia, using clinical-status titrated dose of tolvaptan, are needed to determine whether serum sodium normalization will be translated into a better long-term prognosis.
Safety and tolerability
Symptomatic hyponatremia are true emergencies that demand prompt and definitive intervention. An important consideration in the treatment of hyponatremia is the rate at which serum sodium is corrected. Overly rapid correction of chronic hyponatremia leads to pontine and extrapontine myelinolysis that causes irreversible neurologic deficits. The challenge in treating severe hyponatremia is finding the right balance so as not to risk progression to cerebral edema from undercorrection of hyponatremia and avoid the osmotic demyelination syndrome from overcorrection of this electrolyte disorder.
Among patients with acute hyponatremia, defined as development of hyponatremia within 48 hours, the risk of persistent marked hyponatremia far exceeds any risk from correction of serum sodium and should not deter aggressive treatment. Patients seem to tolerate rates of correction that would be harmful for chronic hyponatremia (>48 hours).Citation33 There have been no reports of osmotic demyelination syndrome or related neurologic sequelae to date among patients who took or who are currently taking tolvaptan.
The data from clinical studies on short and long-term outcomes confirmed an overall safety profile of tolvaptan in a very large population of patients with HF and hyponatremia. In the EVEREST program the benefits on short term outcomes (consistent increases in urine output, a reduction in body weight, and an improvement in many signs and symptoms) have been seen without unfavorable changes in blood pressure, heart rate, electrolytes, or renal function. The neutral long-term outcome effects, different from other treatments in AHFS, confirm the safety of tolvaptan chronically administered.
The most common adverse effects (incidence ≥5% than placebo) to tolvaptan reported in clinical trials were thirst, dry mouth, polyuria and urinary frequency, which are consistent with the pharmacologic action of the drug. Other side effects reported, but not statistically significant in comparison with placebo (standard therapy), includes dehydration with hypotension, acute renal failure and hyperglycemia. Tolvaptan should not be used in hypovolemic hyponatremia or in patients with glomerular filtration rate less than 10 mL/min/1.73 m2, such as those with end stage renal disease with dilutional hyponatremia.Citation34
Implication for therapy
Conventional treatment of hyponatremia in HF patients is based largely on the restriction of fluid intake, saline and diuretic administration, but often these therapeutic approaches are ineffective.Citation35,Citation36 Hyponatremia in HF is frequently associated with reduced diuretic efficacy due to diminished distal tubular sodium delivery and secondary hyperaldosteronism. This could be particularly problematic when patients are not compliant with restrictions in free water intake.Citation37
A combination of hypertonic saline solution (HSS) and loop diuretics is often added to fluid restriction, but this more aggressive treatment is usually advocated for patients with severe hyponatremia who have profound neurological symptoms.Citation38 Licata et al studied the effects of high-dose furosemide and small-volume HSS infusion (group 1) in comparison with a high dose of furosemide as bolus (group 2) in 107 patients with refractory CHF who were unresponsive to high oral doses of furosemide.Citation39 A significant increase in daily diuresis and natriuresis was observed in both groups, but it was more significant in the group receiving HSS (P < 0.05). The serum sodium level increased in group 1 and decreased in group 2 (P < 0.05). HSS administration was well tolerated. It also improved the quality of life and potentiates the diuretic action of furosemide, overcoming established resistance to loop diuretics.
