Abstract
The aim of this survey is to report anesthesiologists’ perception of patients’ anxiety under regional anesthesia, its frequency, effects and causes, and the strategies employed to reduce it. Electronic questionnaires were sent to all grades of anesthesiologists in Nottingham, UK. The response rate for the survey was 79%. Over half of the anesthesiologists in our region believe that anxiety during regional anesthesia is not common. Surgery and anesthesia, followed by block failure were reported by anesthesiologists as the most common causes of patients’ anxiety. Frequently employed techniques to manage anxiety were communication or sedation. Most respondents felt that regional anesthesia provides good analgesia and patient satisfaction. However, 20% felt that regional anesthesia is painful or unpleasant for patients, perhaps explaining the reluctance by some anesthesiologists to perform regional anesthesia.
Keywords:
Introduction
Having surgery is a stressful event in a patient’s life. Anxiety is common pre- operatively, with a prevalence of up to 80%.Citation1–Citation3 Common causes of patients’ anxiety are fear of surgery, anesthesia and complications (eg, pain and nausea), previous unpleasant experience of anesthetics or surgery or a predisposing personality.Citation4–Citation7 Previous “good” experiences (of anesthetics or surgery) invariably mean a more relaxed patient.Citation8
Patients’ expectations of the attitude and behavior of the staff toward them are another important factor that may affect their anxiety and overall hospital experience. If patients are unduly anxious and apprehensive about their operation, their physical recovery, well-being, and overall experience may be negatively affected. Many studies have investigated different interventions and their effect on patients’ anxiety. These interventions include pharmacological anxiolytics,Citation9 distraction therapy,Citation10 and provision of information.Citation11–Citation13
Anesthesiologists’ have a variable perception of patients’ anxiety. Controversy exists on the ability of anesthesiologists to assess and predict patients’ anxiety before surgery. Badner et alCitation14 reported that anesthesiologists are frequently inaccurate when assessing patients’ anxiety and that they usually tend to underestimate it.Citation14 They recommended using more objective measures of anxiety (eg, visual analog scale) rather than relying on the assessment of the care provider. Nurses also inaccurately assess patients’ anxiety, the commonest inaccuracy being overestimation.Citation15
In contrast to Badner, anesthesiologists (using their clinical judgment) were found to accurately predict patients’ anxiety.Citation16 However, this study only examined a restricted group of patients (obstetrics) and a modest correlation was found. Huppe et alCitation17 concluded that reliable estimation of anxiety is best sourced from patients.
With the growing number of surgical procedures that are performed under regional anesthesia; studies are emerging investigating patients’ anxiety undergoing procedures under regional anesthesia and our ability to assess and predict preoperative anxiety of patients having regional anesthesia.
In the present survey, we report how anesthesiologists perceive patient anxiety, its frequency, effects and causes, and their management strategies towards anxious patients having surgery under regional anesthesia. We wished to identify the variation in the current attitude of a group of anesthesiologists in the UK and to discuss this variation in the context of current evidence.
Methods
The survey was reviewed by the local research ethics committee (LREC), who deemed that formal LREC application was unnecessary for this survey. The survey was carried out as part of a larger randomized controlled study designed to investigate improving patients’ anxiety regarding regional anesthesia.
Design
The questionnaire (appendix) was primarily designed to report the findings of some common problems facing anxious patients under regional anesthesia and the how anesthesiologists deal with them in accordance with anesthetic practice in the UK. The survey was set up as an on-line electronic questionnaire (www.surveymonkey.com). The questions in this survey consisted of a series of closed statements answered “Yes” or “No”. In addition, some questions were answered using a grading scale (1 = never/rarely, 2 = often, 3 = always). Anesthesiologists were instructed to report their opinions on how they perceive patients’ anxiety, its frequency and causes. Additionally, from a list of anxiety management strategies, respondents were instructed to select which technique they routinely use to alleviate their patients’ anxiety. Respondents were also asked about their perception of patients’ satisfaction following regional anesthesia. Finally, anesthesiologists were encouraged to add any comments as free text.
