 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Background and purpose:
Weightbath hydrotraction treatment (WHT) is a simple noninvasive effective method of hydro- or balneotherapy to stretch the spine or lower limbs, applied successfully in hospitals and health resort sanitaria in Hungary for more than fifty years. This study aims to introduce WHT with its biomechanical and clinical effects. History, development, equipment, modes of application, biomechanics, spinal traction forces and elongations, indications and contraindications of WHT are precented.
Subjects and methods:
The calculation of traction forces acting along the spinal column during the treatment is described together with the mode of suspension and the position of extra weight loads applied. The biomechanics of the treatment are completed by in vivo measured elongations of lumbar segments using a special underwater ultrasound measuring method. The clinical effects, indications, and contraindications of the treatment are also presented.
Results:
In the underwater cervical suspension of a human body, approximately 25 N stretching load occurs in the cervical spine, and about 11 N occurs in the lumbar spine. By applying extra weights, the above tensile forces along the spinal column can be increased. Thus, the traction effect can be controlled by applying such loads during the treatment. Elongations of segments L3–L4, L4–L5, and L5–S1 were measured during the usual WHT of patients suspended cervically in water for 20 minutes, loaded by 20–20 N lead weights on the ankles. The mean initial elastic elongations of spinal segments were about 0.8 mm for patients aged under 40 years, 0.5 mm between 40–60 years, and 0.2 mm for patients over 60 years. The mean final viscoelastic elongations were 1.5 mm, 1.2 mm, and 0.6 mm for the same age classes, respectively. No significant difference was found between the sexes regarding age-dependence in tension. WHT for discopathy showed significant improvement of clinical parameters, which was still evident three months later, as demonstrated by using a controlled pilot study.
Conclusion and discussion:
WHT effectively mitigates pain, enhances joint flexibility, and improves the quality of life of patients. The WHT equipment is easy to install and the treatment technique is simple. The authors are the first to determine the biomechanical effects of WHT using an in vivo-measuring method and biomechanical calculations; and verifying the beneficial clinical effects by a controlled pilot study. Approximate values of tensile forces occurring along different points of the spinal column have been calculated, depending on the mode of the suspension, and the value and position of the applied extra weight loads. Time-related viscoelastic elongations of lumbar segments and discs have been measured in vivo, in terms of sex, age, body weight and height and the position of the segment. Several clinical parameters were analyzed by a controlled pilot study to verify the beneficial effects of WHT for cervical and lumbar discopathy. Based on these results, advice can be given to therapists to obtain the optimal traction effects of the treatment.
Introduction
Weightbath hydrotraction therapy (WHT) is a method of hydro- or balneotherapy where the patient is suspended in water, loaded by extra weights applied to certain points of the body, in order to stretch different parts of the spinal column or lower limbs. WHT is an original Hungarian invention introduced by the physician, Károly Moll in the early 1950s.Citation1–Citation3 Hydro- and balneotherapy involves the use of water for soothing pains and treating diseases. Hydrotherapy uses normal tap water. Balneotherapy uses thermal or mineral water.
Water therapies date back to the ancient Egyptian, Greek, and Roman civilizations, for which public baths are well known. Hippocrates prescribed bathing in spring water to treat sickness. This practice was revived by a Dominican monk, Sebastian Kneipp in the 19th century.Citation4,Citation5 Water resort therapy has been very popular in European spas and its use to treat rheumatic diseases has a long history.
Traction methods along the longitudinal axis of the body have been known and used for a significant period of time in medical praxis; even Hippocrates constructed an extension desk for spinal traction. However, what often happens during this treatment is that instead of traction effects and stress relaxation, compression increases in the discs. Indeed, White and PanjabiCitation6 stated that by applying traction to the spine, the discs were put under compression due to muscle activities. Andersson and colleaguesCitation7 concluded that by active traction, in lying posture, the back muscles contracted and the disc pressure increased. Similarly, Ramos and MartinCitation8 verified this inverse relationship between the applied traction load and the intradiscal pressure.
These observations verify the importance of the WHT in which patients are suspended in lukewarm water with relaxed muscles, whereby the contracting effects of the muscles disappear. WHT is an effective noninvasive simple traction method that unloads the compressed discs, increases joint flexibility, extends the height of the discs, decreases discoid bulging, relaxes stress both in the nucleus and in the annulus, unloads nerve roots, relieves pain and may even prevent graver problems as well. In Hungary, WHT has successfully been applied for the last fifty years. The method is applied in all rheumatology hospitals and in health spas as an effective health resort therapy.
