Abstract
Subluxation of the capsular tension ring (CTR) into the vitreous is a rare complication. The explantation of these rings from the vitreous by conventional vitrectomy is often a difficult procedure requiring great surgical skill. We report two cases of posteriorly subluxated endocapsular rings, which were explanted with pars plana vitrectomy using the chandelier illumination system. This illumination system has an external light source which is incorporated via a fibreoptic into the infusion cannula, thereby freeing both hands of the surgeon. This allows surgeon to easily perform bimanual intraocular maneuvers such as external scleral indentation, manipulation of CTR in the vitreous cavity and removal of these rings with the handshake technique.
The capsular tension ring (CTR) is widely used in cases of zonular dialysis. Posterior dislocation of the CTR into the vitreous is a rare complication (CitationLang et al 2001; CitationBhattacharjee and Bhattacharjee 2004; CitationLevy and Klemperer 2005; CitationAhmed and Chen 2005; CitationMoreno-Montanes 2005). The explantation of these rings from the vitreous by conventional vitrectomy is often a difficult procedure. We report two cases of posteriorly dislocated CTR explanted using a “chandelier” endoillumination system (Photon, Synergetics, USA). This illumination system has xenon light source incorporated into the infusion cannula via a fibreoptic. This “chandelier” illumination system suspended from the inferotemporal sclerotomy site and gives excellent, uniform illumination from ora-to-ora. This frees up the surgeon’s nondominant hand, which would otherwise have been limited to holding the conventional light pipe. This allows the surgeon to utilize both his hands for all surgical maneuvers, which is of unsurpassable advantage, especially when having to manipulate a 11mm PMMA ring inside the vitreous cavity without causing any damage to the delicate intraocular structures including the retina.
The viewing system we used was the wide field vitrectomy lens, which is a contact lens with a 120°–130° field of view, which gives excellent ora-to-ora panoramic visualization. Since this lens inverts the image, we use a stereoscopic diagonal invertor (Carl Zeiss, Germany) which is attached to the operating microscope and which is controlled by the surgeon using a footswitch (CitationNatarajan and Dongargaonkar 2003). Use of illumination system and widefield contact lens (Volk lens) allows the surgeon to easily perform bimanual intraocular maneuvers such as external scleral indentation, manipulation of CTR in the vitreous cavity and removal of these rings with the handshake technique.
Case reports
Case 1
A 60-year old gentleman presented with subluxated, morgagnian cataract, and a best corrected visual acuity (BCVA) of hand movements. He was posted for phacoemulsification with intraocular lens (IOL) implantation. A 13/11 mm CTR (Iocare encocapsular ring, India) was implanted in the bag to stabilize the zonules. During emulsification of the nucleus, the rhexis was accidentally chopped and posterior extension of the rhexis was noted. The remaining nuclear fragments were delivered out with a vectis after extending the corneal section. The posterior extension was noted to be more than half the diameter of the bag and CTR was seen to be posteriorly dislocated. The corneal section was sutured. A 3 port 20 gauge pars plana vitrectomy was done using the “chandelier” illumination system. The CTR was seen at the ora by external scleral indentation. The vitreous adhesions were removed with the vitrectomy probe. The ring was caught using an intraocular diamond tip forceps in one hand while performing external scleral indentation with the other hand. The ring was then maneuvered into the vitreous cavity bimanually and delivered out of the eye through the clear corneal incision using a handshake technique. The sclerotomies were closed and a scleral fixated AcryFold IOL (Gantec corporation, USA) was implanted. The post-operative course of the patient was smooth and at the second postoperative day the vision was 20/40 and at the second month post-operative visit, he had a final BCVA of 20/25. No evidence of phototoxicity was noted.
Case 2
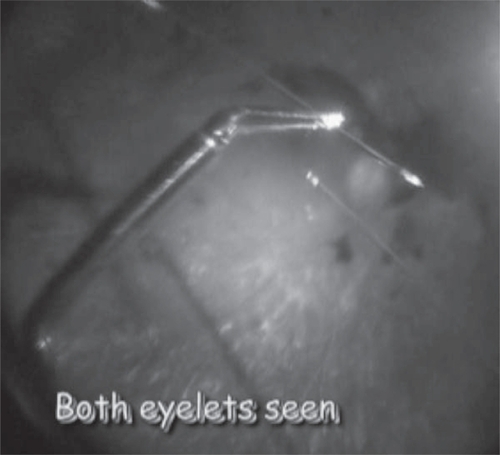
A 52-year old diabetic patient presented to the clinic with a BCVA of 20/200. Examination revealed proliferative diabetic retinopathy and epimacular membrane with subhyloid haemorrhage. He was posted for phacoemulsification and IOL implantation with pars plana vitrectomy for membrane peeling and endolaser. During the surgery a minimal subluxation of the lens was noticed, and CTR (Iocare encocapsular ring, India) was implanted to support the capsular bag. During aspiration of the cortex a posterior capsule rent was noticed. Immediate meticulous examination revealed a near 180° capsular tear and a posterior dislocation of the ring. A 20-gauge pars plana vitrectomy was done using chandelier illumination, the wide field lens and the reinvertor system as described earlier. After performing the vitrectomy, the ring was found by performing external scleral indentation and was grasped from the ora with a diamond tip forceps in one hand while continuing indentation with the other hand. Delicate bimanual handing of the ring was done into the vitreous cavity and then was delivered out via the anterior chamber through the clear corneal incision (). The originally planned vitrectomy was then continued with delamination and peeling of the epiretinal membrane followed by endolaser. A scleral fixated AcryFold IOL (Gantec corporation, USA) was implanted. Postoperatively, the patient was managed conservatively and his BCVA improved to 20/80 at the 2nd post-operative month. No evidence of phototoxicity was noted.