The V2 receptor antagonists may be viewed as the new class of agents for removing excess body water. These “aquaretic” agents have many favorable properties in comparison with loop diuretic.Citation9,Citation11,Citation39,Citation40 One in particular is its property to improve serum sodium concentrations and increase plasma osmolality without depletion of potassium, changes in blood pressure, renal function or neurohormonal activation. In comparison with furosemide, tolvaptan increased urine output without a decrease in renal blood flow and glomerular filtration rate.Citation40
Gheorghiade et al randomized tolvaptan alone versus fluid restriction plus placebo in 28 hospitalized patients with serum sodium concentration <135 mEq/L. Tolvaptan was started at 10 mg/day and titrated to 60 mg/day. Active treatment was continued for up to 27 days, with a follow-up until 65th day. Normalization of serum sodium (primary endpoint) occurred in 50% of patients by day 4 when treated with tolvaptan and by day 8 on fluid restriction (P < 0.03) with a significant greater increase of serum sodium concentration in the tolvaptan group compared to the fluid restriction group at their last inpatient visit.Citation41
The Food and Drug Administration (FDA) has approved the use of tolvaptan for the treatment of clinically significant hypervolemic and euvolemic hyponatremia (serum sodium concentration <125 mEq/L or less marked hyponatremia that is symptomatic and has resisted correction), including patients with HF, cirrhosis and SIADH.Citation42
Other vasopressin receptor antagonist
Lixivaptan (VPA-985) is another oral V2-receptor selective antagonist. In a multicenter, randomized, placebo-controlled trial,Citation43 lixivaptan appeared to be effective and safe in treatment of water retention and dilutional hyponatremia such as SIADH, HF and liver cirrhosis. Abraham et al investigated in a randomized, double-blind, placebo-controlled study the aquaretic response to increasing doses (10 to 400 mg single dose) of lixivaptan in 42 diuretic-requiring patients with mild-to-moderate CHF.Citation44 This study demonstrated a dose-dependent increase in solute-free water excretion and improvement in serum sodium concentration after V2 receptor antagonist treatment. Higher doses of lixivaptan may produce significant dehydration and will require close monitoring with their use.
At present, no long-term outcome data are available. The ongoing BALANCE study, a multicenter, randomized, double-blind placebo controlled trial designed to test the effects of titrated dose of lixivaptan administered for 60 days, on short- and long-term outcomes in hyponatremic patients with advanced HF. The primary end point of the study is the efficacy and safety of lixivaptan in normalizing serum sodium levels and reducing congestion in HF patients with hyponatremia. Secondary end point includes all cause mortality, HF hospitalization, cardiovascular effects and weight loss.Citation45
Conivaptan is the only intravenous combined V1a/V2 receptor antagonist that has been evaluated in humans and is FDA-approved for the treatment of euvolemic and hypervolemic hyponatremia.Citation42 Experimental studies showed that conivaptan has a good pharmacological profileCitation46 and is a potent inhibitor of AVP-induced protein synthesis of cardiomyocytes. It may have beneficial effects in the development and regression of cardiomyocyte hypertrophy.Citation47 Combined V1a/V2 receptor antagonists might be useful in diseases associated with a combination of increased peripheral resistance and dilutional hyponatremia.
Human studies in patients with stable advanced chronic HF showed that conivaptan induces a dose-dependent increase in urine output, decrease of pulmonary capillary wedge pressure, right atrial pressureCitation48 and improvement in serum sodium concentration.Citation49 Current plans for conivaptan are focused on treatment for AHFS. Recently, Goldsmith et al performed a pilot study to evaluate the efficacy and safety of intravenous conivaptan in treating AHFS.Citation50 The results of this study showed that conivaptan increases urine output significantly more than placebo. Conivaptan was well tolerated with no evidence of worsening HF. Further studies are still needed to determine the role of this drug in treatment of AHFS and hyponatremia.