However, in spite of the popularity of WHT in Hungary, it is practically unknown elsewhere. Indeed, beside the Hungarian reports related to the weightbath method and to some of the clinical and biomechanical effects,Citation1,Citation3,Citation9–Citation11,Citation13,Citation14,Citation16,Citation17 there have been until recently few published papers in the international literature on this method.Citation2,Citation4,Citation12,Citation15
The verification of the traction effect of WHT has been reported by Kurutz and colleagues,Citation18–Citation20 by measuring the time-related in vivo elongations of lumbar discs and segments in terms of sex, aging, body weight, and height during the treatment. The stress relaxation effect, the disc unloading, and bulging contraction effects of WHT have been verified by numerical simulation for healthy and degenerated discs by Kurutz and Oroszváry. Citation21 The clinical evidence of the efficacy of the treatment has been proved in controlled studies by Oláh and colleagues,Citation5 demonstrating that for patients with cervical and lumbar discopathy the clinical parameters and quality of life improved significantly after WHT.
The goal of this study was to introduce the method to the international public and describe the equipment and the modes of underwater suspension, the biomechanics of the treatment, the subsequent traction loads along the spine and the traction elongations of lumbar segments during the treatment, and its clinical relations, indications, and contra-indications.
The WHT method
WHT equipment
WHT requires a specially designed basin and hanger equipment. The first wooden hanger () was constructed by Moll,Citation1 and was used in the warm thermal lake of Spa Héviz in Hungary. It was later modified by Pap,Citation9,Citation15 and his simple metal equipment, with small modifications, is still used today. It consists of a collar hanger, mounted beneath a steel arch named a ‘lyre’, by which the patient is suspended, together with two armpit support bars ( and ). The steel hanger structure provides elasticity to the whole construction. The plane of the collar, covered by a spongy plastic material, is not perfectly horizontal as it must follow the natural position of the head (). The basin, under the hanger equipment, is especially deepened to guarantee the patient can hang freely.
Figure 1 The first WHT hanger equipment constructed by Moll in 1953.

Figure 2 The WHT equipment consisting of A) the steel arch named “lyre” and two armpit support bars, on which B) the patient is suspended, C) the collar covered by plastic spongy material, and D) the extra lead weights applied on the ankle.
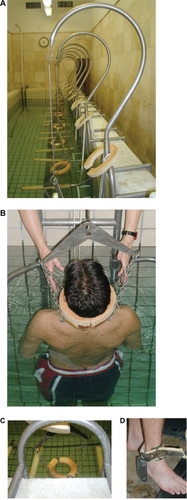
The extension effect can be made more effective by addition of extra weights applied symmetrically, in the plane of the hips, on a waist belt, or alternatively on the ankles ().
WHT application techniques
In WHT, one-, two-, and three-point suspensions are applied as follows. By applying the hanger collar alone, the body is suspended at a single point. By applying the two armpit support bars alone, the body is supported at two points. The combination of the hanger collar with the two armpit support bars represents the three-point suspension.
As a strict rule, the extra weight loads are always placed below the part to be stretched. The therapist must show caution when placing these weights. The special anatomic characteristics of the patient must be taken into consideration regarding the position and measure of the segment to be treated. For example, to stretch the segment, L5–S1, it is important to avoid placing the weights over the plane of the hips as the treatment will be ineffective.
The duration of each treatment is 10–25 minutes, while in duration the total treatment is 2–3 weeks, using daily treatments for both outpatient and inpatient hospital care. At the beginning of the therapy, the treatment time may be 10–12 minutes, which is gradually increased to 20–25 minutes. Experience has shown that extending further the treatment time is ineffective.
WHT biomechanics
WHT traction forces
The traction forces occurring along the spine during WHT were first calculated by Bene and Kurutz.Citation13 During WHT, different tensile forces may occur in different parts of the spinal column depending on the relative density of the human body and the water, the value and position of the applied extra weights, and in particular, the mode of suspension.
The classification of traction loads arises from the definition of traction elongation of spinal segments. Since nobody knows the intact load- and deformation-free state of the spinal segments and discs, a reference state must be chosen. In this way, elongation of spinal segments is specified as an extension compared with the state of the segments in a normal upright standing position just before the traction bath treatment. That is, zero elongation is defined as the compressed reference state of segments just before the treatment.
