Abstract
Epiglottic cyst is not an unusual disease in the larynx. Although it is usually a benign lesion, airway problems may occur due to a large cyst. Surgical excision is usually the treatment of choice, with low recurrence. Because of the limited view and mobility of laryngoscopes, there is sometimes difficulty in the procedure of excision or marsupialization, especially in wide-based epiglottic cysts. The microdebrider has been widely used in treatment of otolaryngological diseases, and specialized blades were designed for laryngeal lesions. We report the use of a microdebrider for treatment of wide-based epiglottic cysts in six patients. The follow-up period ranged from five months to 62 months without recurrence. One hand-powered instrument provided a clear surgical field for precise removal of the cyst and synchronized suction, and increased mobility of the laryngoscope held in the other hand. In comparison to traditional microinstrumentation and carbon dioxide laser, the microdebrider offered a rapid and effective alternative in treatment of wide-based epiglottic cyst.
Introduction
Although epiglottic cyst is a benign disease, its size and location may result in airway complications.Citation1 The treatment of choice is surgical removal. Laryngoscope with microsurgery is sometimes time-wasting and difficult to perform in a small surgical field, especially for wide-based epiglottic cyst. A powered instrument provides precise cutting through immediate exposure of the surgical field, and synchronized suction removes blood and specimen fragments. This technique is practical and time-saving, with rare recurrence.Citation2 For the treatment of epiglottic cyst, in addition to laryngomicrosurgery with traditional microinstrumentation and carbon dioxide laser, the laryngeal blade microdebrider offers a valuable and effective alternative.
Materials and methods
From August 1999 through December 2000, six patients with wide-based epiglottic cyst received surgical procedure under general anesthesia, using a laryngoscope and long-armed laryngeal blade equipped with a microdebrider. The ages of the patients ranged from 42 to 84. All patients underwent general anesthesia via transoral endotracheal intubation. The direct laryngoscope was held in one hand to explore the cyst, and the Xomed XPS shaver system with laryngeal blades (Xomed Surgical Products, Inc. [Medtronic], Jacksonville, FL, USA) was held in the other hand to perform surgery. The instrumentation is shown in . Different cutting tips were used for rapid debulking of the cyst and delicate removal of residual lesions (). The cyst was deroofed with care to avoid damage of epiglottic cartilage (–). Specimens were collected at the time of surgery via an in-line specimen trap. The bleeding of surgical field could be controlled by compression of epinephrine-soaked gauzes. The data of all patients are summarized in .
Figure 1 Powered instrumentation with laryngeal blade and video system.

Figure 2 Two kinds of blade.

Figure 3 Laryngoscopic view. Epiglottic cyst*, lingual tonsil area**.
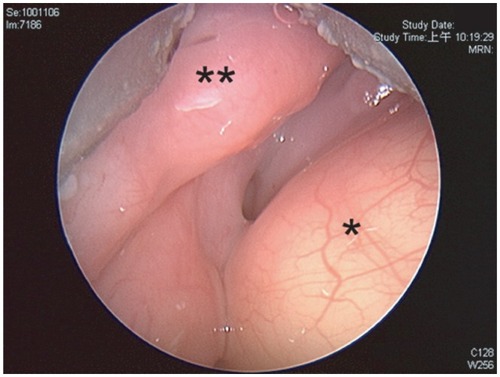
Figure 4 Epiglottic cyst*, lingual tonsil area**, arrow shows cutting edge of blade.
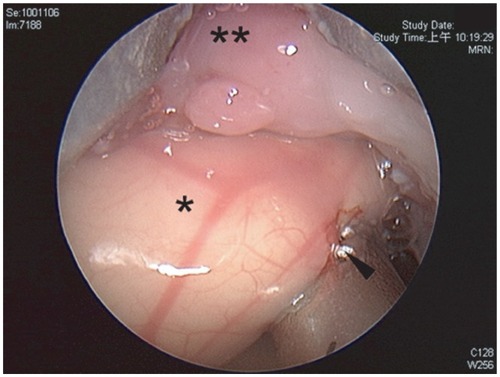
Figure 5 Ruptured cyst*, arrow shows blade, double arrow shows endotracheal tube.
