Abstract
Therapeutic methods directed at alleviating the basic pathological processes of normal-tension glaucoma (NTG) are yet to be established. Although there seems to be little doubt that intraocular pressure (IOP) represents a risk factor in most patients, reduction of IOP does not prevent progression in every patient with NTG, indicating that factors other than elevated IOP are involved in glaucoma progression. New avenues of treatment under investigation include agents that could improve blood flow to the eye and neuroprotective drugs. The major components of the renin-angiotensin system have been identified in ocular tissue. Angiotensin-converting enzyme (ACE) inhibitors are widely used to treat systemic hypertension. ACE inhibitors are inhibitors of kininase II and thus prevent breakdown of bradykinin. Bradykinin displays protective actions against glutamate neurotoxicity through bradykinin-B2 receptors in cultured retinal neurons. ACE inhibitors blocked the liberation of angiotensin II from angiotensin I. Lower angiotensin II levels may have beneficial effects on outcomes by lowering vascular superoxide anion production. The effects of ACE inhibitor as a potential antiglaucoma therapy deserve intense scrutiny.
Introduction
Normal-tension glaucoma (NTG) refers to a glaucomatous optic nerve head change and corresponding glaucomatous visual field defects without elevated intraocular pressure (IOP). A long-term collaborative study conducted in North America and Europe revealed that a 30% reduction in IOP exerted positive effects on the progression of visual field loss in NTG (CitationCollaborative Normal-Tension Glaucoma Study Group 1998a). Treatment goals for open-angle glaucoma have focused almost exclusively on lowering IOP using drugs, laser therapy or surgery. However, many investigators believe that IOP is not the only factor causally related to glaucomatous optic nerve changes and that some factors unrelated to IOP play significant roles in at least some NTG cases. Patients with glaucoma in whom IOP is lowered to within normal range often continue to suffer further progressive damage (CitationMao et al 1991; CitationNouri-Mahdavi et al 1995). A recent 10-year follow-up study showed a direct correlation between IOP levels and stabilization of the optic disc and visual field (CitationAraujo et al 1995). Still, 10% of patients in that study with a mean final IOP of 13 mmHg continued to show disease progression.
The association of glaucoma with various systemic vascular diseases including low systemic blood pressure, transient nocturnal decreases in blood pressure, hypertension, migraine, vasospasm and diabetes has been reported (CitationFlammer et al 1999; CitationHayreh 1999; CitationBonomi et al 2000; CitationDrance et al 2001). Many patients with chronic open-angle glaucoma present with coexisting vascular disorders, the most common of which is systemic hypertension, which occurs in 48% of the total chronic open-angle glaucoma population (CitationGottfredsdottir et al 1997). Pharmacological treatment of non-IOP-dependent mechanisms in glaucoma has largely been limited to the use of calcium-channel blockers, which are widely used in the treatment of systemic hypertension, coronary artery diseases, stroke and arrhythmias. The jury is still out on the contrasting results for systemic calcium-channel blockers used on human glaucoma patients. Calcium-channel blockers may increase blood flow to the optic nerve head (CitationTomita et al 1999) and might be particularly useful in patients with NTG (CitationNetland et al 1993; CitationKancllopoulos et al 1996). However, one study showed no significant difference in progression of glaucoma in patients using or not using systemic calcium-channel blockers (CitationLiu et al 1996). Systemic calcium channel blockers can also have adverse cardiac effects, particularly if the patient is being treated with topical β-blockers (CitationKancllopoulos et al 1996).
Neuroprotection refers to the post-injury protection of neurons that were initially undamaged or only marginally damaged by a particular insult, but are at risk from toxic stimuli released by damaged cells, causing secondary degeneration (CitationYoles and Schwartz 1998). Secondary degeneration refers to the spread of degeneration to apparently healthy neurons that escape the primary insult, but are adjacent to injured neurons and thus exposed to the degenerative milieu that results (CitationYoles and Schwartz 1998).
Renin-angiotensin system
The renin-angiotensin system (RAS) plays an important role in vasoconstriction, regulation of electrolyte balance and vascular remodeling. Local renin-angiotensin regulation is present in the eye (CitationDanser et al 1994; CitationWagner et al 1996). Since the initial application of angiotensin-converting enzyme (ACE) inhibitors as therapeutic agents for the treatment of hypertension, several additional clinical indications have been identified and approved (CitationBrown and Vaughan 1998). ACE inhibitor activity reportedly improves endothelial function and stimulates vascular remodeling, in addition to attenuating progression of arteriosclerosis and the occurrence of cardiovascular events in humans (CitationMancini et al 1996; CitationYusuf et al 2000). The identification of ACE as a signaling molecule, which can be activated by the binding of ACE inhibitor, may account for some of the beneficial effects of this class of compounds on the cardiovascular system.