Tolvaptan in other hyponatremic settings
Although the clinical manifestations are different for SIADH, liver cirrhosis, and HF, they share the same pathophysiologic mechanism responsible for persistent hyponatremia – nonosmotically stimulated AVP release. The efficacy of tolvaptan in improving euvolemic and hypervolemic hyponatremia due to SIADH or liver cirrhosis was tested in two trials previously mentioned. Excluding hypothyroidism, adrenal insufficiency, advanced renal disease (creatinine > 3.5 mg/dL), Child–Pugh score > 10, serum sodium concentration < 120 mEq/L with neurologic impairment, and systolic hypotension, the SALT-1 and SALT-2 trials found that tolvaptan was effective in increasing serum sodium concentration at day 4 and day 30 also in these hyponatremic settings. The improvement in serum sodium concentration also significantly improved the scores for the Mental Component Summary (for vitality, social functioning, emotionally limited accomplishment, calmness, and sadness) of the SF 12 Health survey.Citation28
Another potential clinical application of vasopressin receptor antagonists that is under investigation is its use in autosomal-dominant polycystic kidney disease (ADPKD). There are currently no good treatment options to retard progression of this condition and most patients require renal replacement therapy and/or renal transplantation. The morbidity and mortality associated with ADPKD is substantial. The vasopressin V2 receptors have been implicated in cyst formation and enlargement in polycystic kidney disease. The long-term safety and efficacy of tolvaptan in retarding (rate of renal volume change) progression of ADPKD is currently being studied.Citation51
Conclusion
Hyponatremia in HF is not just a mere inconvenience. It is an independent predictor of adverse outcomes including longer hospital stay, higher readmission rates, and increased short- and long-term mortality. The use of tolvaptan has been shown to induce a rapid and sustained aquaretic response useful for treatment of hyponatremia in patients with acute and chronic HF. Tolvaptan improves short-term outcomes and is proven to be safe in the treatment of AHFS, especially in hyponatremic settings. Further prospective studies of the vaptans, using titrated doses based on serum sodium and clinical status, are necessary to determine whether serum sodium normalization will be translated into a better long-term prognosis in selected hyponatremic patients with HF.
Disclosures
The authors declare no conflicts of interest.
References
- LeeDSAustinPCRouleauJLPredicting mortality among patients hospitalized for heart failure: derivation and validation of a clinical modelJAMA20032902581258714625335
- FallPJHyponatremia and hypernatremia: a systematic approach to causes and their correctionPostgrad Med2000107758210844943
- GheorghiadeMHellkampASPinaILHemodynamic characterization and prognostic value of persistent hyponatremia in patients with severe heart failure in the ESCAPE trialJ Am Coll Cardiol2005Suppl145A
- JanicicNVerbalisJGEvaluation and management of hypo-osmolality in hospitalized patientsEndocrinol Metab Clin North Am20033245948112800541
- HawkinsRCAge and gender as risk factors for hyponatremia and hypernatremiaClin Chim Act2003337169172
- SicaDASodium and water retention in heart failure and diuretic therapy: basic mechanismsCleve Clin J Med200673S2S716786906
- GoldsmithSRGheorghiadeMVasopressin antagonism in heart failureJ Am Coll Cardiol200546101785179116286160
- SchrierRWBerlTAndersonRJOsmotic and nonosmotic control of vasopressin releaseAm J Physiol19792364F321F332373467
- JardSMechanisms of action of vasopressin and vasopressin antagonistsKidney Int Suppl198826S38S422974096
- VerbalisJGVasopressin V2 receptor antagonistsJ Mol Endocrinol2002291912200224
- SicaDAHyponatremia and heart failure – pathophysiology and implicationsCongest Heart Fail20051127427716230871
- LeeWHPackerMPrognostic importance of serum sodium concentration and its modification by converting-enzyme inhibition in patients with severe chronic heart failureCirculation1986732572673002660
- RichMWBeckhamVWittenbergCLevenCLFreedlandKECarneyRMA multidisciplinary intervention to prevent the readmission of elderly patients with congestive heart failureN Engl J Med1995333119011957565975
- KleinLO’ConnorCMLeimbergerJDLower serum sodium is associated with increased short-term mortality in hospitalized patients with worsening heart failure: results from the Outcomes of a Prospective Trial of Intravenous Milrinone for Exacerbations of Chronic Heart Failure (OPTIME-CHF) studyCirculation20051112454256015867182