Obviously, the traction loads are related to the same reference state, ie, the loading process starts from the compressed state before the treatment, by the removal of the body weight and muscle forces in the water. Consequently, there are two components of traction loads: (1) the indirect traction load, that is, the decompressive force consisting of the removal of the compressive preload of body weight and the removal of muscle forces that are partly or totally relaxed during the treatment; and (2) the direct traction load consisting of the active tensile force due to buoyancy and the applied extra loads that are reduced by buoyancy too. Consequently, the traction process in itself can also be divided in an indirect and a direct phase.
Traction forces in one-point suspension
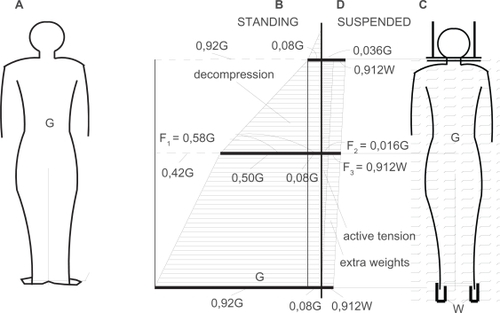
In the case of one-point cervical suspension, the distribution of the indirect and direct traction loads along the spinal column is illustrated in together with the compressive loads of the standing position. Compressive loads of standing are seen to the left (), tensile loads of subaqual suspension are seen to the right (). Since forces always increase towards the support, compressive forces increase downwards the soil support and tensile forces increase upwards towards the hanger collar support. The muscle forces cannot be illustrated.
Figure 3 One-point suspension mode. A) Upright standing position with B) distribution of compressive and decompressive loads along the spinal column; C) cervical suspension in water with D) diagrams of active tensile forces and extra weight loads along the spinal column.
Indirect traction load
In cervical suspension, the first component of the indirect traction load is the removal of the compressive preload acting on the spine before treatment; ie, the net reaction force acting at the analyzed spine level. According to , at lumbar level this force takes about 58%–60% of the body weight G, namely, the weight of the head and trunk together.Citation22 Langrana and colleaguesCitation23 found 0.501G as the net reaction force across the L3 cross-section. In our calculations we used the value of 0.6G for the lower L3–S1 level. This force has to be completed by the removing muscle forces that keep the spine in stable equilibrium in an upright standing position before the treatment. Since cervical suspension provides total muscle relaxation, this force in the lumbar spine can be about the same as the weight of the upper body.Citation24,Citation25 Thus, approximately, the indirect traction load at cervical and lumbar level and at the ankles yield
(1) respectively, since at the cervical level this force consists of the decompression of the head load, and at the ankle level the muscle and tendon forces are high.
Direct traction load
The active tensile force and the extra load depend on buoyancy.Citation13 Bodies in fluid are loaded by the resultant weight of the body acting downwards and the buoyant force acting upwards. Immersed totally in water, the buoyant force Gb of the body is proportional to the ratio of the density of the body ρb and water ρw, that is Gb = G · ρw/ρb. Consequently, the active tensile load for the total body yields G − Gb = G(1 − ρw/ρb). Since the head is not in the water, the weight G has to be reduced by the weight 0.08G of the head, thus, the active tensile load at cervical level, at the collar yields
(2)
In the lumbar level the weight G −0.58G = (1−0.58)G = 0.42G is considered (), thus, the active tensile force at the lumbar level reads:
(3)
By considering ρb = 1040 kg/m3 and ρw = 1000 kg/m3, the above forces read
(4) as seen in . For the standard body weight of G = 700N the cervical and lumbar active tension forces are:
(5) respectively. Due to the buoyancy effect alone, the tensile forces acting on the spinal column of the suspended body in the water are surprisingly small. Caused by the weight of the body, traction forces at the lumbar column are generally insufficient for the required traction effect of the therapy. This experience led to the application of extra weights. Moreover, this effect is even smaller for mineral water, where the water density is higher than that of tap water. At the same time, it may happen that obese patients with smaller density than that of the water start to float.Citation26 Consequently, in such cases the application of extra loads is inevitable. For that very reason, MollCitation1 applied extra lead weights to provoke a more intensive stretching effect. The extra weights W are reduced also by the buoyancy
(6) where the density of lead is ρl = 11350 kg/m3. This force is constant along the total length of the spinal column, as seen in .