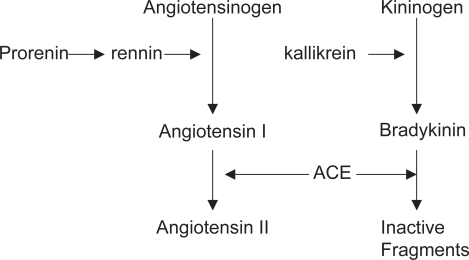
The RAS is an enzymatic cascade that generates a range of angiotensin peptides with varying biological actions. Definitive evidence that an RAS exists within the eye has been provided by molecular biological techniques such as real-time PCR and RNAse protection assays, which have revealed that components of the RAS are synthesized in ocular tissue. Renin is expressed in the pigmented epithelium and retinal Müller cells (CitationBerka et al 1995; CitationWagner et al 1996). Angiotensinogen is the sole precursor of angiotensin peptides and is cleaved to generate angiotensin I by renin and aspartyl proteases (). Angiotensin II can be liberated from angiotensin I by ACE or serine proteases. Angiotensin II is the main effector peptide of the RAS and acts on two main receptor subtypes: angiotensin type I (AT1); and angiotensin type II (AT2). Gene expression for AT1 and AT2 receptors has been identified in several ocular tissues, including the retina (CitationBrandt et al 1994; CitationMurata et al 1997; CitationWheeler-Schilling et al 1999; CitationSarlos et al 2003). AT1 receptors have been localized to the ganglion cell layer and inner nuclear layer in rat retina (CitationWheeler-Schilling et al 1999). AT1 receptor elicits most of the known physiological actions of angiotensin II, including vasoconstriction, electrolyte homeostasis, modulation of drinking behavior and stimulation of pituitary hormone release (CitationCulman et al 1995; CitationIto et al 1995; CitationAguilera and Kiss 1996). In tissue pathology such as cardiovascular disease, nephropathies, liver cirrhosis and cancer, AT1 receptor is implicated in a wide variety of cell events including cell growth, differentiation and migration, fibrosis and inflammation and angiogenesis (CitationYoshiji et al 2001; CitationYoshiji et al 2002; CitationBrewster et al 2003; CitationGilbert et al 2003; CitationMuller et al 2003). Actions of the AT2 receptor are less well defined, but possibly oppose actions of the AT1 receptor, including vasodilation and apoptosis (CitationChung et al 1998). However, evidence in a number of tissues suggests that the AT2 receptor displays similar actions to the AT1 receptor, promoting cell growth and angiogenesis (CitationLevy et al 1996; CitationCao et al 2000; CitationSarlos et al 2003).
The kallikrein-kinin system
In general, the kallikrein-kinin system is thought to counterbalance the activities of the RAS. Kinin peptides are generated from kininogens by kallikrein, a serine protease (). The actions of kinin peptides include promoting inflammation, leakage of plasma proteins, pain and more recently, angiogenesis.
Components of the kallikrein-kinin system have been identified in the eye. Kallikrein and kininase II activity are found in the retina, choroid and ciliary body of swine eyes, with the highest activity of kininase I in aqueous humor (CitationIgic 1985). Bradykinin is a vasodilating nonapeptide that is degraded by ACE (CitationHornig and Drexler 1997). Plasma bradykinin levels are increased in patients treated with ACE inhibitor (CitationCugno et al 2005). Bradykinin displays a wide range of actions, mediated through at least two subtypes of receptor: B1 and B2 (CitationRegoli and Barabe 1980). B1 receptor has been implicated in angiogenesis, as bradykinin stimulates endothelial cell proliferation in vitro via activation of the B1 receptor cAMP pathway (CitationMorbiddelli et al 1998). Most biological actions are mediated by B2 receptors. Bradykinin-B2 receptors are reportedly abundantly distributed in vascular tissues and smooth muscles cell, and also in human brain (CitationRaidoo et al 1996) and retinal (CitationMa et al 1996) neurons. In human retina, tissue kallikrein, low molecular weight kininogen and B1 and B2 receptors are expressed in neuronal cells of the outer nuclear layer, inner nuclear layer and ganglion cell layer, and on the retinal vasculature (CitationMa et al 1996). In addition, mRNA for the B2 receptor has been identified in the retinal ganglion cell layer and in a population of cells adjacent to the sclerocorneal junction in rats (CitationTakeda et al 1999). In B2 receptor-deficient mice with hindlimb ischemia, ACE inhibition increased vessel density and capillary number in the ischemic leg (CitationSilvestre et al 2001). This was not observed in the ischemic hindlimb of mice lacking B2 receptor (CitationSilvestre et al 2001).