- RusinaruDBuiciucOLeborgneLSlamaMMassyZTribouilloyCRelation of serum sodium level to long-term outcome after a first hospitalization for heart failure with preserved ejection fractionAm J Cardiol200910340541019166698
- GheorghiadeMAbrahamWTAlbertNMOPTIMIZE-HF Investigators and CoordinatorsRelationship between admission serum sodium concentration and clinical outcomes in patients hospitalized for heart failure: an analysis from the OPTIMIZE-HF registryEur Heart J200728898098817309900
- GheorghiadeMRossiJSCottsWCharacterization and prognostic value of persistent hyponatremia in patients with severe heart failure in the ESCAPE trialArch Intern Med20071671998200517923601
- GhaliJKHamadBYasothanUKirkpatrickPTolvaptanNat Rev Drug Discov2009861161219644472
- ShoafSEBramerSLBricmontPZimmerCAPharmacokinetic and pharmacodynamic interaction between tolvaptan, an non-peptide AV antagonist and furosemide or hydrochlorothiazideJ Cardiovasc Pharmacol20075021321217703139
- ShoafSEElizariMVWangZTolvaptan administration does not affect steady state amiodarone concentrations in patients with cardiac arrhythmiasJ Cardiovasc Pharmacol Ther20051016517116211205
- KondoKOgawaHYamashitaH7-Chloro-5-hydroxy-1-[2-methyl-4-(2-methylbenzoyl-amino)benzoyl]-2,3,4,5-tetrahydro-1H-1-benzazepine (OPC-41061): a potent, orally active non-peptide arginine vasopressin V2 receptor antagonistBio org Med Chem1999717431754
- HiranoTYamamuraYNakamuraSOnogawaTMoriTEffects of the V2-receptor antagonist OPC-41061 and the loop diuretic furosemide alone and in combination in ratsJ Pharmacol Exp Ther200029228829410604960
- OhnishiAOritaYTakagiNAquaretic effect of a potent, orally active, non peptide V2 antagonist in menJ Pharmacol Exp Ther19952725465517853167
- GheorghiadeMNiaziIOuyangJCzerwiecFKambayashiJOrlandiCTolvaptan investigatorsVasopressin receptor blockade in patients with congestive heart failure: results from a randomized, double-blind studyCirculation20031072690269612742979
- GheorghiadeMGattisWAO’ConnorCMAcute and Chronic Therapeutic Impact of a Vasopressin Antagonist in Congestive Heart Failure (ACTIV in CHF) InvestigatorsEffects of tolvaptan, a vasopressin antagonist, in patients hospitalized with worsening heart failure: a randomized controlled trialJAMA20042911963197115113814
- RossiJBayramMUdelsonJEImprovement in hyponatremia during hospitalization for worsening heart failure is associated with improved outcomes: insights from the Acute and Chronic Therapeutic Impact of a Vasopressin Antagonist in Chronic Heart Failure (ACTIV in CHF) trialAcute Card Care20079828617573581
- FilippatosGRossiJLloyd-JonesDMPrognostic value of blood urea nitrogen in patients hospitalized with worsening heart failure: insights from the Acute and Chronic Therapeutic Impact of a Vasopressin Antagonist in Chronic Heart Failure (ACTIV in CHF) studyJ Card Fail20071336036417602982
- SchrierRWGrossPGheorghiadeMTolvaptan, a selective oral vasopressin V2-receptor antagonist, for hyponatremiaN Engl J Med2006552099211217105757
- UdelsonJEMcGrewFFloresEMulticenter randomized, double-blind, placebo-controlled study on the effect of oral tolvaptan on left ventricular dilation and function in patients with heart failure and systolic dysfunctionJ Am Coll Cardiol2007492151215917543634
- GheorghiadeMOrlandiCBurnettJCRationale and design of the multicenter, randomized, double-blind, placebo-controlled study to evaluate the Efficacy of Vasopressin antagonism in Heart Failure: Outcome Study with Tolvaptan (EVEREST)J Card Fail20051126026915880334
- GheorghiadeMKonstamMABurnettJCJrEfficacy of Vasopressin Antagonism in Heart Failure Outcome Study With Tolvaptan (EVEREST) InvestigatorsShort-term clinical effects of tolvaptan, an oral vasopressin antagonist, in patients hospitalized for heart failure: the EVEREST Clinical Status TrialsJAMA20072971332134317384438
- KonstamMAGheorghiadeMBurnettJCJrEfficacy of Vasopressin Antagonism in Heart Failure Outcome Study With Tolvaptan (EVEREST) InvestigatorsEffects of oral tolvaptan in patients hospitalized for worsening heart failure: the EVEREST Outcome TrialJAMA20072971319133117384437
- SternsRHNigwekarSUHixJKThe treatment of hyponatremiaSemin Nephrol20092928229919523575
- Food and Drug Administration. FDA labeling information FDA web site. http://www.accessdata.fda.gov/drugsatfda_docs/label/2009/022275lbl. Accessed Jan 28, 2009.