Sample
The preliminary draft of the questionnaire was first distributed to 10 anesthesiologists in our department, testing for accuracy, layout and clarity. No problem with the questionnaire was found. The generated electronic link to access the survey was then sent to 130 anesthesiologists of different grades in Nottinghamshire, UK in February 2008. Anesthesiologists’ email addresses were obtained from the database of the Nottingham and East Midlands School of Anesthesia and Nottingham University Hospital NHS Trust. Background data, including age, gender, and grade of anesthesiologists were collected. Consent was implied by submission of the completed survey. All completed questionnaires were anonymized. A second reminder was sent after four weeks for those who did not reply to the first questionnaire.
Statistics
Numbers (percentages) of respondents were calculated and presented for each item in the questionnaire. Additional weighted average responses (WAR) were also quoted. Data were stored and analyzed in Microsoft Excel 2007 (Microsoft Corporation, WA, USA).
Results
Datasets for 111 anesthesiologists (of various grades) were obtained. The response rate for the survey was 79%. The majority of participants were middle grade (40%) and consultants (43%), aged more than 31 yr (83%). There were more males (67%) than females ().
Table 1 Demographic data of the respondents
Respondents’ views were summarized into four categories
The frequency of patients’ anxiety and perception of regional anesthesia ()
Only one third of respondents felt that anxiety is common among patients having regional anesthesia, mostly in the pre-operative period (62%). Although a minority of anesthesiologists (23%) felt that patients’ anxiety is a problem; nearly half of them probably still underestimate it.
Table 2 Anesthesiologist’s perception of patients’ anxiety, its frequency and effects during regional anesthesia
Despite over half of anesthesiologists thinking that they are prepared to deal with anxious patients, they admitted that patients’ anxiety may increase their own anxiety, and reduce the overall success rate of the block. Fewer felt that anxiety may affect their confidence in performing the block (35%).
Causes of patients’ anxiety ()
Anesthesia (85%) and surgery (77%), followed by block failure (65%) were reported by anesthesiologists as the most common causes of patients’ anxiety. Over two thirds of respondents thought that insufficient or detailed pre-operative anesthetic information may not contribute to increasing patients’ anxiety.
Table 3 Causes of patient anxiety as anesthesiologists reported it
Nearly two thirds of anesthesiologists felt that patients’ misconception or misinformation about regional anesthesia from family, friends or surrounding media is another cause of patients’ anxiety. Only a third of respondents (32%) reported that patients’ recall of previous negative experience of the block, and any possible complication of the block, may increase patients’ anxiety.
Management strategies to reduce anxiety ()
The commonest strategies employed by anesthesiologists to reduce patients’ anxiety were communication with the patient and reassurance (95%), giving sedation (82%) and the use of distraction techniques (eg, listening to music) (54%). Only 15%–20% of respondents felt that partner attendance with the patient or watching the operation through a camera in the operating theatre may help alleviate patients’ anxiety.
Figure 1 Anesthesiologists’ management strategies to reduce patients’ anxiety.
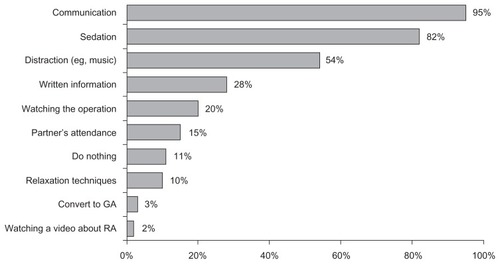
Only one third of respondents thought that written information about the block or allowing patients to see their nerves while being anesthetized on the ultrasound screen may reduce fear and anxiety. A minority of respondents (10%) do not intervene to reduce the anxiety in anxious patients, or may implement relaxation techniques (eg, deep breathing, meditation). None of respondents postpone anxious patients’ surgery and only 2% may convert to general anesthesia.
Patients’ satisfaction with regional anesthesia ()
Almost all respondents felt that regional anesthesia provides good analgesia and patient satisfaction. They also thought that patients would have the block again if needed in the future (>94%). However, nearly 20% felt regional anesthesia is painful or unpleasant for patients. Respondents provided additional comments at the end of the survey. Their comments are summarized below ().
