Abstract
Purpose:
To study the prescription of oral analgesics for musculoskeletal pain by primary care physicians over a 5-year period in Sweden.
Design:
A retrospective automatic database review of patient records at four primary health care centers. All prescriptions of NSAIDs, weak opioids, and coprescriptions of gastroprotecting medications to patients with musculoskeletal were retrieved for the period January 1, 2004 to November 11, 2008.
Results:
A total of 27,067 prescriptions prescribed to 23,457 patients with musculoskeletal pain were analyzed. Of all prescriptions, NSAIDs were the most commonly prescribed analgesic comprising 79%, tramadol was the second most commonly prescribed analgesic comprising 9%, codeine the third most (7%), and dextropropoxyphene the fourth (5%). The proportion of NSAIDs and weak opioids and the proportion of the different weak opioids prescribed showed no change over time. The proportion of nonselective and selective NSAIDs prescribed changed; Coxib prescriptions decreased from 9% to 4% of all analgesics prescribed in 2004–2007 with no change in 2008.
Conclusion:
NSAIDs were found to be the dominant class of analgesic prescribed by primary care physicians to patients diagnosed as musculoskeletal pain. No change was observed in the proportion of NSAID and weak opioid prescription over the period studied. Prescription of selective Coxibs decreased and was less than 4% in 2008. The impact on gastrointestinal and cardiovascular adverse effects associated with the extensive prescription of NSAIDS for musculoskeletal pain warrants further analysis.
Introduction
Musculoskeletal pain is one of the most common complaints seen by primary care physicians.Citation1 Pain therapy consists of nonpharmacological and pharmacological parts.Citation2 The nonsteroidal anti-inflammatory agents (NSAIDs) have become increasingly popular as a second-line therapy.Citation3–Citation5 Today, there are a variety of NSAIDs available for prescription: traditional nonselective (tNSAIDs), and the more selective COX-II-inhibitors (Coxibs). The analgesic effects of the different NSAIDs are more or less identical; however, the Coxibs are associated with a lower risk for upper gastrointestinal side effects.Citation6 Thus, the Coxibs after their introduction become an alternative to traditional NSAIDs in patients exhibiting risk for upper gastrointestinal bleeding. The national pain guidelines provided by the Swedish Council on Technology Assessment in Health Care supports prescription of Coxibs as a cost-effective option in patients with a gastrointestinal risk.Citation2–Citation4
There is still a need for individual analysis regarding the risk of side effects including not only the upper but the entire gastrointestinal tract and the cardiovascular system.Citation7–Citation11 The long-term use of NSAIDs warrants, however, an in-depth analysis of benefit vs risk on an individual basis.
The aim of this present study was to review the prescription pattern of NSAID and weak opioid analgesics for the treatment of musculoskeletal pain by primary care physicians over a 5-year period with a focus on whether any changes could be detected due to the increasing awareness of the risk for gastrointestinal and cardiovascular risks associated with the long-term systemic use of anti-inflammatory drugs.
Study design
The study protocol was reviewed and approved by the local ethical review board. A retrospective, patient record analysis was performed by a specially designed database tool that automatically reviews the records searching for all diagnostic codes of musculoskeletal pain (ICD-10 codes) and prescriptions codes (ATC-codes) for NSAIDs (nonselective and selective Coxibs) and weak opioids (tramadol, codeine, and dextropropoxyphene) were collected and analyzed. The case records for all patients seen by one of general practitioners, primary care physician, working at four major primary care centers in the Stockholm area, primary care centers of Eriksberg, Curera Söder, Österåker, and Skogås, were reviewed from January 1, 2004 through November 11, 2008.
All data were collected and stored in an anonymous database without any coupling to the individual patient; no further patient details were compiled or stored.
Statistics
Prescription pattern is presented in absolute numbers and proportion of prescriptions made.
The data are presented for the entire cohort; all prescriptions and patients are further separated into adult patients aged 18–65 years and elderly patients older than 65 years.
Post hoc analysis of annual proportion of prescriptions data was analyzed by Chi-square test; a P < 0.05 was considered statistically significant.
Results
A total of 27,067 prescriptions prescribed to 13,641 females (58%) and 9,906 males (42%) diagnosed as musculoskeletal pain were reviewed. On the basis of age, 20,800 prescriptions were made to adult patients and 6,267 to elderly patients.
