Abstract
Aim
Previous systematic reviews have found hydrotherapy to be an effective management strategy for fibromyalgia syndrome (FMS). The aim of this systematic review was to summarize the components of hydrotherapy programs used in randomized controlled trials.
Method
A systematic review of randomized controlled trials was conducted. Only trials that have reported significant FMS-related outcomes were included. Data relating to the components of hydrotherapy programs (exercise type, duration, frequency and intensity, environmental factors, and service delivery) were analyzed.
Results
Eleven randomized controlled trials were included in this review. Overall, the quality of trials was good. Aerobic exercise featured in all 11 trials and the majority of hydrotherapy programs included either a strengthening or flexibility component. Great variability was noted in both the environmental components of hydrotherapy programs and service delivery.
Conclusions
Aerobic exercise, warm up and cool-down periods and relaxation exercises are common features of hydrotherapy programs that report significant FMS-related outcomes. Treatment duration of 60 minutes, frequency of three sessions per week and an intensity equivalent to 60%–80% maximum heart rate were the most commonly reported exercise components. Exercise appears to be the most important component of an effective hydrotherapy program for FMS, particularly when considering mental health-related outcomes.
Introduction
Fibromyalgia syndrome (FMS) is a common condition characterized by widespread musculoskeletal pain and tenderness. It is frequently associated with other symptoms such as feelings of stiffness, loss of sleep, fatigue, depression, and anxiety.Citation1
Treatments for FMS have been evaluated extensively in the literature over the last two decades. A number of systematic reviews have evaluated the effectiveness of exercise for FMS.Citation2–Citation6 All have found evidence to support the use of exercise, in particular aerobic exercise, in the management of FMS. A recent Cochrane review concluded that moderate intensity aerobic training for 12 weeks may improve overall well-being and physical function in FMS.Citation2
Recently, a number of trials and systematic reviews have evaluated the effectiveness of structured exercise programs in warm water (such as hydrotherapy) for FMS. The findings of these trials and systematic reviews suggest that these programs are also effective in the management of FMS, over a range of outcomes. A recent systematic review concluded that there is strong evidence for the use of hydrotherapy in the management of FMS.Citation7
Despite a large volume of research evidence supporting the use of hydrotherapy in the management of FMS, there has not yet been a systematic review which summarizes the components (type of exercise frequency, intensity, duration) of an effective hydrotherapy program for FMS. The aim of this systematic review is to summarize these components, using only randomized controlled trials that have reported significant FMS-related outcomes. This approach may provide clinicians and researchers with a framework for the design of hydrotherapy programs for FMS.
Methods
Search strategy
The following medical and allied heath-related databases were searched systematically by two independent reviewers in May 2009: AMED, MEDLINE, CINAHL, Embase, PubMed, SPORTSDiscus, Scopus, Physiotherapy Evidence Database (PEDro), and Cochrane Controlled Trials Register. The following search terms were used with appropriate truncations; fibromyalgia, hydrotherapy, ‘aquatic therapy’, ‘aquatic exercise’, ‘aquatic physiotherapy’, balneotherapy, thalassotherapy, physiotherapy, ‘physical therapy’, ‘spa therapy’, exercise, water, and pool. The search was limited to randomized controlled trials published in peer-reviewed journals from 1998 onwards in the English language.
Inclusion and exclusion criteria
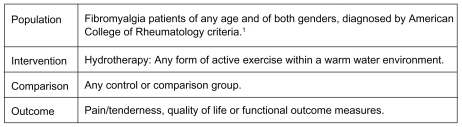
After full text versions of trials were sourced, two authors (LP & ZM) met to discuss their suitability for inclusion. The PICO framework was used to evaluate the suitability of trials for inclusion. PICO (an acronym for population, intervention, comparison and outcome) provides a framework for answering a clinical question.Citation8 Trials that did not fit PICO criteria or did not provide sufficient detail about the components of their hydrotherapy intervention were excluded. The PICO format used in this review is outlined in .
Figure 1 PICO criteria.
