Abstract
Objective
To compare the operative outcomes, postoperative pain, and subsequent convalescence after laparoendoscopic single-site surgery (LESS) or conventional laparoscopic surgery for adnexal preservation.
Study design
From December 2009 to September 2010, 63 patients underwent LESS (n = 33) or a conventional laparoscopic surgery (n = 30) for cyst enucleation. The overall operative outcomes including postoperative pain measurement using the visual analog scale (VAS) were evaluated (time points 6, 24, and 24 hours). The convalescence data included data obtained from questionnaires on the need for analgesics and on patient-reported time to recovery end points.
Results
The preoperative characteristics did not significantly differ between the two groups. The postoperative hemoglobin drop was higher in the LESS group than in the conventional laparoscopic surgery group (P = 0.048). Postoperative pain at each VAS time point, oral analgesic requirement, intramuscular analgesic requirement, and the number of days until return to work were similar in both groups.
Conclusion
In adnexa-preserving surgery performed in reproductive-age women, the operative outcomes, including satisfaction of the patients and convalescence after surgery, are comparable for LESS and conventional laparoscopy. LESS may be a feasible and a promising alternative method for scarless abdominal surgery in the treatment of young women with adnexal cysts
Introduction
Recently, the number of laparoendoscopic single-site surgery (LESS) procedures performed has increased because of advancements in surgical instrumentation, cosmetic considerations and trends toward minimal invasiveness.Citation1 The LESS procedure was developed due to the unique characteristics of the umbilicus, ie, it is the thinnest portion of the abdominal wall, does not have a muscle layer, and is naturally retracted. Hence, during the LESS procedure, there may be less tension during wound closure and relatively less scarring in the umbilicus than that in other areas.Citation2
Many studies have been performed on LESS in the gynecologic field, including in gynecologic oncology. The use of LESS has been reported to be feasible and safe for ectopic pregnancy; adnexal surgery, including ovarian cyst enucleation; hysterectomy, including laparoscopic-assisted vaginal hysterectomy and total laparoscopic hysterectomy; and gynecologic malignancies.Citation3–Citation11 However, because few gynecologic studies have compared LESS and conventional laparoscopy, it is unclear whether LESS is truly better than the conventional surgical approach in reducing objective pain, as reflected by the objective pain scores for both procedures.Citation12–Citation15 Reproductive-age women diagnosed with a benign adnexal cyst have usually been treated with cyst enucleation to preserve their fertility. However, in LESS, it can be technically difficult to achieve the optimal traction-countertraction for enucleation and to control the bleeding from various foci. Hence, we designed the present study to specifically investigate differences in the operative outcomes, postoperative pain, and subsequent convalescence after LESS and conventional laparoscopic surgery for unilateral cyst enucleation in reproductive-age women with benign adnexal cysts.
Materials and methods
Our study was a prospective randomized controlled study involving patients who underwent surgical intervention involving LESS or conventional laparoscopic surgery for cyst enucleation of a unilateral benign adnexal mass. The study period was December 2009 to September 2010, and the study involved patients from Cheil General Hospital and Women’s Healthcare Center, Seoul, Korea. During the study period, 80 patients met the inclusion criteria and agreed to be enrolled in the study. Forty patients were alternately assigned to undergo LESS, and 40 were assigned to undergo conventional laparoscopic surgery.
The inclusion criteria were as follows: aged between 18 and 45 years; premenopausal status; presence of a unilateral adnexal mass, the largest diameter of the unilateral adnexal mass ranging between 4 cm and 10 cm in imaging studies; and normal cancer antigen (CA)-125 levels. The exclusion criteria were as follows: evidence of pelvic or ovarian endometriosis; previous history of pelvic inflammatory disease; suspicion of malignancy or pelvic adhesion; and postmenopausal status. To avoid any possible confounder in the quantification of postoperative pain, patients who needed additional wound extension for specimen removal were excluded from the study. In addition, a patient who wanted to postoperatively control her pain with patient-controlled analgesia (PCA) was excluded from the study.
The study protocol was approved by the Institutional Review Board of the Cheil General Hospital and Women’s Healthcare Center. All the patients were adequately informed of the possible risks and benefits of both LESS and conventional laparoscopic surgery. All study participants signed a written consent agreeing to undergo cyst enucleation by LESS or the conventional method and, if necessary, to allow the use of an additional ancillary port during LESS. The patients were randomly assigned to undergo LESS or conventional laparoscopic surgery. Three experienced surgeons (YJ Cho, JM Kim and ML Kim) were involved in the protocol, and in the treatment procedure. At the end of the surgery, intraoperative data such as the trocar-introduction time, operation time, intraoperative and postoperative complications, and number of conversions to laparotomy were recorded. During the convalescence period, oral feeding was started on postoperative day 1. Intramuscular or oral analgesics were provided only on the patient’s request. The visual analog scale (VAS), scored from 0 to 10 (with “0” being “no pain” and “10” being “agonizing pain”) was self-reported at 6, 24, and 48 hours after surgery. Follow-up information about the use of analgesics and patient-reported time to recovery end points were obtained from office visits at 4 weeks after the surgery via a modified questionnaire (Appendix A) that was adapted from those used in a previous study and was administered by the physician members of the research team.Citation16
Statistical analysis was performed with SPSS version 15.0 (SPSS, Inc, Chicago, IL) by using Student’s t-test, Fisher’s exact test, and the Chi-square test. A P-value of less than 0.05 was considered to be statistically significant.