As a summary, in the case of one-point suspension with extra loads, the direct traction loads at cervical, lumbar, and ankle levels yield:
(7) respectively, since at ankle level the buoyant force is considered to be zero by neglecting the small buoyant effect of the feet.
Finally, the total traction loads, as the sum of the indirect and direct loads at cervical, lumbar, and ankle levels are
(8) that in the standard case detailed above with 2 × 20 = 40N extra lead loads yield
(9)
From these expressions, the ratio of the decompressive, buoyant, and extra weight loads can be studied.
In the one-point cervical suspension mode, the extra loads can be positioned on other parts of the spine, for example on the waist, when the traction effect of the weights can be calculated over the positioned point, between that point and the collar. If there are no extra weights applied, in the above results W = 0 is considered.
Traction forces in two-point suspension
Occasionally, during WHT, the direct loading of the occipitoatlantal part of the spinal column must partly or totally be avoided. If WHT aims to stretch either the lumbar part of the spinal column or the big joints of the lower limbs, and the concentrated loading of the cervical segments is contraindicated, or simply, being suspended at the occipitoatlantal point is inconvenient for the patient, application of armpit supports may be used. Armpit support represents a two-point suspension.
In contrast to the one-point suspension, using armpit supports, the muscles must be active to keep the body in equilibrium in the water. Consequently, the decompressive effect of the muscles cannot be taken into consideration. Moreover, the weight of the head acts as compression force to the spine. Furthermore, with armpit support, the action lines of tensile forces are disadvantageous with regards to the stretching effect. Namely, in cervical suspension, the collar support, where the forces are concentrated, is very close to the spinal column, therefore the action line of the direct traction forces is close to the spinal column leading to an increased effect of stretching. However, with armpit bars, the action line of the direct traction forces are distributed along the back muscles towards the armpit supports, far away from the spinal column. These hypotheses have to be further researched. Consequently, the traction forces cannot be correctly calculated in this suspension mode.
Traction forces in three-point suspension
The above mentioned analytical problems become more intensive in the case of the three-point suspension where there is a combination of cervical suspension and bilateral armpit bar support. Tensile forces of cervical suspension are highly influenced by the active muscle forces occurring from the bilateral armpit supports. Moreover, the armpit bars are generally applied as conditional supplementary supports only if it is necessary to unload the cervical segments. Regarding the numerical approach, the main problem is that the usage of supplementary armpit supports in itself, depends exclusively on the decision of the patient, and it is continuously changing during the therapy. Thus, during this mode of suspension, all combinations of pure one- and two-point suspension can happen; therefore, an infinite number of arbitrary combinations may occur at irregular time intervals. This makes the analysis very complicated.
At present, the only mechanical consequence which can be drawn for the three-point suspension is that the traction effect in the spinal column is smaller than in the case of pure cervical suspension. This problem needs more experimental and analytical investigation.
WHT traction deformations
Elongations of segments L3–L4, L4–L5, and L5–S1 were measured by Kurutz and colleagues,Citation14,Citation18–Citation20 during normal WHT of patients suspended cervically in lukewarm water for 20 minutes, without extra weights, and loaded by 20 N lead weights on each ankle. WHT is a typical viscoelastic process with initial instant elastic and 20-minute long creeping phases. Thus both the initial elastic and the further creeping elongations were measured by using a special subaqual ultrasound measuring method.Citation19 The extension of the distance between two spinous processes of adjacent vertebrae was measured during the WHT, in special time instants, by a mobile ultrasound instrument. During the measuring process, physicians were in the bath, together with the suspended patient. The ultrasound pictures and measured results were digitally stored and evaluated by using an image analyzer.
At the beginning of the suspension without extra weights, 30%–50% of patients showed instant elastic elongations with a mean value of 0.4–0.6 mm per segment. At the end of the treatment, elongations were observed in 70%–85% of patients in the group with, and 55%–65% in the group without extra weights. The mean additional elongations per segment were approximately 0.2–0.35 mm without, and 0.5 mm with extra weights. The total final elongations were approximately 0.8–0.9 mm and 0.8–1.4 mm without and with extra weights respectively.