- GhaliJKMechanisms, risks, and new treatment options for hyponatremiaCardiology200811114715718434717
- GoldsmithSRTreatment options for hyponatremia in heart failureHeart Fail Rev200914657318777208
- BraterDCDiuretic TherapyN Engl J Med19983393873959691107
- GohKPManagement of hyponatremiaAm Fam Physician2004692387239415168958
- LicataGDi PasqualePParrinelloGEffects of high-dose furosemide and small-volume hypertonic saline solution infusion in comparison with a high dose of furosemide as bolus in refractory congestive heart failure: Long-term effectsAm Heart J200314545946612660669
- Costello-BoerrigterLCSmithWBBoerrigterGVasopressin-2-receptor antagonism augments water excretion without changes in renal hemodynamic or sodium and potassium excretion in human heart failureAm J Physiol Renal Physiol2006290F273F27816189291
- GheorghiadeMGottliebSSUdelsonJETolvaptan InvestigatorsVasopressin V(2) receptor blockade with tolvaptan versus fluid restriction in the treatment of hyponatremiaAm J Cardiol2006971064106716563917
- Food and Drug Administration FDA labeling information. http://www.fda.gov/Drugs/default.htm. Accessed Jan 28, 2009.
- WongFBleiATBlendisLMThuluvathPJA vasopressin receptor antagonist (VPA-985) improves serum sodium concentration in patients with hyponatremia: a multicenter, randomized, placebo controlled trialHepatology20033718219112500203
- AbrahamWTShamshirsazAAMcFannKOrenRMSchrierRWAquaretic effect of lixivaptan, an oral, non-peptide, selective V2 receptor vasopressin antagonist, in New York Heart Association functional class II and III chronic heart failure patientsJ Am Coll Cardiol2006471615162116630999
- THE BALANCE Study: Treatment of Hyponatremia Based on Lixivaptan in NYHA Class III/IV Cardiac Patient Evaluation. http://www.clinicaltrials.gov. Accessed August 12, 2009.
- YatsuTTomuraYTaharaAPharmacological profile of YM087, a novel nonpeptide dual vasopressin V1a and V2 receptor antagonist, in dogsEur J Pharmacol19973212252309063692
- TaharaATomuraYWadaKEffect of YM087, a potent nonpeptide vasopressin antagonist, on vasopressin-induced protein synthesis in neonatal rat cardiomyocyteCardiovasc Res1998381982059683922
- UdelsonJESmithWBHendrixGHAcute hemodynamic effects of conivaptan, a dual V1A and V2 vasopressin receptor antagonist, in patients with advanced heart failureCirculation20011042417242311705818
- GhaliJKKorenMJTaylorJRfor the conivaptan study groupEfficacy and safety of oral conivaptan: A V1a/V2 vasopressin receptor antagonist, in patients with advanced heart failureJ Clin Endocrinol Metab2006912145215216522696
- GoldsmithSRElkayamUHaughtWHBarveAHeWEfficacy and safety of the vasopressin V1A/V2-receptor antagonist conivaptan in acute decompensated heart failure: a dose-ranging pilot studyJ Card Fail20081464164718926434
- TEMPO 3/4 Trial Tolvaptan Efficacy and Safety in Management of Polycystic Kidney Disease and Its Outcomes (TEMPO3/4). http://www.clinicaltrials.gov/ct2/show/NCT00428948?term_TEMPO&rank_1. Accessed February 28, 2008.