Operative techniques
The patient was placed in the lithotomy position. The surgeon stood on the left side of the patient. The first assistant stood on the right side of the patient to operate the scope. In the case of LESS, the patients underwent surgery through a single 2–2.5 cm vertical umbilical incision, performed via the open Hasson technique. We used a homemade wound retractor and a surgical glove as the single-port device. The distal ring of an Alexis® retractor (Applied Medical, Santa Rancha Margarita, CA) was used as the intra-abdominal portion of a commercialized wound retractor, and it was rolled up with the wrist portion of a powder-free latex surgical glove (GammexPF, 7–0; Ansell Ltd, Victoria, Australia). The multiple fingers of the glove functioned as a multiport for the laparoscopic instruments and the scope.
We used a rigid 0 or 30 degree, 5 mm or 10 mm laparoscope and standard rigid 5 mm laparoscopic instruments. The homemade single-port device was inserted into the umbilicus, and two or three 5 mm sheaths and one 10 mm sheath were inserted through the open fingertip portions of the surgical glove and tied with 6-0 silk ligatures to prevent gas leakage. Next, carbon dioxide was insufflated to maintain intra-abdominal pressure at 12 mmHg. Once the laparoscope and instruments were in place, the subsequent procedure was similar to the one performed in conventional laparoscopic surgery (). Adnexal specimens were extracted with an EndoPouch (Ethicon Endo-Surgery, Cincinnati, OH) via the umbilicus. The peritoneum and fascia were approximated and closed layer by layer with 2-0 Vicryl sutures.
Figure 1 Laparoendoscopic single-site surgery (LESS) for adnexal preservation (intraoperative view).
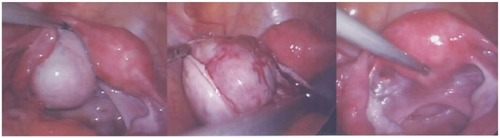
For conventional laparoscopy, the 10 mm laparoscope was introduced into the abdominal cavity through the umbilicus, and three 5 mm accessory trocars were suprapubically inserted under direct vision. All the specimens were extracted using the EndoPouch via the umbilicus under the guidance of a 5 mm laparoscope.
Results
Among the 80 patients selected, 63 were eligible for analysis. In the LESS group, seven patients were excluded because three had deep infiltrating pelvic endometriosis and needed resection of those lesions, one was diagnosed with ovarian endometrioma, one was lost to follow-up, and two needed an additional ancillary port for adhesiolysis and bleeding control. In the conventional laparoscopic surgery group, ten patients were excluded because one had severe pelvic adhesion, six had pelvic and/or ovarian endometriosis, and three had incompletely answered the self-reported questionnaires. These ten excluded patients were successfully treated by the surgical procedure appropriate for their condition. The characteristics of the patients are summarized in . Both the groups were comparable in terms of demographic characteristics and the final pathologic results. The perioperative outcomes are shown in . The mean operation times were 42.1 minutes and 36.3 minutes for the LESS group and conventional laparoscopic surgery group, respectively. No patient from either of the groups required conversion to laparotomy. The mean hemoglobin drop was 2.0 g/dL in the LESS group and was thus higher than that in the conventional laparoscopic surgery group (P = 0.048). However, no patient required a blood transfusion in the study groups.
Table 1 Demographic data of patients
Table 2 Perioperative outcomes of the patients
Postoperative complications occurred in two patients in the LESS group. One patient experienced abdominal distension and pain after oral intake and was diagnosed with paralytic ileus by abdominal radiography. After conservative management, her bowel function was restored spontaneously. Another patient experienced delayed ovarian bleeding from the enucleation site. Her initial hemoglobin level was 13.3 g/dL; at postoperative day 3, her hemoglobin level was 7.5 g/dL. On transvaginal ultrasonography, a 7 cm hematoma was detected at the enucleation site. The patient had no symptoms or signs of acute bleeding and refused transfusion for anemia correction. On a follow-up visit 2 weeks after the surgery, the size of the hematoma had decreased to 5 cm and was found to have completely resolved in 6 weeks after surgery.