In analyzing age-effects, three age-classes were distinguished: young (under 40 years), middle aged (40–60 years) and old (over 60 years). In the group with extra weights, the mean initial/final age-related elongations for less than 40 years, between 40–60 years, and over 60 years were: 0.58/1.50 mm, 0.66/1.51 mm, 0.34/0.96 mm (L3–L4); 0.80/1.41 mm, 0.49/1.19 mm, 0.24/0.36 mm (L4–L5); and 1.06/1.63 mm, 0.24/0.79 mm, 0.07/0.25 mm (L5–S1), respectively. For the group without extra weights these values were 0.42/0.99 mm, 0.50/1.10 mm, 0.07/0.44 mm (L3–L4); 0.86/1.29 mm, 0.41/0.86 mm, 0.15/0.38 mm (L4–L5); and 0.27/0.53 mm, 0.50/0.87 mm, 0.15/0.61 mm (L5–S1), respectively.
For the lumbar segments, L3–S1, the mean initial/final age-related elongations with extra weights for less than 40 years, between 40–60 years, and over 60 years were: 0.82/1.51 mm, 0.48/1.19 mm, 0.23/0.55 mm, respectively.
WHT clinical relations
WHT has been successfully applied for more than fifty years in all spas, rheumatology hospitals, health resort sanatoria, and wellness centers in Hungary. Indications and contraindications of WHT have been developed during this time, based on medical experience only, without any clinical studies. Consequently, most of the indications and contraindications detailed below can be considered only as hypotheses to be verified by medical practice. However, a recent controlled pilot study with follow-up has been reported on the clinical effects of WHT in treating disorders of the cervical and lumbar spine.Citation5
WHT indications and contraindications
WHT can be applied in the active recovering state of acute radiculitis, radiculoneuritis, after commencement of mobilization. Frequently, soon after the beginning of the first treatment, a sudden improvement can be observed.
WHT can be applied with success in treating compensated scoliosis in adults where the problem is secondary discopathy or myalgia. However, for conservative treatment of fixed posture problems or decompensated scoliosis, the decision on treatment must be based on orthopedic consultation, taking into consideration the individual patient, with respect for age and condition.
There is some success in applying WHT for mild osteoporosis if the mobility of the spinal column can be observed in every segment, due to a preceding pharmaceutical treatment and consistently applied physiotherapy.
As a conclusion, indications for the use of WHT are as follows: discopathy (osteochondrosis); spondylosis; spondylarthrosis; cervicobrachialgia; lumboischialgia (subacute, chronic radiculopathia, post-radiculitic neuralgia); neuralgia occipitalis; migraine cervicalis; Morbus Scheuermann; spondylarthritis ankylopoetica states I–II; contracture of hip and knee joints.
Contraindications for the use of WHT are as follows:
General contraindications: if the bath in itself is contraindicated; insuficient coronaria; ischemic heart disease; angina pectoris; hypertonia; hyperthyreosis; asthma bronchiale; emphysema pulmonum gravis; cor. pulmonale chr. decomp.; tumor; tbc.
Local contraindications: acute radiculitis, radiculoneuritis, spondylolysis, spondylolisthesis; spondilitis tbc, aspecifica; tumor vertebrae, status post laminectomiam, and other postoperative states, (status post spondylodesim, screwed osteosynthesis op., Wiltsche op.); inflammation contractions of joints of hip and knee; varicositas cruris gravis; ulcus cruris.
Clinical results of WHT
The clinical results of WHT were initially analyzed by Domokos and SzabóCitation16 in an uncontrolled study of 790 patients. For lumbar discopathy, 50% of the patients recovered, 45% of them showed improvement, and 5% had no change. For degenerative diseases of the cervical segments, WHT was successful in 36%, partly effective in 60% and ineffective in 4% of the patients.
WHT for discopathy achieves significant improvement, mitigates pain and enhances joint flexibility. Oláh and colleaguesCitation5 investigated clinical trials to verify the beneficial impacts of WHT on the clinical parameters and quality of life of patients with cervical and lumbar discopathy. A controlled pilot study with follow-up was investigated on ambulatory patients having cervical or lumbar discopathy, related to several clinical parameters, eg lumbar pain intensity, finger–floor distance, shifting of hand position on the thigh upon lateral flexion of the trunk, neck pain intensity, lateral and dorsal flexion of the cervical spine, SF-36® score, Oswestry index, magnetic resonance imaging changes of intervertebral disc protrusion, patient’s subjective opinion, and physician’s appraisal. WHT for cervical discopathy achieved significant improvement of all studied clinical parameters, which were still evident three months later. In the group with lumbar discopathy, all parameters improved significantly after WHT; the improvement proved to be lasting after three months and increased further in the case of two parameters.
