Abstract
Anthrax, a zoonotic disease that primarily affects herbivores, has received recent attention as a potential agent of bioterrorism. We report a patient who presented with a 4-day history of pain, watering and difficulty in opening the left upper and lower eyelids, and fever. Clinical examination revealed brawny nonpitting edema with serosanguinous discharge. The history of the death of his sheep 1 week prior to the illness provided the clue to the diagnosis. Although standard cultures of the blood and the serous fluid from the lesion were negative, probably as a result of prior treatment, the diagnosis of cutaneous anthrax was made by a polymerase chain reaction (PCR) test of the serous fluid. Serial photographs demonstrating resolution of the lesion with appropriate antibiotic therapy are presented.
Introduction
Anthrax, a zoonotic disease caused by Bacillus anthracis (B. anthracis), primarily affects herbivores including sheep, cattle, horses, and other domestic animals.Citation1 Humans may be affected as a result of exposure to an infected animal or animal products. This organism has received recent attention as a potential agent of bioterrorism.Citation1 Three forms are described: cutaneous, inhalational, and gastrointestinal.Citation1 We describe a patient with oculocutaneous anthrax.
Case description
A 39-year-old male presented to our outpatient clinic with a 4-day history of fever and swelling of the left upper and lower eyelids associated with pain, watering, and difficulty in opening the eyelids. He reported that his sheep had died suddenly 1 week prior to his illness. There was no past history of any medical illness. The patient reported that he was prescribed tablets and injections by a general practitioner, but was unable to provide details of this treatment to us.
On examination, there was brawny nonpitting edema of the upper and lower eyelids of the left eye and left side of the face (). There was an ulceration and black discoloration along the left lower lid margin with serosanguinous discharge. His visual acuity was 20/20 in both the eyes. The anterior and posterior segments of both the eyes were within normal limits. A diagnosis of oculocutaneous anthrax was considered based on the history and clinical findings. Serous fluid from the eyelid and blood were collected and sent for conventional cultural methods and polymerase chain reaction (PCR) test. The Gram stain of the serous fluid revealed no leucocytes or bacteria. Cultures of the serous fluid and blood were negative for B. anthracis.
Figure 1 Brawny nonpitting edema of the upper and lower eyelids of the left eye with serosanguinous discharge

PCR method for the detection of B. anthracis
The patient’s DNA was extracted using the QIA amp DNA blood mini kit (QIAGEN, Hilden, Germany) according to the manufacturer’s instruction. A 596-bp fragment of the protective antigen (PA) gene, PA (F)-TCC TAA CAC TAA CGA AGT CG and PA (R)-GAG GTA GAA GGA TAT ACG GT and a 846-bp fragment of the capsule (CAP) gene, CAP (F)-CTG AGC CAT TAA TCG ATA TG and CAP (R)Citation2,Citation3 of B. anthracis were used as the target for anthrax PCR. The DNA was amplified in a total volume of 50 μL with the above mentioned primers, 200 μm (each) deoxynucleotide triphosphates, 1X PCR buffer, 1.5 mM MgCL2 and 2.5 units of Taq polymerase (Amplitaq Gold-Applied Biosystems, California, USA) and followed by the addition of 5 μL of the template DNA. Thermal cycling was performed at 94°C for 5 minutes (initial denaturation) followed by 35 cycles at 94°C for 1 minute, 52°C for 1 minute (annealing), 72°C for 2 minutes (extension) and the final extension at 72°C for 5 minutes; cooled to 4°C.Citation4 Thermal cycling was done in the Gene AMP PCR system 9200 (Applied Biosystems, California, USA).
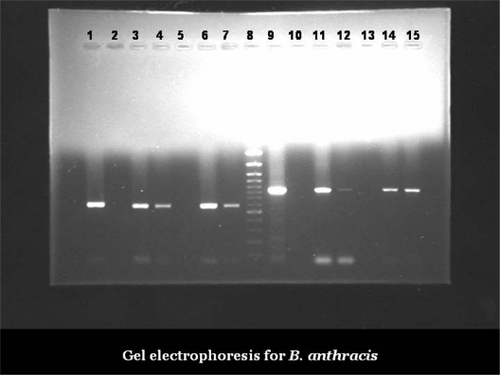
A 15 μL portion of the PCR product and 5 μL of 10% tracking dye (0.02% xylene cyanol, 0.02% bromophenol blue and 50% glycerol) was added to the PCR tube. Fifteen microliters of this mix were loaded into the wells in the agarose (Amersham Pharmacia, New Jersey, USA). The PCR products were analyzed by submarine gel electrophoresis through a 1% agarose gel in 1X TAE buffer. The gel was run at 120 volts for 60 minutes, stained with 0.5 μg/mL of ethidium bromide (Amersham Pharmacia, New Jersey, USA), visualized and recorded under UVCitation4 in the Gel Doc 2000 System (Bio-Rad, California, USA). The Gene Ruler™ 100-bp (3000–100bp) DNA Ladder Plus (MBI Fermentas, USA) was used as the molecular standard. The PCR from the fluid and the blood were positive for the gene encoding the protective antigen (PA gene) and the capsule (CAP gene) of B. anthracis ().
Figure 2 Gel electrophoresis for B. anthracis.
Clinical course of the patient
The patient was started on injection crystalline penicillin, 2 million international units (1250 mg) every 2 hours intravenously. No topical therapy was prescribed, however, the patient was given anti-inflammatory agents (ibuprofen). The patient responded well to antibiotic therapy with reduction of fever and lid edema. A black eschar developed within a few days of treatment (). On completion of a 10-day course of intravenous antibiotics, he was discharged on oral penicillin G 500 mg every 6 hours. The total duration of antibiotic therapy including intravenous antibiotics was 6 weeks. Although the eschar reduced in size over time, it was firmly adhered to the underlying tissue. When the eschar was removed after 1 month of the onset of illness, an ulcerated undersurface was observed (). The ulceration healed over the next 2 weeks with scarring and ectropion of the left lower lid (). The low grade lid edema and mechanical ptosis of the left upper eyelid resolved over the next few weeks.
Figure 3 Black eschar involving the left lower lid with residual edema of the left upper lid.