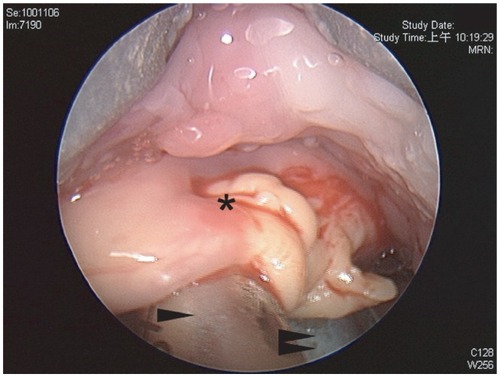
Figure 6 Deroofed cyst* wound, arrow shows epiglottis, double arrow shows endotracheal tube.
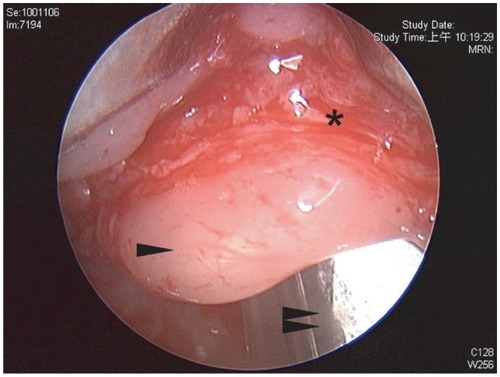
Table 1 The data of patients receiving removal of epiglottic cysts with powered microdebrider
Results
All patients stayed in ward of the hospital after operation for one day and then were followed up in the outpatient department (OPD) regularly. The specimens collected from the trap were adequate for histological diagnosis. The follow-up period ranged from five months to 62 months. There was no recurrence noted during the regular OPD follow-up.
Discussion
Epiglottic cyst is a benign tumor, contributing about 4.3% to 6.1% of all laryngeal benign tumors. Although it is a benign lesion, its presentation of symptom ranges from asymptomatic to lethal outcome, depending on its size and location. Epiglottic cyst can occur at all ages, and the most common is in the sixth decade.Citation1
According to Asherson’s classification, there are three kinds of laryngeal cysts: (1) ductal cysts, (2) saccular cysts, and (3) thyroid-cartilage foraminal cysts, which are rare. Ductal cysts are common, and result in obstruction of collecting ducts of the salivary glands in the larynx. They are also called retension cysts or mucous cysts. Ductal cysts occurred at any place of the larynx, mainly located within the mucous membrane, covered with squamous or ciliated columnar epithelium. Saccular cysts are delivered from the saccule of the laryngeal appendage, and are also called congenital embryonic cysts. They are often seen in neonates, although sometimes in adults. Saccular cysts are larger than ductal cysts, and can occur in the laryngeal ventricle, vocal cords, false cords, and the aryepiglottic fold. Saccular cysts are submucosal lesions and covered with complete mucosa. Thyroid-cartilage foraminal cysts occur in thyroid cartilage. They are due to residual embryonic vessels in thyroid cartilage protruded with mucosa. Epiglottic cysts are often ductal cysts, and the most common location is the lingual surface of the epiglottis. Sometimes they extend to the aryepiglottic fold or the laryngeal surface of the epiglottis. The differential diagnosis includes thyroglossal duct cyst, lymphangioma, hemangioma, chondroma, lingual thyroid, and papilloma.Citation3
The correct diagnosis of epiglottic cyst depends on disease history-taking and physical examination. The lesion can be seen with indirect laryngeal mirror or flexible fiberoptic laryngoscopy. Other examinations such as neck lateral plain film, thyroid scan, and computed tomography scans also provide useful information for diagnosis.