Blood flow
AT1 receptor antagonist ameliorates impaired optic nerve head blood flow in rabbits (CitationInoue et al 2003). The decreased flow velocity in hypertensive patients improved with an oral ACE inhibitor (CitationSteigerwalt et al 1998). ACE inhibitor may act in several ways to increase the blood flow in the eye. The L-arginine nitric oxide pathway is an important local regulator of vascular tone. In the ophthalmic circulation, bradykinin is a potent activator of this pathway, and it causes pronounced endothelium-dependent relaxations in isolated blood vessels (CitationYao et al 1991; CitationHaefliger et al 1992, Citation1994), which releases nitric oxide through B2 receptors (CitationMeyer et al 1995), and increases in ophthalmic flow in the isolated perfused eye (CitationMeyer et al 1993). Stimulation of the L-arginin nitric oxide pathway by bradykinin not only leads vasodilation but also to the inhibition of migration (CitationNyborg et al 1990) and proliferation of vascular smooth muscle cells (CitationGarg and Hassid 1989; CitationDubey 1994).
It must be emphasized that angiotensin II is also assumed to play a role in cerebral myogenic autoregulation (CitationStrandgaard and Paulsen 1992). Myogenic autoregulation may also be present in the choroidal vasculature (CitationKiel 1994). Hence angiotensin receptor blockade may be useful to prevent abnormal cerebral and ocular autoregulation in patients with activated RAS.
ACE inhibitors and diabetic retinopathy
Diabetic retinopathy is a major cause of blindness in those of working age (CitationGoldstein et al 1993). Diabetic retinopathy progresses from a mild non-proliferative form characterized by vascular permeability to moderate or severe non-proliferative diabetic retinopathy in which retinal vessels close, and finally to proliferative diabetic retinopathy that comprises new blood vessel growth typically between the retina and posterior surface of the vitreous.
Angiotensin II is a known stimulus for the expression of vascular endothelial growth factor (VEGF), which is associated with the induction of retinal neovascularization (CitationAiello et al 1995; CitationGilbert et al 1998; CitationOtani et al 2000; CitationOkada et al 2001). Vitreous levels of both angiotensin II and VEGF are significantly higher in eyes with active proliferative diabetic retinopathy (PDR) than in eyes with quiescent PDR, suggesting that upregulated angiotensin II may be involved in the progression of neovascularization (CitationFunatsu et al 2002). In experimental diabetic models, inhibition of angiotensin II formation with ACE inhibition results in suppression of VEGF expression (CitationMoravski et al 2000; CitationHiggins et al 2003). Vitreous VEGF levels were higher in patients with PDR than in patients without diabetes, but these high levels were significantly reduced after ACE inhibitor treatment (CitationHogeboom et al 2002). A growing number of both clinical and experimental studies suggest that inhibition of the RAS can provide protective effects against diabetic retinopathy in the absence of hypertension. The most widely cited clinical evidence for a role of the RAS in diabetic retinopathy in the absence of hypertension was produced in the EURODIAB Controlled Trial of Lisinopril in Insulin-Dependent Diabetic Mellitus study (EUCLID), which reported that ACE inhibition with lisinopril reduced progression of retinopathy in type I diabetic patients who were normotensive (CitationChaturvedi et al 1998). This 2-year multicenter study showed that progression of retinopathy was reduced by at least one level in the lisinopril-treated group compared with that in placebo-treated control individuals after adjustment for center. This study also showed a decreased rate of progression to PDR in the lisinopril-treated group after adjustment for glycemic control. At 1 month, mean diastolic blood pressure was 74 mmHg for the lisinopril-treated group and 77 mmHg in the placebo group and this difference was maintained over the course of study (CitationEUCLID Study Group 1997). The normotensive Appropriate Blood Pressure Control in Diabetes (ABCD) study compared the effects on progression of diabetic retinopathy obtained with moderate and intensive control of blood pressure in normotensive type 2 diabetic patients treated with enalapril or nisoldipine (CitationSchrier et al 2002). Follow-up blood pressure was 128 mmHg for the intensive treatment group and 137 mmHg for the moderate control group. At 5 years, this prospective study showed that progression of diabetic retinopathy was 34% in the intensively treated group, compared with 46% in the moderately treated group. No significant difference in response was seen between enalapril- and nisoldipine-treated patients. These results showed that a decrease in blood pressure in normotensive patients with type 2 diabetes was associated with reductions in progression of diabetic retinopathy. The results of both the EUCLID and normotensive ABCD studies show significant beneficial effects of ACE inhibition on progress of diabetic retinopathy in diabetic patients in the absence of hypertension, but the mechanisms that contribute to this response have yet to be identified. Both studies reported a significant reduction in systemic blood pressure. These results may suggest that reduction of blood pressure within the normotensive range could contribute to the decreases in progression of diabetic retinopathy. However, inhibition of the RAS has also been shown to effect a number of circulating factors, including reactive oxygen species and inflammatory cytokines, which could indirectly contribute to vascular effects (CitationKoh et al 2003). In addition, mechanical stretch can activate the AT1 receptor (CitationZou et al 2004) and upregulate the VEGF pathway in retinal endothelial cells (CitationSuzuma et al 2001), suggesting that blood pressure itself may affect actions of the AT1 receptor. The relative contributions of reduced systemic blood pressure within the normotensive range and other systemic or local ocular effects of RAS inhibitors to the progression of diabetic retinopathy remain unknown.