Quality appraisal
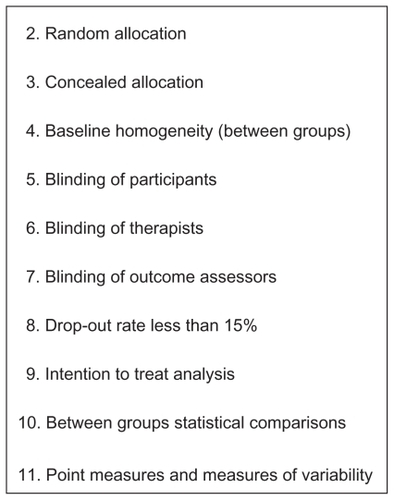
The methodological evaluation of included trials was conducted using the PEDro scale, an 11-point scale which addresses external and internal validity. The first criterion evaluates external validity and is not considered as part of the overall scoring. Criteria 2–11 address internal validity which contribute to an overall score out of 10.Citation9 Three of the items included in the PEDro scale have been demonstrated to be predictive of systematic error or bias in randomized trials (lack of concealment of allocation, blinding and loss of participants at follow up).Citation10 The PEDro scale was chosen for this review because of its capacity to detect these potential sources of biases. Critical appraisal of each study was conducted by two independent reviewers (LP & ZM), who met to discuss any variances in scores until consensus was achieved. The 10 PEDro criteria are outlined in .
Figure 2 PEDro criteria.
Data extraction and analysis
Data relating to the components of hydrotherapy interventions were extracted in four main categories:
Exercise components
Type of exercise (aerobic, strengthening, flexibility, relaxation, warm up and cool down), duration of each hydrotherapy session in minutes and program in weeks, frequency of sessions per week, intensity of exercises as reported in trials and method of progression of exercise.
Environmental components
Equipment used and location of the hydrotherapy intervention.
Service delivery components
Co-interventions, nature of supervision (credentials of those supervising the hydrotherapy) and delivery format (group or individual format).
Outcome measures
Data relating to the outcomes of hydrotherapy interventions were extracted and organized into three categories; pain or tenderness, quality of life and function. Dichotomous outcomes were reported for each of these categories (significant or nonsignificant between group findings).
Definitions
Hydrotherapy was defined as having two important elements: warm water immersion and exercise.Citation11 For the purpose of this review, warm water was defined as a temperature over 30 degrees Celsius, or when water temperature was reported as warm in the trial. Exercise was further defined as active exercise, consisting of contraction and relaxation of one or more muscle groups in a structured and organized manner. Trials using warm water immersion without exercise were excluded.
The intensity of aerobic exercise is often measured as a percentage of maximal heart rate (% HRmax) or percentage of heart rate reserve.Citation12 Intensity can also be measured as a percentage of an individual’s maximal effort, determined by their perceived level of exertion using the Borg Scale, a convenient and valid measure of exercise intensity for aerobic exercise.Citation13 The original Borg scale rates exertion on a 15-point scale from 6 to 20 and assumes a linear relationship to maximum heart rate.Citation13
Other terminology and definitions
Thalassotherapy has been described as a combination of bathing in sea water in a marine climate with solar radiation.Citation14 Thalassotherapy itself does not include exercise, but is frequently combined with exercise. Balneotherapy is term derived from the Latin word balneum which means bath.Citation15 Like thalassotherapy, balneotherapy involves bathing in mineral or thermal water, and can also involve an exercise component. Trials investigating the effectiveness of thalassotherapy and balneotherapy were only included in this review if they involved an exercise component.
Results
Included and excluded trials
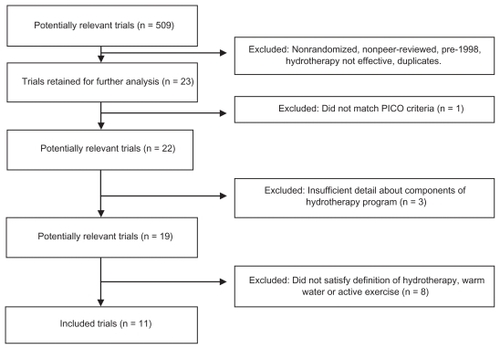
Eleven randomized controlled trials were included in this review. The article by Gowans and colleagues reported on data from their 2001 trial. Six of the 11 trials were published between 2006 and 2009, which may reflect an increasing interest in this area of research in recent years. provides an overview of included and excluded trials.
Figure 3 Included and excluded trials.