Table 4 Patients’ experience with the block from anesthesiologists’ perspective
Table 5 Respondents’ comments
Discussion
This survey revealed that over two thirds of respondents thought that anxiety is uncommon among patients having surgery while they are awake (having regional anesthesia); this is consistent with recent reports which showed a low rate of self-reported anxiety (36%) among regional anesthesia patients.Citation18,Citation19
In the present survey, most surveyed anesthesiologists felt they are always prepared to manage anxiety; however, half of them admitted to underestimating it, and only a third can accurately predict it; in agreement with what was previously reported in that anesthesiologists are poor predictors of patients’ anxiety and they usually tend to underestimate it.Citation14
Anesthesia and surgery have been rated as the most common anxiety-provoking factors; similar findings have been reported by other studies.Citation5–Citation7 Additional reported causes of anxiety may include inaccurate information conveyed to the patients from people, the internet, or advertising media. Patients may have been inaccurately informed by television or written stories that often exaggerate the frequency and impact of complications.
Interestingly, most anesthesiologists believe that too much or too little information seems to have a small effect on patients’ anxiety; this leaves anesthesiologists with the quandary of what is the appropriate amount of information to be conveyed to patients without increasing their anxiety.Citation20,Citation21
Patients are usually concerned about anesthetic complications (eg, pain and nerve damage); this has been found to be associated with the increased levels of anxiety.Citation4,Citation5 However, less than one third of respondents think patients’ fear of complications may increase their anxiety. This may suggest inaccuracy among anesthesiologists by underestimating patients’ fear due to any possible complications. Although these studies examined anxiety in patients having general anesthesia; lack of data about patients’ anxiety during regional anesthesia makes it difficult to compare these findings.
Anesthesiologists felt that talking to patients and reassuring them, is the most effective method in reducing patients’ anxiety. Indeed, a confident, professional and friendly relationship with the patient reduces anxiety. Seeing patients well in advance (as opposed to keeping them uninformed, then, one hour before surgery giving them all information and asking them to decide) with adequate explanation of the benefits and risks, along with constant communication and reassurance throughout the procedure, would establish rapport, build confidence and trust, and alleviate fears. Such patients do not usually feel pressurized.Citation22 Respondents’ comments have suggested that simple reassurance and the affirmation that the patient always “has the option to go to sleep if needed”, is usually enough to allay most anxieties.
Anesthesiologists often give sedative drugs or advise patients to listen to music of their preference, either preoperatively or during the operation. All of these measures are well established methods to reduce patients’ anxiety,Citation9,Citation10 and patients usually gain benefit from them.Citation23 Several respondents commented upon the effectiveness of using anatomy slides and an orthopedic spine model to demonstrate how/where spinal/epidural needles are inserted, emphasizing they do not go into the cord itself.
Although viewing an anesthetic film about regional anesthesia pre-operatively or watching the operation intra-operatively has been shown to decrease patients’ anxiety;Citation19,Citation24 only a minority of the respondents agreed that these two interventions were helpful to lessen patients’ anxiety. This may have added to the controversy regarding the efficiency of these methods,Citation25,Citation26 and the availability of these educational materials in our hospitals. These figures may be similar to those found in a study by Hyde et alCitation23 who reported more than two thirds of patients preferred not to watch the operation.
It is unusual or often not practical to have the patient’s partner in attendance during a surgical procedure except in obstetrics where it is routine (at the mother’s request). Anesthesiologists, in our survey, do not think partner attendance may help in improving patients’ anxiety. In the literature, this has also shown a small positive effect on patients’ anxiety, but was not considered to be clinically important.Citation27
Despite all available measures adopted by anesthesiologists to help patients feel calm and less anxious, there is still a significant number of anesthesiologists who do nothing to manage anxious patients. Probably, these respondents underestimate anxiety, or do not consider it as a problem that needs to be solved.