Potential use of ACE inhibitors in glaucoma treatment
Elevated IOP is the most important risk factor for glaucomatous damage, but it is still only a risk factor. Visual damage in glaucoma results from a combination of elevated IOP and IOP-independent risk factors. Although hypothesizing that NTG has an underlying mechanism independent of IOP is tempting, use of hypotensive treatment strategies does appear to slow the progression of NTG (CitationCollaborative Normal-Tension Glaucoma Study Group 1998a). However, the findings of the Collaborative Normal Tension Glaucoma Study Group showed no significant association between mean IOP change and visual field progression (CitationCollaborative Normal-Tension Glaucoma Study Group 1998a; CitationCollaborative Normal-Tension Glaucoma Study Group 1998b).
Even more recently, application of neuroprotection to the treatment of non-IOP-dependent glaucomatous damage has received increasingly intensive attention. If glaucoma is actually a collection of diseases that all result in a common optic neuropathy, therapy aimed at preventing the process of damage would show enormous therapeutic potential.
ACE inhibitors have recently attracted attention as a new class of drugs for the treatment of glaucoma. ACE inhibitors have been shown to lower IOP in patients with ocular hypertension or primary open-angle glaucoma (CitationConstad et al 1988). Lotti and Pawlowski (CitationLotti and Pawlowski 1990) proposed the involvement of prostaglandins in the ocular hypotensive effect of enalaprilat. This conclusion was based on the finding that indomethacin blocked the IOP-lowering effect of enalaprilat. ACE inhibitors are also inhibitors of kininase II and thus prevent the breakdown of bradykinin. Increased bradykinin levels promote prostaglandin synthesis. Prostaglandin, particularly PGF2α, is known to increase uveoscleral outflow of aqueous humor (CitationCrawford and Kaufman 1987).
Apoptosis has been shown to be at least one of the mechanisms for retinal ganglion cell death in monkey models of pressure-induced glaucoma (CitationQuigley et al 1995). Evidence for apoptosis in Alzheimer’s disease has been provided from both animal models and human materials (CitationSchmechel 1999). Longitudinal intervention studies for hypertension, such as the Systolic Hypertension in Europe (SYST-EUR) study and the Peridopril Protection Against Recurrent Stroke Study (PROGRESS) trial, have reported a significant inverse relationship between antihypertensive treatments and risk of vascular-related dementia (CitationForette et al 2002; CitationTzourio et al 2003). For example, SYST-EUR data from the 8-year follow-up phase of the program have suggested a 55% reduction in risk for dementia during long-term active treatment with the ACE inhibitor enalapril (CitationForette et al 2002). Similarly, the PROGRESS study indicated that a substantially reduced risk for dementia (34%) was confirmed by treatment with the ACE inhibitor perindopril. Long-term use of ACE inhibitors may have a protective role against the development of Alzheimer’s disease (CitationOhrui et al 2004).
Bradykinin has a protective action against glutamate neurotoxicity through bradykinin-B2 receptors in cultured retinal neurons (Yasuyoshi et al 2004). We have previously reported that NTG patients were more sensitive to exogenous bradykinin than normal subjects (CitationHirooka et al 2002). These data suggest that endogenous bradykinin levels may be lower in NTG patients than in normal subjects. Angiotensin I-converting enzyme and endothelial cell kininase are thought to represent one and the same enzyme (CitationMombouli and Vanhoutte 1995). As a kininase, this enzyme is responsible for the degradation of bradykinin. ACE inhibitors are thus capable of prolonging the half-life of any bradykinin in the proximity of endothelium. Long-term treatment with ACE inhibitors increases plasma bradykinin levels (CitationCugno et al 2005). CitationYasuyoshi et al (2000) recently reported that bradykinin has protective effects on neurotoxicity induced by glutamate through bradykinin B2 receptors in cultured retinal neurons. The protective action of bradykinin is mediated by the opening of the mitochondrial adenosine triphosphate-sensitive potassium channel (CitationYamauchi et al 2003).