Quality of trials
Overall, the trials included in this systematic review were of a good quality. PEDro critical appraisal scores ranged from fiveCitation16–Citation18 to eight.Citation19,Citation20 The majority of trials did not use an intention to treat analysis, which could potentially reduce the validity of their results. However, only one trial reported a drop out rate of over 15%.Citation14 Individual PEDro criterion scores are listed in .
Table 1 Individual PEDro criteria
Exercise components
Type of hydrotherapy program
All 11 trials utilized a warm up, cool down or relaxation period in their hydrotherapy program. In addition, all trials included some form of aerobic exercise. Aerobic exercise included deep water running, active movement of joints against the resistance of the water, jumping, jogging, dancing and low intensity resistance exercises using floatation equipment. Only one trial did not include either a strengthening or flexibility component in their program.Citation20 One trial included both a strengthening and flexibility component and the remaining nine trials used either a strengthening or a flexibility component, but not both.Citation21 This may indicate that strengthening and/or flexibility exercises are important components of hydrotherapy programs for FMS. summarizes the type of hydrotherapy intervention used in each trial.
Table 2 Hydrotherapy interventions
Duration of hydrotherapy programs
Hydrotherapy program duration ranged from 30 to 60 minutes per session. Seven of the 11 trials used a 60 minute session duration and four trials used either 30 or 35 minutes. In contrast, there was great variability in the total duration of programs, ranging from four to 32 weeks (refer to ). Consistently, trials did not report a rationale for the duration of hydrotherapy sessions or the duration of their overall hydrotherapy program.
Table 3 Components of interventions
Frequency of hydrotherapy programs
Frequency of programs ranged from two to four times per week. The majority of trials used a frequency of three times per week. Two trials used a frequency of twice per week and one trial used a frequency of four times per week (refer to ). No trial provided an evidence-based justification for the frequency of their hydrotherapy program.
Intensity of hydrotherapy programs
The intensity of aerobic exercise was reported in eight of the 11 trials Seven of these trials used a percentage of their subject’s maximum heart rate and one trial used their subject’s rating of perceived exertion on the Borg scale (refer to ).Citation10,Citation11 The range of exercise intensity used in trials was from 60%–80% HRmax.
Method of progression of hydrotherapy programs
Only three trials increased the difficulty of exercise as their participants improved. All three of these trials progressed their programs by increasing exercise intensity (refer to ).
Environmental components
Most of the trials included in this review used a pool environment. One trial was conducted in the sea.Citation14 Seven trials used equipment, either heart rate monitors or flotation devices to provide flotation or resistance to movement.Citation14,Citation17–Citation22 Of the 11 trials, only one described the mineral or chemical content of the water.Citation23
Service delivery components
Five trials used either education or land-based exercise as a co-interventionCitation26,Citation21,Citation23–Citation26 No other co-interventions were reported in trials. All trials reported supervising their hydrotherapy program. Only five trials reported the credentials of the person supervising their program and all five of these trials were supervised by a physiotherapist (physical therapist).Citation14,Citation16,Citation19,Citation21,Citation23 All trials used a group hydrotherapy format.
Outcome measures
In accordance with the inclusion criteria of this systematic review, all 11 trials reported statistically significant outcomes in favor of hydrotherapy, either as a between-group measure or as a pre-post measure. Nine trials reported significant between-group measures for one of the following outcomes: pain/tenderness, quality of life, or function.Citation14,Citation16–Citation18,Citation20,Citation22,Citation24–Citation26 Seven trials included a follow up period, most commonly after a de-training period or a period of no intervention.Citation16–Citation18,Citation21,Citation23,Citation24,Citation26 The outcome measures used to determine the effectiveness of hydrotherapy in each trial are summarized in . Between-groups measures are delineated from pre–post measures.
Table 4 Outcome measures and follow up periods
Trends in outcomes
In accordance with the inclusion criteria for this systematic review, all included trials reported significant physical FMS-related outcomes. However, 10 out of 11 trials also reported significant mental health outcomes (depression or anxiety), as either a subscale of a health-related quality of life outcome measure or as a depression or anxiety orientated outcome measure. Three trials reported significant pre–post mental health outcomes following treatment or at follow upCitation16,Citation21,Citation26 Six trials reported significant between-group outcomes immediately following their intervention phase.Citation14,Citation18–Citation20,Citation22,Citation25 The remaining two trials reported significant between-group mental health outcomes at both the end of their intervention phase and after a follow up period.Citation17,Citation23
Seven of the 11 trials reported more than one statistically significant outcome (between-groups), but all seven of these trials used a nonintervention comparison group (refer to ). Four of the five trials that reported more than one significant outcome (pre–post) used an exercise-based comparison group (land-based, home-based or water-based exercise). The remaining trial compared hydrotherapy to balneotherapy without exercise.