Patients’ demographics are presented in .
Table 1 Demographics for the entire cohort studied from January 1, 2004 to November 11, 2008
There were no major differences in patient demographics or prescription routines between the four primary health care centers studied.
The entire cohort
NSAIDs were most commonly prescribed analgesic (79%–80%) without any change in proportion of prescription over the 5-year period studied. Tramadol was the second most (9%) of all analgesics prescribed and comprised 45% of weak opioid prescriptions without any change over time (44%–46%). Codeine, dextropropoxyphene, and selective Coxibs were prescribed in 7%, 5%, and 4% of all prescriptions analyzed ().
Table 2 Annual numbers of prescriptions for the entire patient cohort studied
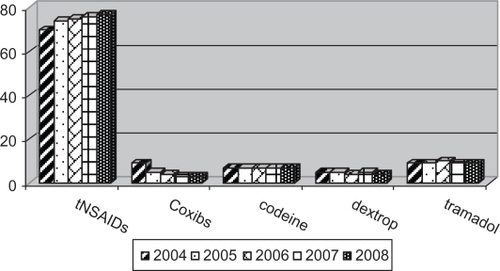
The proportion of NSAID and weak opioid prescriptions in the entire cohort studied did not change during the study period. Prescription of Coxibs decreased, however, between 2004 and 2007 (11.5%–3.8%, P < 0.01) with no further change in 2007–2008 (3.9% of all NSAIDs prescribed). A small reduction in dextropropoxyphene prescriptions was seen: 23%–19% of weak opioid from 2004 to 2008. Annual numbers of prescriptions are presented in and the proportion of prescriptions annually is shown in .
Figure 1 Proportion of prescriptions from 2004 to 2008 for the entire cohort studied.
Separation of prescription data into adults and elderly patients
When the prescription data were separated for adult patients and elderly patients, different prescription patterns were observed. NSAIDs were more commonly prescribed to adults compared with elderly patients and weak opioids more commonly to elderly patients (P < 0.05; ). The proportion of Coxib out of all NSAIDs prescribed was higher among elderly 7% vs 3% (P < 0.05; see ).
Table 3 Proportion of NSAID and weak opioid prescription among entire cohort and when divided into adults and elderly for the 5-year study period
Table 4 Proportion of prescriptions in adult patients and elderly patients over the 5 year period studied
Prescription of dextropropoxyphene showed no change among adults but decreased among elderly, compensated by an increase in tramadol prescription ().
Discussion
Principal findings
We found NSAIDs to be commonly prescribed for musculoskeletal pain, and the proportion of NSAIDs and weak opioids prescribed did not change during the 5-year study (2004–2008). The relative proportion of traditional, nonselective NSAIDs and Coxibs prescribed did, however, change: the prescription of traditional nonselective NSAIDs increased and selective Coxibs decreased during the first 4 years studied but with no change during 2007–2008. Prescription of weak opioids was in general more common among elderly; however, in this more vulnerable patient cohort, no major change in the proportion of NSAIDs and weak opioids was noticed over the time period studied.
Strengths and weaknesses of the study
The aim of the present survey was to study the prescription pattern of NSAIDs and weak opioids to patients with musculoskeletal pain by primary care physicians. A group of patients commonly seen and where the prescription should be considered not only taking the analgesic effect but also the risks for side effects and health economy into account.Citation12 By the automatic data case record review technique used, a huge number of prescriptions could be analyzed. The prescription pattern was seemingly similar between the four health care centers studied, presenting both urban and suburban environments. It should be acknowledged that no intervention was done; all data were collected retrospectively by an automatic review of patient data records, and thus no doctor bias can by any means be expected. The pattern observed should reasonably present a balanced view of clinical routine prescription practice. The study design carries however limitations. The information retrieved included merely prescription information, and no information of comorbidity, concomitant medications, or occurrence of side effects was unfortunately collected. The data retrieved consists only of prescribed medication by ATC code. We have no data about incidence and severity of any side effects, need for extra/emergent health care center consultations, and visits to the emergency department or admission to hospital.
