Abstract
We report the first case in the literature of Kyrieleis’ vasculitis related to acute retinal necrosis by Varicella zoster virus in a 76-year-old woman with bilateral involvement. In our patient the arterial lesions appeared 15 days after the initial presentation.
Kyrieleis’ vasculitisCitation1 is a rare condition in which white-yellowish exudates are placed in a beaded pattern within the retinal arteries.Citation2 It is predominantly associated with toxoplasma infection but has been described in tuberculosis, syphilis, and mediterranean spotted fever.Citation3,Citation4 We describe a patient who developed Kyrieleis’ plaques in the setting of an acute retinal necrosis.
A 76-year-old white immunocompetent woman presented with red eye, floaters and blurry vision in her left eye for one week. Visual acuity was 0.5 LogMAR, anterior uveitis with granulomatous keratic precipitates, vitreitis, and patchy white multifocal and confluent areas in the mid and far periphery of the retina (). Polymerase chain reaction of aqueous was positive for Varicella zoster virus (VZV). We started treatment with oral valacyclovir, intravitreous foscarnet injections, and retinal photocoagulation of the necrotic areas (). In spite of those treatments the right eye was affected one week later. Segmental arteritis with Kyrieleis’ plaques ( and ) were observed in both eyes with associated cicatricial retinitis two weeks later. Final visual acuity was 0.60 LogMAR in left eye and 0.30 LogMAR in right eye.
Figure 1 Montage photo of initial presentation with large confluent areas of retinal necrosis.
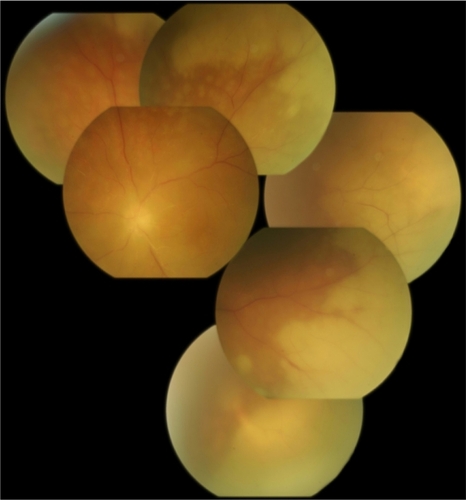
Figure 2 Montage photo after laser photocoagulation.
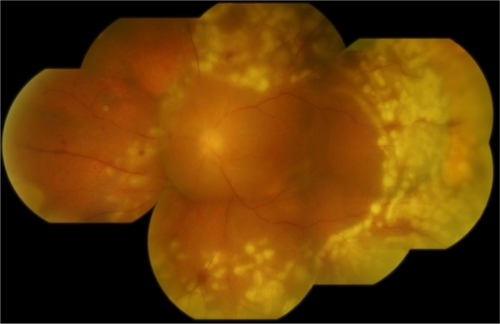
Figure 3 Kyrieleis’ pattern of arteritis is present as white plaques within the artery that appear nodular and do not extend outside the vessel.
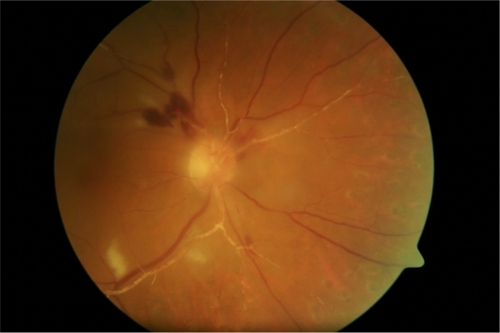
Figure 4 Magnification of Kyrieleis’ plaques within the arteries.

To our knowledge this is the first report of Kyrieleis’ vasculitis in acute retinal necrosis by VZV. Kyrieleis’ plaques are always associated with inflammation. Its presence reflects the severe intraocular inflammation experienced by the eye, but it does not worsen the prognosis. It is difficult to explain the “segmental arteritis”, Griffin and Bodian believed the plaques on the vessels possibly represented migration of exudates from the active choroiditis to the periarterial sheaths.Citation5 However, this does not seem feasible because the vessels are not sheathed. As there is no pathological study available in the literature, the nature of the beads is still unknown. In our patient the arterial lesions appeared about 15 days after the initial presentation. It is possible that they may represent an immunological response to an infectious agent resulting in the deposition of immune cells and/or inflammatory debris within or adjacent to the vessel wall.
Disclosure
No conflicts of interest were declared in relation to this paper.
References
- KyrieleisWUber atypische gerfaesstuberkulose der netzhautArch Augenheilkd1933107182190
- JainISSingKSegmental arteritisIndian J Ophthalmol196614229231
- KrishnamurthyRCunninghamETAtypical presentation of syphilitic uveitis associated with Kyrieleis plaquesBr J Ophthalmol2008921152115318653612
- KhairallahMLadjimiAChakrounMPosterior segment manifestations of Rickettsia conorii infectionOphthalmol2004111529534
- GriffinAOBodianMSegmental retinal periarteritis: a report of three casesAm J Ophthalmol19594754413637172