Discussion
The effectiveness of various forms of hydrotherapy in the management of FMS has been established in recent years through a number of randomized controlled trials and systematic reviews. This systematic review aimed to summarize the components of randomized controlled trials that have reported significant FMS-related outcomes. Clinicians seeking to design evidence-based hydrotherapy programs for FMS could be guided by the findings of this review.
Exercise components
Type of hydrotherapy program
Aerobic exercise, with a warm-up and a cool-down or relaxation period were common features of the hydrotherapy programs analyzed in this systematic review. This is consistent with the subgroup analyses of other systematic reviews on the effectiveness of general exercise programs for FMS.Citation2–Citation4
Duration
The findings of this review suggest that a hydrotherapy session of between 30 and 60 minutes is of a sufficient duration to make significant changes to a range of outcomes for FMS. This review also demonstrates that programs of a relatively short duration (4–6 weeks) can still result in improved outcomes. Great variability is seen in the overall durations of the programs used in trials. Program duration may have been determined by a range of factors including what was convenient to study administrators or participants. No trial stated a rationale or referred to the literature to justify the duration of their hydrotherapy program.
Frequency
Although the majority of trials included in this review used a frequency of three sessions per week, this review demonstrates that a hydrotherapy program conducted twice a week can also lead to positive outcomes for FMS. The chosen frequency of sessions in clinical practice may depend on financial, organizational, motivational or time-related factors. Although an exercise prescription of twice a week is below that suggested by physical fitness guidelines, the findings of this review suggest that twice weekly hydrotherapy is as effective as more frequent hydrotherapy. Citation27 This finding may have implications for those who are not able to attend hydrotherapy more than twice a week.
Intensity
Of the trials that accurately reported their exercise intensity, a range of exercise intensity of 60%–80% HRmax was observed. This review did not attempt to classify exercise intensity into low, moderate and high categories, but it seems reasonable to consider 60%–80% HRmax as a moderate range of exercise intensity. This finding is consistent with the subgroup analysis of a recent Cochrane review on the effectiveness of general exercise for FMS.Citation2 Heart rate monitors and patient-rated scales of perceived exertion are possible methods that can be used to standardize the intensity of hydrotherapy exercise in a clinical setting.
Method of progression
A patient who is compliant with an exercise program should ideally progress to more challenging exercises as their pain, function and quality of life improve. Only three trials reported progressing the difficulty of their program as their participants improved.Citation14,Citation19,Citation25 As a result, based on the findings of this review, a strong statement regarding the most appropriate method of progression of programs cannot be made.
Environmental components
Most of the hydrotherapy programs analyzed in this review were conducted in pool environments and did not describe the mineral or chemical content of the water. Sea water or water with added minerals or chemicals may help to increase compliance with hydrotherapy programs or promote relaxation or enjoyment, both of which could potentially improve the outcomes of hydrotherapy programs. Equipment that provides flotation or resistance to movement may increase the type of exercises that can be prescribed as a part of a hydrotherapy program, and may help those supervising hydrotherapy programs to prescribe exercises for those with co-morbidities.
Service delivery components
Despite the fact that only five of the 11 trials included in this review reported the credentials of those supervising their program, it is noted that all five programs were supervised by physiotherapists. Professional supervision may be an important component of hydrotherapy programs for FMS.
Outcome measures
All of the trials that reported significant between-group outcomes compared hydrotherapy to a no intervention group. In contrast, the majority of trials that reporting no significant difference between their intervention and comparison groups used an exercise-based comparison group. In these trials (comparing two forms of exercise) both groups had improved. Exercise therefore appears to be a very important component of a hydrotherapy program for FMS (as opposed to passive water-based therapies). A direct comparison of passive and active water-based therapies is beyond the scope of this review.