Conclusions
Weightbath therapy aims to treat degenerative diseases of the spinal column and states of contracture in the joints of the lower limbs. The artificially produced permanent or intermittent traction force in the spinal column or in a section of it helps the column to be stretched and elongated longitudinally – which yields the unloading of compressed nerves – leading to the repose of disc prolapses. Although WHT is a successful method in treating low-back pain or discopathy, to increase the efficiency of the treatment, a biomechanical analysis is useful. Namely, for deciding the adequate treatment method depending on the aim of the therapy, the knowledge of the mechanical effects of the therapy itself is necessary.
WHT application aspects
To prescribe any version of WHT, the following factors need to be taken into consideration: the class and type of the rheumatic disease to be treated by WHT; the localization of the disease; the severity and state of the disease; the natural constitution of the individual patient, age, sex, weight, height, muscles, body mass index, general state.
In applying WHT for the required tensile effect, the following possibilities should be considered simultaneously: mode of suspension; the position of the applied extra weights; the amount of the applied extra weights; the time duration of each treatment; and the time duration of the whole cure.
The above detailed analysis should help therapists decide on the optimal form of treatment.
Considering the mode of suspension
By applying one-, two- or three-point suspension, the therapist has to consider that localization of the tensile force can be modified by the mode of suspension.
In one-point suspension, the tensile effect is concentrated at the cervical segments of the spinal column, and the tensile force occurring in the lower segments decreases proportionally in terms of the distance from the support point (). In two-point suspension, the cervical segments are unloaded while the tensile effect is concentrated into the distal segments and the hip joints. The three-point suspension works between the loading–unloading of the cervical segments mutually with the change of loading in the lumbar part of the spinal column due to muscle activation, depending on the self control of the patient.
Considering the extra weights
Generally, for the therapy of cervical segments, self weight of the body in itself may be enough, if the density of the patient is higher than that of the water. In the case of obese patients or using mineral water of a higher density, or, for an effective stretching of the hip or knee joints, extra weights are needed. The required tensile effects are realized by applying them on waist or ankle belts.
In the case of lumbar therapy, for an effective stretching for women of average weight and muscles, 20–20 N, for men of higher weights and muscles, 30–30 N extra lead weights can be applied. The value of weights may also be increased during the therapy.
Interruption of the treatment
During treatment, the patient must not move or stretch their muscles. Patients should be suspended in the lukewarm water tranquilly, in a totally comfortable, relaxed position, almost sleeping with closed eyes. The patient must follow the instructions of the therapist to reach this optimal state.
However, the treatment must be interrupted immediately if the patient cannot tolerate it, or in the case of any sudden effects such as: a feeling of collapse; numbness; dizziness; headache; pain in chest (or elsewhere); or in any change in the normal state of the patient. Most of these problems can be avoided since generally these symptoms are the consequence of the incorrect application of the treatment, or incorrect assessment of the state of the patient. To avoid these problems, the therapist should consider the results of this paper.
Summary
Although WHT is a simple, noninvasive, effective stretching method that has been applied successfully in Hungary for more than fifty years, it is relatively unknown elsewhere. This present study can be used to introduce and familiarize the method to rheumatologists and hydrotherapists anywhere.
The aim of this paper was to give an overview of the treatment with respect to its clinical and biomechanical background, and to give guidance to therapists to avoid complications or the inefficiency of the treatment. On the basis of the above detailed biomechanical results, WHT can be applied more effectively without any risk of side effects or complications.
The authors were the first to determine the traction effects of WHT by using biomechanical calculations and in vivo-measuring methods; and were the first to investigate the clinical evidence of the therapy by using a controlled pilot study. The approximate value of the tensile force occurring in the different points of the spinal column was calculated, depending on the mode of suspension, specific characteristics of the human body, and the value and position of the applied extra weight loads. Several beneficial clinical effects were verified for patients having cervical or lumbar discopathy.
Beside the biomechanical results, the WHT technique and the indications and contraindications of it are also detailed here. Using this paper therapists can obtain a more complete overview of WHT, with important information that can help in consideration of the circumstances for its use, and choosing the optimal mode of the cure.