Our findings may not be seen as unexpected. NSAIDs have become the mainstay of therapy for acute musculoskeletal pain.Citation2,Citation3 NSAIDs are also commonly recommended as second-line therapy for pain associated with arthritis when paracetamol has been tested or is unable to provide adequate pain control.Citation2–Citation4 One should, however, acknowledge that we studied primary care physicians and musculoskeletal pain, in general, and not firmly defined diagnosis of arthrosis or arthritis. Similar studies about prescription pattern for musculoskeletal pain made in the United States and Finland (published in 2001 and 2004) showed variability in prescription routines.Citation13,Citation14 Also the findings in a Norwegian survey showed huge variability in patient intake of analgesics for musculoskeletal pain.Citation15 These studies describe prescription of NSAID systemic, as well as topical, weak opioids, and also occasionally stronger opioids. The option for over-the-counter (OTC) medication should also be acknowledged.Citation16 We did not retrieve anamnestic information, and we are, thus, not able to state to what extent our patients used OTC drugs. A more recent American survey showed similar findings to ours, ie, a common prescription routine of NSAIDs,Citation17 and the proportion of Coxibs prescribed changed with a peak in 2001–2003 followed by a dramatic reduction during 2004. The Vioxx and Bextra retractions following identification of an increased incidence of cardiovascular event in 2004 and 2005 caused a major change in the willingness to prescribe Coxibs.Citation9,Citation10 Our findings with respect to NSAID use is similar to that found in a nationwide study in Denmark describing the annual NSAID market.Citation18 The use of NSAIDs is supported by many national guidelines and international reviews, but the awareness of the risk for side effects associated with NSAIDs and the selective Coxibs have promoted a focus on paracetamol as the baseline drug and provided the option for addition of weak opioids when greater analgesia is desired.Citation19
The prescription pattern and compliance to prescribed medication are intrigues parts of the pharmacological management especially in more protracted pain, “chronic pain situations” such as musculoskeletal pain including arthrosis/arthritis. The benefit from the analgesics, reduction of pain, must be evaluated against the risk for side effects in each individual patient.Citation20 Cost is also becoming increasingly important, and in many countries, cheapest generic product is recommended in order to reduce direct drug costs. Cost considerations should, however, take into account not only the direct prescribed drug cost but also costs associated with coprescriptions in order to prevent or treat side effects and other resources needed, ie, any additional contacts with health care.Citation21 We found a clear switch, increase in prescription of nonselective NSAIDs and a reduction in prescription of Coxibs. The impact of this change needs further attention. The option of paracetamol, topical NSAIDs, and addition of low-dose strong opioid when needed should be considered an alternative.
Unanswered questions and future research
The aim of the present study was to review prescription pattern and changes over time. Information about dose, dosing, and compliance to prescription was not analyzed. No outcome variables were included; thus, it is not possible to make any assessment of risk vs benefit from the prescribed medications. The risk for gastrointestinal events associated with NASID use is well recognized. The Coxibs were introduced in order to reduce the gastrointestinal risk and the clinical benefit has been well documented.Citation6 The beneficial effects with regard to upper gastrointestinal events with the Coxib must, of course, be put into the perspective of the cardiovascular risks. It is, however, becoming increasingly obvious that the cardiovascular risk is not class related but differs between the different substances.Citation22,Citation23 Further studies analyzing the overall benefit vs risk and pain reduction, incidence and severity of any gastrointestinal and cardiovascular side effects associated with the change in the prescription ratio of traditional NSAIDs (with and without coprescribed gastroprotection) and Coxibs are warranted.
Summary and conclusion
Anti-inflammatory agents, NSAIDs, were by far the most commonly prescribed analgesic by family physicians for the treatment of musculoskeletal pain. Prescription of Coxibs decreased, however, from 2004 and is only prescribed to a low percentage (<4%). The overall proportion between weak opioids (tramadol, codeine, and dextropropoxyphene) and NSAIDs or the relative proportion of the different weak opioids did not change. Studies evaluating the impact of this extensive use of NSAIDs on the upper gastrointestinal, as well as lower, and cardiovascular side effects are thus warranted.
Acknowledgements
This study has been supported by grants from MSD. All authors have contributed equally in the preparation of this manuscript.
Disclosure
None of the authors have any competing interests.