Mental health-related outcomes
In addition to physical outcomes, 10 out of 11 trials reported significant mental health-related outcomes. Anxiety and depression are two conditions which are commonly associated with FMS.Citation7,Citation22 Improved anxiety and depression-related outcomes were reported immediately following intervention periods and after follow up periods in a number of trials. One trial demonstrated no significant difference between a hydrotherapy group and a passive balneotherapy group over a range of outcomes.Citation23 However, depression scores were significantly lower both immediately following intervention and at follow up (between group measures). This finding may indicate that although passive treatments of FMS in warm water can lead to improvements in FMS-related outcomes, the exercise component may be more important in changing depression-related outcomes. This is consistent with the findings of systematic reviews on the effectiveness of exercise in the management of mild to moderate clinical depression.Citation28–Citation31
Limitations of this review
As with any research, this systematic review also has some limitations. Firstly, the very nature of a systematic review inhibits a broad and diverse approach to the literature. For example, this systematic review is limited to randomized controlled trials published in the last 10 years. It is possible the literature published prior to this period may be relevant to the review question. Similarly, while all attempts were made to interrogate and access all relevant literature, it is possible some publications may have been missed in the search process. This could have been due to access to relevant databases, use of alternate key words and varying terminologies. However, as this review identified more than 10 randomized controlled trials on the same topic, the body of evidence to inform the review question is considerable. Secondly, this review only presents components of hydrotherapy programs that are effective and does not consider components of hydrotherapy programs that are ineffective.
Clinical implications
This systematic review builds on the findings of previous systematic reviews and randomized controlled trials on this topic. Clinicians can utilize the findings of this review in the creation of their own hydrotherapy programs for FMS. According to the findings of this review, the exercise component of a hydrotherapy program for FMS should include some form of aerobic activity. Including a warm-up, cool-down or relaxation period as well as either a flexibility or strength-based component, for a duration of at least four weeks at a frequency of three times per week is also recommended. Self-rated depression or anxiety scales can be used to monitor mental health outcomes.
Directions for future research
Hydrotherapy for FMS is a topic which was been evaluated extensively in the literature in recent years. Nevertheless there are still some aspects to this topic which require further evaluation. Further research is required to determine the most appropriate duration of hydrotherapy programs for FMS, and whether improvements can be maintained when programs are continued independently. This information is of interest from both a clinical and an economic perspective. More research comparing passive water-based therapies to hydrotherapy would also be of value from an economic perspective.
Conclusion
Aerobic exercise, warm up and cool-down periods and relaxation exercises are common features of hydrotherapy programs reported in randomized controlled trials that have reported significant FMS-related outcomes. Flexibility and strength-based exercises were also commonly utilized. Treatment durations of 60 minutes, frequencies of three sessions per week and exercise intensities equivalent to 60%–80% HRmax were the most common exercise components used in programs. When considering exercise, environmental, and service delivery components, exercise appears to be the most important factor in hydrotherapy programs, particularly when considering mental health-related outcomes.
Disclosures
The authors report no conflicts of interest in this work.