The treatment of choice for epiglottic cyst is surgical removal. Usually, surgeons use traditional laryngomicrosurgery or carbon bicarbonate laser under microscopy.Citation4 Complete excision of the cyst reduces recurrence, but it needs longer surgical and anesthetic time.Citation5 Also, the surgical field is limited under microscopy, and the mobility of the laryngoscope is also restricted during surgical excision. It is more difficult to remove a wide-based epiglottic cyst in a small and immobile surgical field. In addition, during excision of wide-based cyst by traditional instrumentation, the surgical field will be easily blurred by blood accumulation. The surgical field may be better with laser surgery, but it is also not easy to excise wide-based epiglottic cyst with poor mobility and need to adjust laryngoscope and microscope frequently.
Microdebriders have been widely used in the otolaryngological field for sinus surgery, adenoidectomy, uvulopalatopharyngoplasty, laryngeal and tracheal lesions. We report here the use of microdebrider for treatment of wide-based epiglottic cyst.Citation6–Citation10 The powered instrument, or microdebrider, equipped with long-armed laryngeal blade provided precise cutting through immediate exposure of the surgical field and synchronized suction.Citation11,Citation12 The blade with suction grasps a point of the cystic wall, and the surgeon made a through cutting of the mucosa by paddle controller. At the same time, the suction removes surrounding blood to keep the surgical field clear. All these functions were controlled in one hand, while the laryngoscope could be held in the other hand or in fixed condition. The laryngoscope was equipped with endoscope and video-monitor system to provide a magnified view. Wide-based epiglottic cyst usually extended beyond one surgical field, so we could adjust the laryngoscope immediately to proper position for further cyst deroofing. Hemostasis was usually achieved by compression of epinephrine gauze, and electrocauterization was rarely needed. Although the microdebrider produce fragments of tissue which were smaller than those obtained by conventional excision, histological diagnosis was possible by using a standard in-line suction trap on the microdebrider.Citation13
In addition to traditional surgery with microinstrumentation and laser surgery, the laryngeal blade microdebrider offers a valuable and effective alternative. The surgeon should be familiar with the characteristics and operation of the powered instrument to avoid unnecessary complications.
Disclosure
The authors report no conflicts of interest in this work.
References
- LamHCAbdullahVJSooGEpiglottic cystOtolaryngol Head Neck Surg2000122231110652415
- FlintPWPowered surgical instruments for laryngeal surgeryOtolaryngol Head Neck Surg2000122226326610652402
- DeSantoLWDevineKDWeilandLHCysts of the larynx – classificationLaryngoscope19708011451765411821
- SuCYHsuJLTransoral laser marsupialization of epiglottic cystsLaryngoscope200711771153115417505326
- KawaidaMKohnoNKawasakiYFukudaHSurgical treatment of large epiglottic cysts with a side-opened direct laryngoscope and snareAuris Nasus Larynx199219145501514946
- KoltaiPJChanJYounesAPower-assisted adenoidectomy: total and partial resectionLaryngoscope20021128 Pt 2 Suppl 100293112172236
- MurrayNFitzpatrickPGuariscoJLPowered partial adenoidectomyArch Otolaryngol Head Neck Surg2002128779279612117337
- ParsonsDSBothwellMRPowered instrument papilloma excision: an alternative to laser therapy for recurrent respiratory papillomaLaryngoscope200111181494149611568590
- RodriguezKMurrayNGuariscoJLPower-assisted partial adenoidectomyLaryngoscope20021128 Pt 2 Suppl 100262812172235
- YanagisawaEWeaverEMEndoscopic adenoidectomy with the microdebriderEar Nose Throat J199776272749046692
- NuyensMZbarenPSeifertEEndoscopic resection of laryngeal and tracheal lesions using the microdebriderActa Otolaryngol2006126440240716608793
- Sant’AnnaGDMauriMUse of the microdebrider for Reinke’s edema surgeryLaryngoscope2000110122114211611129032
- McGarryGWGanaPAdamsonBThe effect of microdebriders on tissue for histological diagnosisClin Otolaryngol Allied Sci19972243753769298616