Inhibition of bradykinin degradation by ACE inhibitors may increase the activity of superoxide dismutase and modulate the production of nitric oxide, leading to the inactivation of reactive oxygen species, while also inhibiting various pro-oxidative mechanisms within the vasculature (CitationEhring et al 1994). Lower angiotensin II levels, such as seen during treatment with ACE inhibitor, may have beneficial effects on outcome by lowering vascular superoxide anion production (CitationRajagopalan and Harrison 1996). ACE inhibitor may benefit vascular function. A previous study reported average rates of decline in NTG as −0.41 dB per year (CitationAnderson et al 2001) with a mean follow-up of 4.5 years. In subjects with a significant decline, mean rate of loss across the entire field was −0.90 dB/year (CitationAnderson et al 2001). In subjects who had not progressed, mean rate of loss across the entire field was −0.14 dB/year (CitationAnderson et al 2001). We retrospectively reviewed a total of 38 patients with NTG (CitationHirooka et al 2006), divided into 3 groups: control subjects with no previous history of hypertension; NTG hypertension patients receiving ACE inhibitor; and NTG hypertension patients receiving other antihypertensive drug treatment. In the ACE inhibitor-treated group, mean deviation (MD) change per year was 0.48 ± 0.19 dB, compared to −0.38 ± 0.23 dB in control subjects, and −0.50 ± 0.39 dB in the other antihypertensive drug-treated group. These results suggest that ACE inhibitors might exert favorable effects on the visual field in patients with NTG (CitationHirooka et al 2006). ACE inhibitors have numerous properties that theoretically should be beneficial in treating non-IOP-dependent mechanisms in glaucoma.
Randomized, controlled clinical trials have not been performed to clarify neuroprotective effects of ACE inhibitors in glaucoma yet. In the absence of such trials, further studies in various animal models of glaucoma are also needed.
References
- AguileraGKissA1996Regulation of the hypothalamic-pituitary-adrenal axis and vasopressin secretion. Role of angiotensin IIAdv Exp Med Biol396105128726690
- AielloLPPierceEAFoleyED1995Suppression of retinal neovascularization in vivo by inhibition of vascular endothelial growth factor (VEGF) using soluble VEGF-receptor chimeric proteinsProc Natl Acad Sci USA9210457617479819
- AndersonDRDranceSMSchulzerMCollaborative Normal-Tension Glaucoma Study Group2001Natural history of normal-tension glaucomaOphthalmology1082475311158794
- AraujoSVSpaethGLRothSM1995A ten-year follow-up on a prospective, randomized trial of postoperative corticosteroids after trabeculectomyOphthalmology102175399098274
- BerkaJLStubbsAJWangDZ1995Renin-containing Müller cells of the retina display endocrine featuresInvest Ophthalmol Vis Sci36145087775123
- BonomiLMarchiniGMarraffaM2000Vascular risk factors for primary open angle glaucoma: the Enga-Neumarkt StudyOphthalmology10712879310889099
- BrandtCRPumferyAMMicalesB1994Renin mRNA is synthesized locally in rat ocular tissuesCurr Eye Res13755637531130
- BrewsterUCSetaroJFPerazellaMA2003The rennin-angiotensinaldosterone system: cardiorenal effects and implications for renal and cardiovascular diseases statesAm J Med Sci326152412861121
- BrownNJVaughanDE1998Angiotensin-converting enzyme inhibitionsCirculation971411209577953
- CaoZKellyDJCoxA2000Angiotensin type 2 receptor is expressed in the adult rat kidney and promotes cellular proliferation and apoptosisKidney Int5824375111115077
- ChaturvediNSjolleAKStephensonJM1998Effect of lisinopril on progression of retinopathy in normotensive people with type I diabetes. The EUCLID Study Group. EURODIAB Controlled Trial of Lisinopril in Insulin-Dependent Diabetes MellitusLancet35128319433426
- ChungOKuhlHStollM1998Physiological and pharmacological implications of AT1 versus AT2 receptorsKidney Int Suppl67S9599736262
- Collaborative Normal-Tension Glaucoma Study Group1998aComparison of glaucomatous progression between untreated patients with normal-tension glaucoma and patients with therapeutically reduced intraocular pressuresAm J Ophthalmol12648797