Anesthesiologists felt that high levels of patients’ anxiety may decrease the success rate of the block. Patients’ anxiety was previously found to increase the failure rate of regional anesthesia. Citation28 This could be due to the direct effect of patients’ anxiety on their anxiety and confidence in performing the block.
It is believed among anesthesiologists that regional anesthesia provides excellent anesthesia/analgesia; and that this will improve patients’ satisfaction. As a result, most patients would have a similar block if needed in the future. However, fewer patients (18%–20%) still experience some degree of pain and discomfort during the block procedure,Citation29 possibly due to differences in patients’ perception of pain, or practitioners’ experience. This may explain the reluctance by some anesthesiologists to perform regional anesthesia.
Conclusion
Anesthesiologists in our region reported that anxiety during regional anesthesia is uncommon and that surgery and anesthesia, followed by block failure are the most common causes of patients’ anxiety pre-operatively. The most commonly employed techniques to manage anxiety were communication followed by sedation. Virtually all respondents felt that regional anesthesia provides good analgesia and patient satisfaction. However, approximately 20% felt that the procedures are painful or unpleasant for patients, perhaps explaining reluctance by some anesthesiologists to perform regional anesthesia.
Disclosure
The authors report no conflicts of interest in this work. The work was not supported by any external funding.
References
- HashimotoYBabaSKohHTakagiHIshiharaHMatsukiAAnxiolytic effect of pre-operative showing of anesthesia video for surgical patientsMasui1993426116168315804
- ShevdeKPanagopoulosGA survey of 800 patients’ knowledge, attitudes and concerns regarding anesthesiaAnesth Analg1991731901981854034
- NorrisWBairdWLPre-operative anxiety: a study of the incidence and aetiologyBr J Anaesth1967395035096027959
- ScottLEClumGAPeoplesJBPre-operative predictors of postoperative painPain1983152832936856324
- MitchellMJPsychological preparation for patients undergoing day surgeryAmbul Surg200081929
- MitchellMPatients’ perceptions of pre-operative preparation for day surgeryJ Adv Nurs1997263563639292371
- CarrEKatrinaBSandraAPaulSPatterns and frequency of anxiety in women undergoing gynecological surgeryJ Clin Nurs20061534135216466484
- KindlerCHHarmsCAmslerFIhde-SchollTScheideggerDThe Visual Analog Scale allows effective measurement of pre-operative anxiety and detection of patients’ anesthetic concernsAnesth Analg20009070671210702461
- MackenzieNSedation during regional anaesthesia: indications, advantages and methodsEur J Anaesthesiol19961327
- BechtoldMLPerezRAPuliSRMarshallJBEffect of music on patients undergoing outpatient colonoscopyWorld J Gastroenterol2006127309731217143946
- BondyLRSimsNSchroederDROffordKPNarrBJThe effect of anesthetic patient education on pre-operative patient anxietyReg Anesth Pain Med19992415816410204903
- HughesSThe effects of giving patients preoperative informationNurs Stand200216333711949188
- KlopfensteinCEForsterAVan GesselEAnesthetic assessment in an outpatient consultation clinic reduces pre-operative anxietyCan J Anaesth20004751151510875713
- BadnerNHNielsonWRMunkSKwiatkowskaCGelbAWPreoperative anxiety: detection and contributing factorsCan J Anaesth1990374444472340614
- JohannaHMaritaPVesaVPekkaLFear of patients related to coronary arteriographyJ Adv Nurs19982854629687130
- HicksJAJenkinsJGThe measurement of preoperative anxietyJ R Soc Med1988815175193184108
- HuppeMUhligTHeinzeJVogelsangHSchmuckerPMethodological approaches for the assessment of emotional states in anesthesiologyAnasthesiol Intensivmed Notfallmed Schmerzther20003531110689516
- MitchellMConscious surgery: influence of the environment on patient anxietyJ Adv Nurs20086426127118785887
- JlalaHFrenchJFoxallGHardmanJBedforthNEffect of pre- operative multimedia information on perioperative anxiety in patients undergoing procedures under regional anaesthesiaBr J Anaesth201010436937420124283
- InglisSFarnillDThe effects of providing pre-operative statistical anaesthetic-risk informationAnaesth Intensive Care1993217998058122737