Acknowledgements
Distinguished thanks are due to head physician É Bene for her professional assistance and advice. Radiologists P Molnár, E Monori and associate professor A Lovas are gratefully acknowledged for their contribution to the experiments. The study was supported by research grants OTKA T-022622, T-033020, T-046755 and K-075018. The authors report no conflicts of interest in this work.
References
- MollKCuring discushernia by so-called “weightbath” therapy. [in Hungarian]Orvosi Hetilap1953421173
- MollKDie Behandlung der Discushernien mit den sogenannten “Gewichtsbadern”Contempl Rheum195697326329
- MollKAbout the new simple medical treatment of discushernia by the so-called “stretch of crutch”. [in Hungarian]Orvosi Hetilap19572053113452521
- BenderTKaragülleZBálintGPGutenbrunnerCBálintPVSukenikSHydrotherapy, balneotherapy, and spa treatment in pain managementRheumatol Int20052522022415257412
- OláhMMolnárLDobaiJOláhCFehérJBenderTThe effects of weightbath traction hydrotherapy as a component of complex physical therapy in disorders of the cervical and lumbar spine: a controlled pilot study with follow-upRheumatol Int20082874975618193231
- WhiteAAPanjabiMMClinical Biomechanics of the SpinePhiladelphia, PALippincott Williams & Wilkins1990722
- AnderssonGBSchultzABNachemsonALIntervertebral disc pressures during tractionScand J Rehabil Med Suppl1983988916585945
- RamosGMartinWEffects of vertebral axial decompression on intradiscal pressureJ Neurosurg1994813503538057141
- PapKLyre of vibration – weightbath therapy. [in Hungarian]Orvosi Hetilap19611884213732581
- KeresztiGThe Barré-Léon syndrome activated due to weightbath and Glisson suspension therapy. [in Hungarian]Rheumatology, Balneology, Allergy1964532
- BozsókiSIrányiJPhysiotherapia. [in Hungarian]Budapest, HungaryMedicina1976
- BeneÉDas GewichtbadZeitschrift für Physikalische Medizin, Balneologie, medizinische Klimatologie1988176771
- BeneÉKurutzMWeightbath therapy and its biomechanics. [in Hungarian]Med J Orvosi Hetilap199313411211123
- KurutzMBeneÉLovasAMolnárPMonoriEElongations of lumbar spine segments, measured in vivo during weightbath treatment. [in Hungarian]Orvosi Hetilap200214367368411975045
- PapKVibrations – Lyre – Gewichtsbad zur Behandlung der Spondylosen und DiscopathienBeitr zur Orthop und Traumat1961 H. 2.
- DomonkosJSzabóZSWeightbath therapy in the medical bath in Szeged. [in Hungarian]Rheumatology, Balneology, Allergy196347
- GömörBBálintGRheumatology. [in Hungarian]Budapest, HungaryMedicina1989
- KurutzMBeneÉLovasAIn vivo deformability of human lumbar spine segments in pure centric tension, measured during traction bath therapyActa Bioeng Biomech200356792
- KurutzMAge-sensitivity of time-related in vivo deformability of human lumbar motion segments and discs in pure centric tensionJ Biomech20063914715716271599
- KurutzMIn vivo age- and sex-related creep of human lumbar motion segments and discs in pure centric tensionJ Biomech2006391180119015925372
- KurutzMOroszváryLFinite element analysis of weightbath hydrotraction treatment of degenerated lumbar spine segments in elastic phaseJ Biomechanics2009433433441
- BartonJBasic Biomechanics for Medical High Schools. [In Hungarian]Budapest, HungaryTextbook Edition1994240
- LangranaNAEdwardsWTSharmaMBiomechanical analyses of loads on the lumbar spineWieselSWWeinsteinJNHerkowitzHDvorakJBellGThe Lumbar SpinePhiladelphia, PAW.B. Saunders Company1996163181
- NachemsonALDisc pressure measurementsSpine1981693977209680
- SatoKKikuchiSYonezawaTIn vivo intradiscal pressure measurement in healthy individuals and in patients with ongoing back problemsSpine1999242468247410626309
- VeghGCervical traction forces by in vivo experiments in weight-bath therapyEsztergom, Hungary: Conference of Hungarian Society of BalneologyNovember 16–18, 2007