Figure 4 Ulcerated undersurface of the left lower lid on removal of the eschar.

Figure 5 Scarring and ectropion of the left lower lid.

Comments
B. anthracis is commonly found in agricultural environments. It is a Gram-positive, aerobic, endospore-forming bacilli that, in the vegetative form, has a poor survival rate outside an animal or human host.Citation5 It is capable of producing fatal infection in livestock and in humans.Citation1 Anthrax is considered to be one of most dangerous biological weapons.Citation6 Humans are infected when spores are introduced into the body by contact with infected animals or animal products.Citation1 Cutaneous anthrax has been reported to occur as preseptal cellulitis in the eyelids.Citation7,Citation8 Cutaneous anthrax, if untreated, leads to life-threatening septicemia.Citation1
This report highlights that a high index of clinical suspicion and prompt institution of appropriate therapy are essential for a successful outcome. Since lesions can become sterile within 24 hours of antimicrobial therapy, confirmation of diagnosis can be made using PCR,Citation2–Citation4,Citation9 as was done in our patient, when the conventional cultural methods fail to identify the etiology or when patients have already received antimicrobial therapy.
Acknowledgements
SD-study conception, acquisition of data and photographs, literature review, critical appraisal of the write up, and approval of the final version of the manuscript; JP-literature review, write up of the article, and approval of the final version of the manuscript; RR-literature review, acquisition of data and photographs, critical appraisal of the article, and approval of the final version of the manuscript; PP-microbiological aspects and approval of the final version of the manuscript; PM-microbiological aspects, critical appraisal of the write up, and approval of the final version of the manuscript.
Disclosures
The authors report no conflicts of interest in this work.
References
- SpencerRCBacillus anthracisJ Clin Pathol20035618218712610093
- BeyerWGlocknerPOttoJBohmRA nested PCR and DNA amplification fingerprinting method for detection and identification of B. anthracis in soil samples from former tanneriesSalisbury Med Bull199687Suppl4749
- HutsonRADugglebyCJLoweJRMancheeRJTurnbullPCThe development and assessment of DNA and oligonucleotide probes for the specific detection of B. anthracisJ Appl Bacteriol1993754634728300447
- TurnbullPCBGuidelines for the surveillance and control of anthrax in humans and animals3rd edWorld Health OrganizationGeneva, (WHO/EMC/ZDI/98.6) 19986062
- PetskoGAWinter, plague and pestilenceGenome Biol20012:COMMENT1013. Epub 2001 Oct 23.
- InglesbyTVO’TooleTHendersonDAAnthrax as a biological weapon: Updated recommendations for managementJAMA20022872236225211980524
- CelebiSAykanUAlagozGEsmerligilSPalpebral anthraxEur J Ophthalmol20011117117411456020
- SoysalHGKiratliHRecepOFAnthrax as a cause of preseptal cellulitis and cicatricial ectropionActa Ophthalmol Scand20017920820911284766
- HadjinicolaouAVDemetriouVLHezkaJBeyerWHadfieldJLKostrikisLGUse of molecular beacons and multiallelic real-time PCR for detection of and discrimination between virulent Bacillus anthracis and other Bacillus isolatesJ Microbiol Methods200978455319379778