- Collaborative Normal-Tension Glaucoma Study Group1998bThe effectiveness of intraocular pressure reduction in the treatment of normal-tension glaucomaAm J Ophthalmol126498505
- ConstadWHFiorePSamsonC1988Use of an angiotensin converting enzyme inhibitor in ocular hypertension and primary open-angle glaucomaAm J Ophthalmol10567473287943
- CrawfordKKaufmanPL1987Pilocarpine antagonizes prostaglandin F2α-induced ocular hypotension in monkeys. Evidence for enhancement of Uveoscleral outflow by prostaglandin F2αArch Ophthalmol1051112163477218
- CugnoMAgostoniPMariD2005Impaired bradykinin response to ischaemia and exercise in patients with mild congestive heart failure during angiotensin-converting enzyme treatment. Relationships with endothelial function, coagulation and inflammationBr J Haematol1301132015982353
- CulmanJHohleSQadriF1995Angiotensin as neuromodulator/neurotransmitter in central control of body fluid and electrolyte homeostasisClin Exp Hypertens17281937735275
- DanserAHDerkxFHAdmiraalPJ1994Angiotensin levels in the eyeInvest Ophthalmol Vis Sci351008188125711
- DranceSAndersonDRSchulzerMCollaborative Normal-Tension Glaucoma Study Group2001Risk factors for progression of visual field abnormalities in normal-tension glaucomaAm J Ophthalmol13169970811384564
- DubeyRK1994Vasodilator-derived nitric oxide inhibits fetal calf serum- and angiotensin-II-induced growth of renal anterior smooth muscle cellsJ Pharm Exp Ther2694028
- EhringTBaumgartDKrajcarM1994Attenuation of myocardial stunning by the ACE inhibitor ramiprilat through a signal cascade of bradykinin and prostaglandins but not nitric oxideCirculation901368858087948
- FlammerJHaefligerIOOrgulS1999Vascular dysregulation: a principal risk factor for glaucomatous damage?J Glaucoma8212910376264
- ForetteFSeuxMLStaessenJA2002The prevention of dementia with antihypertensive treatment: new evidence from the Systolic Hypertension in Europe (Syst-Eur) studyArch Inter Med162204652
- FunatsuHYamashitaHNakanishiY2002Angiotensin II and vascular endothelial growth factor in the vitreous fluid of patients with proliferative diabetic retinopathyBr J Ophthalmol86311511864890
- GargUCHassidA1989Nitric oxide-generating vasodilators and 8-bromo-cyclic guanosine monophosphate inhibit mitogenesis and proliferation of cultured rat vascular smooth muscle cellsJ Clin Invest83177472540223
- GilbertREKrumHWilkinson-BerkaJ2003The rennin-angiotensin system and the long-term complications of diabetes: pathophysiological and therapeutic considerationDiabet Med206072112873287
- GilbertREVranesDBerkaJL1998Vascular endothelial growth factor and its receptors in control and diabetic rat eyesLab Invest781017279714188
- GoldsteinDEBlinderKJIdeCH1993Glycemic control and development of retinopathy in youth-onset insulin-dependent diabetes mellitus. Results of a 12-year longitudinal studyOphthalmology1001125318341491
- GottfredsdottirMSAllinghamRRShieldsMB1997Physicians’ guide to interactions between glaucoma and systemic medicationsJ Glaucoma6377839407366
- HaefligerIOFlammerJLüscherTF1992Nitric oxide and endothelium-1 are important regulators of human ophthalmic arteryInvest Ophthalmol Vis Sci33234031607246
- HaefligerIOMeyerPFlammerJ1994The vascular endothelium as a regulator of the ocular circulation: A new concept in ophthalmology?Surv Ophthalmol39123327801220
- HayrehSS1999The role of age and cardiovascular diseases in glaucomatous optic neuropathySurv Ophthalmol43S274210416745
- HigginsRDYanYGengY2003Captopril and vascular endothelial growth factor in a mouse model of retinopathyCurr Eye Res27123914632165
- HirookaKShiragaFHasegawaE2002Bradykinin sensitivity in primary open-angle glaucoma and normal-tension glaucoma patientsAm J Ophthalmol134922412470771
- HirookaKBabaTFujimuraT2006Prevension of visual field defect progression with angiotensin-converting enzyme inhibitor in eyes with normal-tension glaucomaAm J Ophthalmol142523516935614
- Hogeboom van BuggenumIMPolakBCReichert-ThoenJW2002Angiotensin converting enzyme inhibiting therapy is associated with lower vitreous vascular endothelial growth factor concentrations in patients with proliferative diabetic retinopathyDiabetologia45203911935151