- GardenALMerryAFHollandRLPetrieKJAnaesthesia information – what patients want to knowAnaesth Intensive Care1996245945988909673
- HuPHarmonDFrizelleHPatient comfort during regional anesthesiaJ Clin Anesth200719677417321932
- HydeRBrydenFAsburyAJHow would patients prefer to spend the waiting time before their operations?Anaesthesia1998531921959534647
- BayarATuncayIAtasoyNAyogluHKeserSEgeAThe effect of watching live arthroscopic views on postoperative anxiety of patientsKnee Surg Sports Traumatol Arthrosc20081698298718566798
- SalzwedelCPetersenCBlancIKochUGoetzAESchusterMThe effect of detailed, video-assisted anesthesia risk education on patient anxiety and the duration of the preanesthetic interview: a randomized controlled trialAnesth Analg200810620220918165579
- DoneMLLeeAThe use of a video to convey pre-anesthetic information to patients undergoing ambulatory surgeryAnesth Analg1998875315369728822
- PrabhuMWangLFTaitARBulloughASA randomized controlled study of whether the partner’s presence in the operating room during neuraxial anesthesia for cesarean delivery reduces patient anxietyInt J Obstet Anesth20091836236719733054
- LavidaleaMMurataOValléaBMaguèsaJFuzieraRRichezAAcute patient’s anxiety increases axillary brachial plexus block failure [Abstract]Reg Anesth Pain Med200631e2
- RungGWMcQuillanPMWilliamsDPRiemondySPatients’ perception of regional anesthesia at a university hospitalReg Anesth Pain Med19982361
Appendix
Anesthesiologists’ perception of patients’ anxiety under regional anesthesia
How concerned are you that anxiety is a problem during regional anesthesia (a lot, a little, none)?
What proportion of your patients undergoing regional anesthesia are anxious patients (most, some, none)?
In your opinion, what is the most concerning time for patients undergoing regional anesthesia (pre-op, intra-op, post-op)?
Do you feel prepared to react toward differing types of anxious patients’ behaviors during regional anesthesia (always, sometimes, never)?
Does differing advice from surgeon and anesthesiologist regarding the various anesthetic techniques increase patients’ anxiety (yes, no)?
How accurately do you think you assess your patients’ anxiety prior to regional anesthesia (overestimate it, underestimate it, correctly estimate it).
Does patient anxiety have any effect on your anxiety (yes, no)?
Does patient anxiety have any effect on your level of confidence in performing the block (yes, no)?
Does patient anxiety have any effect on the success of the block itself (yes, no)?
How important is patient satisfaction to your practice (high, low)?
How often do you track your patients’ satisfaction after a procedure under regional anesthesia (never, often, always)?
How often do you use the following techniques to alleviate patients’ anxiety?
Please rate your answer (never/rarely, often, always).
Do nothing
Give sedation
Written information/leaflet.
Postpone the operation
Communication/reassurance/tell a joke
Convert to general anesthesia
Distraction (eg, music, read a book)
Partner’s attendance (partner/friend/relative)
Patients watching a video about regional anesthesia
Patients watching the procedure via operating camera
Encourage them to use relaxation techniques (eg, deep breathing/meditation)
In peripheral nerve blockade, patients seeing their nerves while being anesthetized on ultrasound screen.
What are the causes of patients’ anxiety? (never/rarely, often, always).
Needle-phobia
Fear of unknown
Fear of the surgery/anesthesia
Recall of previous bad experience
Fear of complications (pain/nerve damage)
Regional anesthesia might make operation less successful
Giving patients detailed anesthetic information pre-op
Giving patients little anesthetic information pre-op
Misinformation from lay people, family, friends, and surrounding media.
Regarding the block, do you think...? (never/rarely, often, always)
Patients find the block unpleasant
Patients remember the events during the block
Patients experience pain during the block
Patients experience pain during surgery
Patients have adequate pain relief after surgery
Following regional anesthesia, patients would have a block again
Patients are satisfied with the block.
Please add any further comments...............