References
- HasselströmJLiu-PalmgrenJRasjö-WrååkGPrevalence of pain in general practiceEur J Pain20026537538512160512
- ZhangWMoskowitzRWNukiGOARSI recommendations for the management of hip and knee osteoarthritis, part I: critical appraisal of existing treatment guidelines and systematic review of current research evidenceOsteoarthritis Cartilage2007159981100017719803
- ZhangWMoskowitzRWNukiGOARSI recommendations for the management of hip and knee osteoarthritis, Part II: OARSI evidence-based, expert consensus guidelinesOsteoarthritis Cartilage200816213716218279766
- WeaverALCurrent and emerging treatments for mild/moderate acute ambulatory painAm J Ther200815Suppl 10S12S1619127123
- FendrickAMGreenbergBPA review of the benefits and risks of nonsteroidal anti-inflammatory drugs in the management of mild-to-moderate osteoarthritisOsteopath Med Prim Care20093119126235
- HuntRHHarperSWatsonDJThe gastrointestinal safety of the COX-2 selective inhibitor etoricoxib assessed by both endoscopy and analysis of upper gastrointestinal eventsAm J Gastroenterol20039881725173312907325
- BardouMBarkunANPreventing the gastrointestinal adverse effects of nonsteroidal anti-inflammatory drugs: from risk factor identification to risk factor interventionJoint Bone Spine201077161220022539
- LanasASopeñaFNonsteroidal anti-inflammatory drugs and lower gastrointestinal complicationsGastroenterol Clin North Am200938233335219446262
- AlacquaMTrifiròGCavagnaLPrescribing pattern of drugs in the treatment of osteoarthritis in Italian general practice: the effect of rofecoxib withdrawalArthritis Rheum200859456857418383398
- BarozziNTettSEWhat happened to the prescribing of other COX-2 inhibitors, paracetamol and non-steroidal anti-inflammatory drugs when rofecoxib was withdrawn in Australia?Pharmacoepidemiol Drug Saf200716111184119117636557
- GreenbergJDFisherMCKremerJThe COX-2 inhibitor market withdrawals and prescribing patterns by rheumatologists in patients with gastrointestinal and cardiovascular riskClin Exp Rheumatol200927339540119604430
- DrummondMFerrazMBMasonJAssessing the cost effectiveness of NSAID: an international perspectiveJ Rheumatol1995227140814117562786
- MäntyselkäPAhonenRKumpusaloETakalaJVariability in prescribing for musculoskeletal pain in Finnish primary health carePharm World Sci200123623223611826513
- Caudill-SlosbergMASchwartzLMWoloshinSOffice visits and analgesic prescriptions for musculoskeletal pain in US: 1980 vs 2000Pain2004109351451915157714
- HoltedahlRAnalgesics use in patients with chronic musculoskeletal complaintsTidsskr Nor Laegeforen2004124151930193215306862
- MäntyselkäPAhonenRViinamäkiHTakalaJKumpusaloEDrug use by patients visiting primary care physicians due to nonacute musculoskeletal painEur J Pharm Sci2002174–520120612453609
- WilsonRDAnalgesic prescribing for musculoskeletal complaints in the ambulatory care setting after the introduction and withdrawal of cyclooxygenase-2 inhibitorsArch Phys Med Rehabil20099041147115119577028
- FosbølELGislasonGHJacobsenSThe pattern of use of non-steroidal anti-inflammatory drugs (NSAIDs) from 1997 to 2005: a nationwide study on 4.6 million peoplePharmacoepidemiol Drug Saf200817882283318383428
- SchnitzerTJUpdate on guidelines for the treatment of chronic musculoskeletal painClin Rheumatol200625Suppl 1S22S2916741783
- PatrignaniPTacconelliSCaponeMLRisk management profile of etoricoxib: an example of personalized medicineTher Clin Risk Manag20084598399719209280
- HurCChanATTramontanoACGazelleGSCoxibs versus combination NSAID and PPI therapy for chronic pain: an exploration of the risks, benefits, and costsAnn Pharmacother20064061052106316720709
- CombeBSwergoldGMcLayJCardiovascular safety and gastrointestinal tolerability of etoricoxib vs diclofenac in a randomized controlled clinical trial (The MEDAL study)Rheumatology200948442543219223284
- FarkouhMEGreenbergBPAn evidence-based review of the cardiovascular risks of nonsteroidal anti-inflammatory drugsAm J Cardiol20091031227123719406264