- HornigBDrexlerH1997Endothelial function and bradykinin in humansDrugs544279429844
- IgicR1985Kallikrein and kininases in ocular tissuesExp Eye Res41117202993009
- ItoMOliverioMIMannonPJ1995Regulation of blood pressure by the type 1A angiotensin II receptor geneProc Natl Acad Sci USA92352157724593
- InoueTYokoyamaTKoikeH2003CS-088, an angiotensin type 1 receptor antagonist, ameliorated the impaired blood flow in the optic nerve head of rabbitOphthalmic Res35351414688427
- KanellopoulosAJEricksonKANetlandPA1996Systemic calcium channel blockers and glaucomaJ Glaucoma5357628897236
- KielJW1994Choroidal myogenic autoregulation and intraocular pressureExp Eye Res58529437925690
- KohKKAhnJYHenSH2003Pleiotropic effects of angiotensin II receptor blocker in hypertensive patientsJ Am Coll Cardiol429051012957441
- LevyBIBenessianoJHenrionD1996Chronic blockade of AT2-subtype receptors prevents the effect of angiotensin II on the rat vascular structureJ Clin Invest98418258755652
- LiuSAraujoSVSpaethGL1996Lack of effect of calcium channel blockers on open-angle glaucomaJ Glaucoma5187908795757
- LottiVJPawlowskiN1990Prostaglandins mediate the ocular hypotensive action of the angiotensin converting enzyme inhibitor MK-422 (enalaprilat) in African green monkeysJ Ocul Phalmacol617
- MaJXSongQHatcherHC1996Expression and cellular localization of the kallikrein-kinin system in human ocular tissuesExp Eye Res6319268983960
- ManciniGBHenryGCMacayaC1996Angiotensin-converting enzyme inhibitor with quinapril improves endothelial vasomotor dysfunction in patients with coronary artery disease. The TREND (Trial on Reversing ENdothelial Dysfunction) StudyCirculation94258658759064
- MaoLKStewartWCShieldsMB1991Correlation between intraocular pressure control and progressive glaucomatous damage in primary open-angle glaucomaAm J Ophthalmol1115151985490
- MeyerPFlammerJLüscherTF1993Endothelium-dependent regulation of the ophthalmic microcirculation in the perfused porcine eye: Role of nitric oxide and endothelinsInvest Ophthalmol Vis Sci343614218258520
- MeyerPFlammerJLüscherTF1995Local action of the renin angiotensin system in the porcine ophthalmic circulation: effects of ACE-inhibitors and angiotensin receptor antagonistsInvest Ophthalmol Vis Sci36555627890486
- MombouliJVVanhouttePM1995Kinins and endothelial control of vascular smooth muscleAnnu Rev Pharmacol Toxicol35679057598512
- MoravskiCJKellyDJCooperME2000Retinal neovascularization is prevented by blockade of the renin-angiotensin systemHypertension36109910411116132
- MorbidekkiLParentiAGiovannelliL1998B1 receptor involvement in the effect of bradykinin on venular endothelial cell proliferation and potentiation of FGF-2 effectsBr J Pharmacol1241286929720802
- MullerDNFiebelerAParkJK2003Angiotensin II and endothelin induce inflammation and thereby promote hypertension-induced end-organ damageClin Nephrol60Suppl 1S21212940529
- MurataMNakagawaMTakahashiS1997Expression and lacalization of angiotensin II type I receptor mRNA in rat ocular tissuesOphthalmologica21138469380359
- NetlandPAChaturvediNDreyerEB1993Calcium channel blockers in the management of low-tension and open-angle glaucomaAm J Ophthalmol115608138488913
- Nouri-MahdaviKBrigattiLWeitzmanM1995Outcomes of trabeculectomy for primary-open angle glaucomaOphthalmology102176099098275
- NyborgNCNielsenPJPrietoD1990Angiotensin-II does not contract bovine retinal resistance arteries in vitroExp Eye Res50469742373150
- OhruiTMatsuiTYamayaM2004Angiotensin-converting enzyme inhibitors and incidence of Alzheimer’s disease in JapanJ Am Geriatr Soc526495015066094
- OkadaYYamanakaISakamotoT2001Increased expression of angiotensin-converting enzyme in retinas of diabetic ratsJpn J Ophthalmol455859111754899
- OtaniATakagiHOhH2000Angiotensin II-stimulated vascular endothelial growth factor expression in bovine retinal pericytesInvest Ophthalmol Vis Sci411192910752960
- QuigleyHANickellsRWKerriganLA1995Retinal ganglion cell death in experimental glaucoma and after axotomy occurs by apoptosisInvest Ophthalmol Vis Sci36774867706025