Figure 1 Case 2. Both eyelets of the CTR seen during intravitreal bimanual manipulation under chandelier illumination system.
Discussion
The use of “chandelier” illumination has been described for dissecting epiretinal membranes, retinal detachments, macular translocation surgery, removing large foreign bodies, managing dropped IOLs and nuclear fragments (CitationPacko 2004; CitationKaiser 2005). To the best of our knowledge, this is the first report of such a large (11 mm) diameter object removed from the vitreous cavity using “chandelier” illumination and the contact wide field vitrectomy lens.
In both our cases, the CTR was grasped with the diamond tip forceps while visualizing it with external scleral indentation. As this is a bimanual procedure, it would not have been easily performed were it not for the “chandelier” illumination system. The surgeon was able to handle the CTR delicately and bimanually in the vitreous cavity without assistance and was able to bring the ring into the anterior chamber. The ring was finally removed out of the eye by employing the hand shake technique where the ring is transferred from a forceps in one hand to a forceps held in the other hand. This handshake technique has been used in the past to remove dropped IOLs, nuclear fragments, foreign bodies etc. (CitationLang et al 2001)
The light from the xenon source has been filtered to eliminate a significant proportion of the hazardous part of the light spectrum and thus reduce the phototoxic potential. The greater distance of the light source from the retina as well as the larger surface area over which it is dispersed both contribute to actually make the chandelier light source safer than the conventional light pipe. In a study on rabbit eyes, no phototoxicity from the sustained retinal exposure to a fixed, implantable light source for a clinically relevant duration could be demonstrated whereas a standard endoilluminator probe can create a phototoxic lesion in the experimental setting (CitationVander et al 1991). Other authors (Citationvan den Biesen et al 2000) reported that commercially available light sources for endoillumination during vitrectomy are not safe because of photochemical retinal damage. We did not observe evidence of phototoxicity until 2nd month postoperative period in 2 patients reported herein.
This case report aims at highlighting the ease and comfort, which the chandelier illumination, the contact wide field vitrectomy lens and the stereoscopic diagonal inverter provide to explant posteriorly dislocated CTR.
Disclosure
The authors have no financial or proprietary interest in any product mentioned herein. The authors are supported in part by NIH/NEI grant EY-14793 and an unrestricted grant to MUSC from Research to Prevent Blindness, Inc., New York, NY (RHT).
References
- AhmedIIChenSH2005Surgical repositioning of dislocated capsular tension ringsOphthalmology1217253316199268
- BhattacharjeeHBhattacharjeeK2004Management of a posteriorly dislocated endocapsular tension ring and a foldable acrylic intraocular lensJ Cataract Refract Surg30243614967296
- LangYFinebergEGarzoziHJ2001Vitrectomy to remove posteriorly dislocated endocapsular ringJ Cataract Refract Surg2717101111709226
- LevyJKlempererI2005Posteriorly dislocated capsular tension ringOphthalmic Surg Lasers Imaging364161816238042
- KaiserR2005Vitrectomy; When and how size mattersRev Ophthalmol1212
- Moreno-MontanesJHerasHFernandez-HortelanoA2005Surgical treatment of a dislocated intraocular lens capsular bag-capsular tension ring complexJ Cataract Refract Surg31270315767145
- NatarajanSDongargaonkarS2003Wide angle viewing systems in vitreous surgeryGargAPandeySAdvances in Ophthalmology1st edNew DelhiJaypee Brothers61521
- PackoK2004Early experience reveals benefits of 25 G vitrectomyRev Ophthalmol118
- van den BiesenPRBerenschotTVerdaasdonkRM2000Endoillumination during vitrectomy and phototoxicity thresholdsBr J Ophthalmol841372511090475
- VanderJFEagleRCJrBrownGC1991Retinal tolerance of an implantable light source for use during vitrectomy surgeryOphthalmic Surg2273591787939