The data for postoperative pain, including the VAS score and the use of additional analgesics after surgery, are shown in . There were no statistical differences in the VAS scores obtained at 6, 24, and 48 hours after surgery. Moreover, the mean number of days of oral analgesic use after discharge was only 1.3 days and 0.9 days in the LESS and conventional surgery groups, respectively. There was no difference in the number of days until return to work. The self-reported scar satisfaction scale results were similar for both groups. Most of the patients stated that they would recommend the procedure to a friend or a family member undergoing laparoscopic adnexa-preserving surgery.
Table 3 Pain and convalescent outcomes
Conclusion
Ever since laparoscopic surgery was introduced in the gynecologic field, minimally invasive surgery has steadily evolved toward progressively less invasive techniques. Currently, there is an increasing interest in LESS.Citation17
There are many benefits of LESS as compared to conventional multiport laparoscopic surgery. LESS may result in better cosmesis owing to the relatively hidden umbilical scar, obviation of the use of ancillary ports, and use of the open Hasson technique; therefore, the injury rates by the Verres needle and primary trocar are low. Additionally, inferior epigastric vessel injury, postoperative wound infection, and hernia formation are potentially reduced. Compared to the conventional 5 mm or 11 mm trocar incisions, a relatively large incision on the umbilicus facilitates easier specimen removal.Citation11 Some studies involving retrospective comparsions of hysterectomy have shown that the post-operative pain and narcotic use is less than conventional laparoscopic hysterectomy.Citation13,Citation14 To our knowledge, a prospective study focusing on only cyst enucleation has not yet been published.
At present, several studies have been published regarding LESS treatment of adnexal disease and have shown that the results for LESS are comparable to those for conventional laparoscopic surgery. Most of these studies have compared or listed the perioperative outcomes of adnexal surgery procedures such as salpingo-oophorectomy or salpingectomy.Citation3,Citation6,Citation7,Citation11–Citation13,Citation18–Citation24 However, in our study, we compared the perioperative results including return to work and postoperative satisfaction for LESS and conventional laparoscopic surgery performed only for cyst enucleation in reproductive-age women with unilateral adnexal cysts. As reproductive-age women are concerned about the cosmetic problems clinicians have to consider LESS, but little is known about the safety of adnexa-preserving surgery involving LESS.
One of the current problems with LESS is the crowding of instruments at the point of entry into the abdomen. This problem can be partially offset by using articulating instruments with varying curvatures. In all our procedures, we used only a conventional scope and instruments for LESS. The operative time, complications, and postoperative convalescence were comparable between both groups. However, if there is a concern about the high cost of flexible laparoscopic instruments, we think that conventional instruments, which are cost effective, could be safely used. The use of a 30-degree scope or digital endoscope (Olympus EndoEYE) would eliminate the cumbersome right-angle light pillar and the camera head, thereby minimizing the possibility of crowding at the entry site. Furthermore, its superior digital image quality owing to the 5 mm telescope would provide excellent visualization.Citation25
LESS and conventional laparoscopic surgery were comparable in terms of pain. No statistical differences were observed between VAS scores or the requirement for analgesics (intramuscular or oral) for both groups. In addition, given the aforementioned facts, we used a specific convalescence questionnaire, which was previously used, focused on patient-reported time to specific, easily recalled postoperative events. The patient-reported scar satisfaction scale results were high for both groups, and most of the patients experienced complete recovery and returned to work within 7 days. Although this study was a prospective randomized controlled study, the study population was small. We think that LESS is safe and feasible for women who need adnexapreserving surgery, but we could not find major advantages of this method in terms of early convalescence and postoperative pain. Large prospective randomized studies are required to establish the advantages of adnexa-preserving surgery involving LESS over those of adnexa-preserving surgery involving conventional laparoscopic surgery. However, the postoperative hemoglobin drop was statistically higher in the LESS group (2.0 ± 0.7 g/dL) than in the conventional surgery group (1.7 ± 0.6 g/dL). Conversely, none of the patients required blood transfusion, and we think that this difference in postoperative hemoglobin drop can be reduced if we gain more experience in performing LESS.
To our knowledge, this is the first study involving a prospective comparison between LESS and conventional laparoscopic surgery performed for adnexal preservation. We conclude that performing LESS is safe and feasible in selected female patients diagnosed with a benign adnexal mass requiring fertility-preserving surgery.
Disclosure
The authors report no conflicts of interest in this work.