- RaidooDMRamchurrenNNaidooY1996Visualisation of bradykinin B2 receptors on human brain neuronsImmunopharmacology3310478856125
- RajagopalanSHarrisonDG1996Reversing endothelial dysfunction with ACE inhibitors. A new trendCirculation9424038759059
- RegoliDBarabeJ1980Pharmacology of bradykinin and related kininsPharmacol Rev321467015371
- SarlosSRizkallaBMoravskiCJ2003Retinal angiogenesis is mediated by an interaction between the angiotensin type 2 receptor, VEGF, and angiopoietinAm J Pathol1638798712937129
- SchmechelDEApoptosis in neurodegenerative diseasesHannunYABoustanyRMApoptosis in neurobiologyBoca Raton, FLCRC Press19992348
- SchrierRWEstacioROEalerA2002Effect of aggressive blood pressure control in normotensive type 2 diabetic patients on albuminuria, retinopathy and strokesKidney Int6110869711849464
- SilvestreJSBergayaSTamaratR2001Proangiogenic effect of angiotensin-converting enzyme inhibition is mediated by the bradykinin B2 receptor pathwayCirc Res896788311597990
- SteigerwaltRDJrBelcaroGVLauroraG1998Ocular and orbital blood flow in patients with essential hypertension treated with trandolaprilRetina18539459869463
- StrandgaardSPaulsonOB1992Regulation of cerebral blood flow in health and diseasesJ Cardiovasc Pharmacol19S89931382171
- SuzumaIHataYClermontA2001Cyclic stretch and hypertension induce retinal expression of vascular endothelial growth factor and vascular endothelial growth factor receptor-2: potential mechanisms for exacerbation of diabetic retinopathy by hypertensionDiabetes504445411272159
- TakedaHKimuraYHigashidaH1999Localization of B2 bradykinin receptor mRNA in the rat retina and sclerocorneaImmunophalmacology45515
- The EUCLID Study Group1997Randomized placebo-controlled trial of lisinopril in normotensive patients with insulin-dependent diabetes and normoalbuminuria or microalbuminuriaLancet3491787929269212
- TomitaKAraieMTamakiY1999Effects of nilvadipine, a calcium antagonist, on rabbit ocular circulation and optic nerve head circulation in NTG subjectsInvest Ophthalmol Vis Sci4011445110235547
- TzourioCAndersonCChapmanN2003Effects of blood pressure lowering with perindopril and indapamide therapy on dementia and cognitive decline in patients with cerebrovascular diseaseArch Inter Med163106975
- WagnerJJan DanserAHDerkxFH1996Demonstration of rennin mRNA, angiotensinogen mRNA, and angiotensin converting enzyme mRNA expression in the human eye: evidence for an intraocular rennin-angiotensin systemBr J Ophthalmol80159638814748
- Wheeler-SchillingTHKohlerKSautterM1999Angiotensin II receptor subtype gene expression and cellular localization in the retina and non-neuronal ocular tissues of the ratEur J Neurosci1133879410564346
- YamauchiTKashiiSYasuyoshiH2003Mitochondrial ATP-sensitive potassium channel: a novel site for neuroprotectionInvest Ophthalmol Vis Sci442750612766083
- YaoKTschudiMFlammerJ1991Endothelium-dependent regulation of vascular tone of the porcine ophthalmic arteryInvest Ophthalmol Vis Sci32179182032802
- YasuyoshiHKashiiSZhangS2000Protective effect of bradykinin against glutamate neurotoxicity in cultured rat retinal neuronsInvest Ophthalmol Vis Sci412273810892873
- YolesESchwartzM1998Potential neuroprotective therapy for glaucomatous optic neuropathySurv Ophthalmol42367729493279
- YoshijiHKuriyamaSFukuiH2002Angiotensin-I-converting enzyme inhibitors may be an alternative anti-angiogenic atrategy in the treatment of liver fibrosis and hepatocellular carcinoma. Possible role of vascular endothelial growth factorTumor Biol2334856
- YoshijiHKuriyamaSKawataM2001The angiotensin-I-converting enzyme inhibitor perindopril suppresses tumor growth and angiogenesis: possible role of the vascular endothelial growth factorClin Cancer Res71073811309359
- YusufSSleightPPogueJ2000Effects of an angiotensin-converting-enzyme inhibitor, ramipril, on cardiovascular events in high-risk patients. The Heart Outcomes Prevention Evaluation Study InvestigatorsN Engl J Med3421455310639539
- ZouYAkazawaHQinY2004Mechanical stress activates angiotensin II type 1 receptor wiithout the involvement of angiotensin IINat Cell Biol649950615146194