References
- WolfeFSmytheHAYunusMBThe American college of rheumatology 1990 criteria for the classification of fibromyalgiaArthritis Rheum19903321601722306288
- BuschAJBarberKAOverendTJPelosoPSchachterCLExercise for treating fibromyalgia syndromeCochrane Database of Syst Rev20074CD00378617943797
- BuschAJSchachterCLOverendTJPelosoPBarberKARExercise for fibromyalgia: a systematic reviewJ Rheumatol20083561130114418464301
- JonesKDAdamsDWinters-StoneKBurckhardCSA comprehensive review of 46 exercise treatment studies in fibromyalgiaHealth Qual Life Outcomes200641677216999856
- SimJAdamsNSystematic review of randomized controlled trials of nonpharmacological interventions for fibromyalgiaClin J Pain20021832433612218504
- RossyLABuckelewSPDorrNA meta-analysis of fibromyalgia treatment interventionsAnn Behav Med199921218019110499139
- McVeighJGMcGaugheyHHallMKanePThe effectiveness of hydrotherapy in the management of fibromyalgia syndrome: a systematic reviewRheumatol Int20082911913018751709
- LacasseMLafortuneVBartlettLGuimondJAnswering clinical questions: what is the best way to search the webCan Fam Physician2007531535153617872886
- MaherCGSherringtonCHerbertRDMoseleyAMElkinsMReliability of the PEDro scale for rating quality of randomized controlled trialsPhys Ther200383871372112882612
- MoherDCookDJJadadARAssessing the quality of reports of randomised trials: implications for the conduct of meta-analysesHealth Technol Assess1999312
- HallJSkevingtonSMMaddisonPJChapmanKA randomized and controlled trial of hydrotherapy in rheumatoid arthritisArthritis Care Res1996932062158971230
- FryACThe role of resistance exercise intensity on muscle fibre adaptationsSports Med2004341066367915335243
- NobleBJBorgGAVJacobsICeciRKaiserPA category ratio perceived exertion scale: relationship to blood and muscle lactates and heart ratesMedicine Sci Sports Exerc1983156523528
- De AndradeCSCarvalhoRFPPSoaresASAbreu FreitasRPGuerraLMMVilarMJThalassotherapy for fibromyalgia: a randomized controlled trial comparing aquatic exercises in sea water and water poolRheumatol Int20082914715218600327
- NasermoaddeliAKagomimoriSBalneotherapy in medicine: a reviewEnvion Health Prev Med200510171179
- EvcikDYigitIPusakHKavuncuVEffectiveness of aquatic therapy in the treatment of fibromyalgia syndrome: a randomized controlled open studyRheumatol Int20082888589018278501
- GusiNTomas-CarusPHäkkinenAHäkkinenKOrtegra-AlonsAExercise in waist-high warm water decreases pain and improves health-related quality of life and strength in the lower extremities in women with fibromyalgiaArthritis Rheum2006551667316463415
- Tomas-CarusPHäkkinenAGusiNLealAHäkkinenKOrtega-AlonsoAAquatic training and detraining on fitness and quality of life in fibromyalgiaMed Sci Sports Exerc20073971044105017596770
- AssisMRSilvaLEAlvesAMBA randomised controlled trial of deep water running: clinical effectiveness of aquatic exercise to treat fibromyalgia syndromeArthritis Rheum2006551576516463414
- IdeMRLaurindoIMMRodrigues-JuniorALTanakaCEffect of aquatic respiratory exercise-based program in patients with fibromyalgiaInt J Rheum Dis200811131140
- JentoftESRKvalvikAGMengshoelAMEffects of pool-based and land-based aerobic exercise on women with fibromyalgia/chronic widespread muscle painArthritis Rheum2001451424711308060
- Tomas-CarusPHäkkinenAGusiNLealAHäkkinenKOrtega-AlonsoAEight months of physical training in warm water improves physical and mental health in women with fibromyalgia: a randomized controlled trialJ Rehab Med200840248252
- AltanLBingölUAykaçMKoçZYurtkuranMInvestigation of the effects of pool-based exercise on fibromyalgia syndromeRheumatol Int20042427227714508601
- GowansSEdeHueckAVossSRichardsonMA randomized controlled trial of exercise and education for individuals with fibromyalgiaArthritis Care Res199912212012810513500
- GowansSEdeHueckAVossSSilajAAbbeySEReynoldsWJEffect of a randomized, controlled trial of exercise on mood and physical function in individuals with fibromyalgiaArthritis Rheum200145651952911762686
- GowansSEdeHueckAVossSSilajAAbbeySESix-month and one-year followup of 23 weeks of aerobic exercise for individuals with fibromyalgiaArthritis Rheum200451689089815593364
- EggerGDonovanRJGiles-CortiBBullFSwinburnBDeveloping national physical activity guidelines for AustraliansAust N Z J Public Health200125656156311824996
- MeadGEMorleyWCampbellPGreigCAMcMurdoMLawlorDAExercise for depressionCochrane Database of Syst Rev20084
- CraftLLLandersDMThe effect of exercise on clinical depression: a meta-analysisMed Sci Sports Exerc19983053393579526878
- LawlorDAHopkerSWThe effectiveness of exercise as an intervention in the management of depression: systematic review and metaregression analysis of randomised controlled trialsBr Med J2001322728976377111282860
- StrathopoulouGBowersMBBerryACSmitsJAJOttoMWExercise interventions for mental health: a quantitative and qualitative reviewClin Psychol2006132179193