References
- JeonHGJeongWOhCKInitial experience with 50 laparoendoscopic single site surgeries using a homemade, single port device at a single centerJ Urol201018351866187120303108
- KimTJSingle-port access (SPA) laparoscopic surgeryKorean J Gynecol Endosc Minim Invasive Surg20092112730 Korean
- YoonBSParkHSeongSJParkCTParkSWLeeKJSingle-port laparoscopic salpingectomy for the surgical treatment of ectopic pregnancyJ Minim Invasive Gynecol2010171262919926346
- LimMCKimTJKangSBaeDSParkSYSeoSSEmbryonic natural orifice transluminal endoscopic surgery (E-NOTES) for adnexal tumorsSurg Endosc200923112445244919343442
- KimTJLeeYYKimMJSingle port access laparoscopic adnexal surgeryJ Minim Invasive Gynecol200916561261519835804
- FagottiAFanfaniFRossittoCLaparoendoscopic single-site surgery for the treatment of benign adnexal disease: a prospective trialDiagn Ther Endosc2010201010825820169051
- EscobarPFBedaiwyMAFaderANFalconeTLaparoendoscopic single-site (LESS) surgery in patients with benign adnexal diseaseFertil Steril20109362074.e7e1020100614
- LeeYYKimTJKimCJSingle-port access laparoscopic-assisted vaginal hysterectomy: a novel method with a wound retractor and a gloveJ Minim Invasive Gynecol200916445045319487164
- KoyanagiTMotomuraSTransumbilical single-incision laparoscopic surgery: application to laparoscopically assisted vaginal hysterectomyArch Gynecol Obstet2011283230530920084387
- JungYWKimYTLeeDWThe feasibility of scarless single-port transumbilical total laparoscopic hysterectomy: initial clinical experienceSurg Endosc20102471686189220035346
- FaderANEscobarPFLaparoendoscopic single-site surgery (LESS) in gynecologic oncology: technique and initial reportGynecol Oncol2009114215716119481243
- LeeYYKimTJKimCJSingle port access laparoscopic adnexal surgery versus conventional laparoscopic adnexal surgery: a comparison of perioperative outcomesEur J Obstet Gynecol Reprod Biol2010151218118420392556
- FagottiABattoniCVizzielliGPostoperative pain after conventional laparoscopy and laparoendoscopic single site surgery (LESS) for benign adnexal disease: a randomized trialFertil Steril2011961255259.e221565338
- KimTJLeeYYChaHHSingle-port-access laparoscopic-assisted vaginal hysterectomy versus conventional laparoscopic-assisted vaginal hysterectomy: a comparison of perioperative outcomesSurg Endosc20102492248225220177921
- YimGWJungYWPaekJTransumbilical single-port access versus conventional total laparoscopic hysterectomy: surgical outcomesAm J Obstet Gynecol2010203126.e1e620417481
- CanesDBerqerAAronMLaparoendoscopic single site (LESS) versus standard laparoscopic left donor nephrectomy: matched-pair comparisonEur Urol20105719510119664877
- RamirezPTSingle-port laparoscopic surgery: is a single incision the next frontier in minimally invasive gynecologic surgery?Gynecol Oncol2009114214314419559942
- FagottiAFanfaniFMaroccoFRossittoCGallottaVScambiaGLaparoendoscopic singlesite surgery (LESS) for ovarian cyst enucleation: report of first 3 casesFertil Steril20099231168.e13e1619589520
- EscobarPFFaderANParaisoMFKaoukJHFalconeTRobotic-assisted laparoendoscopic singlesite surgery in gynecology: initial report and techniqueJ Minim Invasive Gynecol200916558959119589731
- EscobarPFStarksDCFaderANBarberMRojas-EspalliatLSingle-port risk-reducing salpingo-oophorectomy with and without hysterectomy: surgical outcomes and learning curve analysisGynecol Oncol20101191434720579712
- FaderANRojas-EspaillatLIbeanuOGrumbineFCEscobarPFLaparoendoscopic single-site surgery (LESS) in gynecology: a multi-institutional evaluationAm J Obstet Gynecol20102035501.e1e620663487
- MaroccoFFanfaniFRossittoCGallottaVScambiaGFagottiALaparoendoscopic single-site surgery for fertility-sparing staging of border line ovarian tumors: initial experienceSurg Laparosc Endosc Percutan Tech2010205e172e17520975495
- FagottiAFanfaniFMaroccoFLaparoendoscopic single-site surgery for the treatment of benign adnexal diseases: a pilot studySurg Endosc20112541215122120872020
- FagottiARossittoCMaroccoFPerioperative outcomes of laparoendoscopic single-site surgery (LESS) Versus conventional laparoscopy for adnexal disease: a case-control studySurg Innov2011181293321245066
- DesaiMMSteinRRaoPEmbryonic natural orifice transumbilical endoscopic surgery (E-NOTES) for advanced reconstruction: initial experienceUrology200973118218718799203
Appendix A
Patient questionnaire
How many days or weeks did you require oral pain killers after being discharged from the hospital?
How many days or weeks before you went back to work after being discharged from the hospital?
How would you rate your surgical scar(s) on a scale of 1–5, with 5 being delighted and 1 being very displeased?
Would you recommend that a friend or family member in a similar situation undergo your procedure? Yes/No.