Abstract
We describe the smallest incision cataract removal technique, Microphakonit, in which bimanual phacoemulsification can be performed with a 0.7 mm phaco tip and 0.7 mm irrigating chopper. Cortical removal is done using 22 gauge or 0.7 mm irrigation/aspiration instruments. The technique was used for 25 adult human eyes with grade 2 nuclear sclerosis and 5 adult human eyes with grade 3 nuclear sclerosis. None of these patients were noted to have intraoperative complications. One eye with grade 3 nuclear sclerosis had mild, central striate keratopathy postoperatively. Six months after surgery, 92% of the patients had a best corrected visual acuity (BCVA) of 20/20 and 96% had ≥20/25.
Microphakonit is a technique of bimanual phacoemulsification using a 0.7 mm phaco needle tip and 0.7 mm irrigation chopper described by one of us (AA) (CitationAgarwal et al 2007). Herein, we describe the evolution of the instrumentation, surgical technique, and the surgical outcome.
Surgical instrumentation
The Microphakonit technique aims to remove the cataract through 0.7 mm instruments. These tiny optimum incisions avoid fluid leakage around the incision and decrease anterior chamber fluctuations.
Needle tip
An anticipated problem with the 0.7 mm Microphakonit needle compared with the 0.9 mm Phakonit needle was a decrease in the speed of the surgery due to a decrease in the aspiration flow rate. Larry Laks (MicroSurgical Technology, Redmond, WA, USA) tackled this problem by designing a tip with thinner walls, resulting in a relative increase in the inner diameter of the tip. This allowed the speed of surgery to approximate that of a 0.9 mm tip. The efficiency of Microphakonit can be further increased with gas-forced infusion (as described below) and using a 30 degree tip.
Irrigating chopper
A 0.7 mm Microphakonit open-end irrigating chopper was designed specifically for this technique. One of us (AA) has previously designed two 0.9 mm irrigating chopper – open-end and open-side (CitationAgarwal et al 1998a, Citation1998b, Citation2000). Although open-side choppers do not push a piece directly in front of it away as the open-end does, the open-end chopper has the advantage of increased fluid inflow when compared with the open-side irrigating chopper. While designing 0.7 mm irrigating chopper, less fluid inflow is expected. To overcome this problem, it was logical to use open-end model. The open-end 0.7 mm chopper was refined by Larry Laks to reduce any flow restriction present as a by-product of the method of attachment, thus maximizing inflow. This chopper has a sharp cutting edge ().
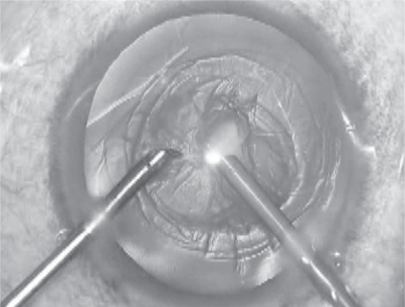
Figure 1 Showing the 0.7 mm phaco tip and the 0.7 mm irrigating chopper. Microphakonit being done.
However, despite using an open-end model, the fluid entering the eye was not enough, and the anterior chamber frequently collapsed. We solved this problem by using gas-forced infusion, either internal or external. Internal gas-forced infusion uses the air pump contained in the same phaco machine. It can regulate the amount of air entering the infusion bottle in such a way that no surge or collapse occurs. The anterior vented, internal gas-forced infusion system of the Accurus system (Alcon laboratories, Texas, USA) helps by creating positive pressure through infusion into the eye when performing the Microphakonit. In this case the air is pushed into the bottle of intraocular solution thus actively pushing the fluid into the eye without raising or lowering the bottle. Control of the air pump is digitally integrated to the Accurus panel. For the Microphakonit, we preset the infusion pump at 100 mmHg. External gas-forced infusion as previously described by this author (CitationAgarwal et al 2002) consists of a fish tank air pump which is connected via a Millipore filter to the infusion bottle. It can be regulated to low or high settings, but not fine tuned. In the 25 eyes of this report, we used the internal gas-forced infusion of the Accurus machine.
Both the Microphakonit needle tip and Microphakonit irrigating chopper can fit onto the handles of the Duet system (MicroSurgical Technology, Redmond, WA, USA). If the surgeon is already using the Duet system and wants to adapt the technology of the Microphaconit, only the tips need to be purchased without changing the handle.
Integration into any existing phaco machine is possible.
Bimanual 0.7 mm irrigation/aspiration handpieces
The bimanual irrigation/aspiration hand-piece with a 0.7 mm diameter is also designed so that it fits the same small incision of Microphakonit. The 0.7 mm irrigation handpiece is constructed to be a side port design.
Surgical technique
Surgical incision
A side-port incision should be made first, and ophthalmic viscosurgical device should be injected from this port. This will distend the globe and help in creating the main incision more easily. Now the main incision can be made. One should be careful to make the incision slightly longer than usual, when using gas-forced infusion and the Microphakonit. We have found the movement of the eye during surgery can be better controlled by making the clear corneal incisions at 1:30 and 4:30 clock hour positions respectively.
Anterior continuous curvilinear capsulorhexis
A 5–6 mm capsulorhexis should be attempted. This can be done with the 26 gauge needle bent to form a cystitome. The bend should be kept small and less angled than usual to avoid it tearing the lip of the incision while entering and exiting the eye. A 25 Gauge rhexis forceps (MST) may also be used by those more accustomed to performing the rhexis using the capsulorhexis forceps. This passes through the 0.7 mm incisions easily. In the nondominant hand, a globe stabilization rod can be used to control the eye movement.
Hydrodissection
Cortical cleaving hydrodissection is performed and the fluid wave passing under the nucleus should be checked as well as a check for rotation of the nucleus. The advantage of Microphakonit is that one can do hydrodissection from both incisions so that even the subincisional areas can get easily hydrodissected. It is of note, however, that because there is little escape of fluid, one should be careful during hydrodissection. If too much fluid is passed into the eye, a complication such as a posterior capsular rent may occur and therefore it is necessary to decompress the anterior chamber during this maneuver by applying slight posterior pressure on the scleral lip while doing hydro maneuvers.
Microphakonit
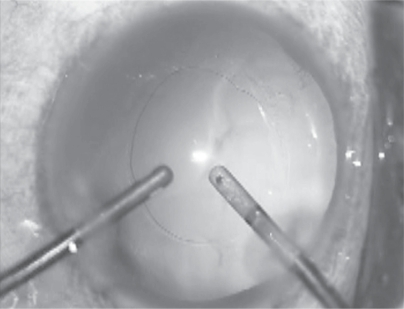
The 22 gauge (0.7 mm) irrigating chopper is connected to the infusion line of the phaco machine and introduced with the foot pedal on position 1. The phaco probe is connected to the aspiration line and the 0.7 mm phaco tip (without an infusion sleeve) is introduced through the clear corneal incision. Using the phaco tip and moderate ultrasound power, the center of the nucleus is directly embedded starting from the superior edge of the rhexis, with the phaco probe directed obliquely downward toward the vitreous (). The settings at this stage are: phaco power, 50%; aspiration flow rate, 20 cc/min; and vacuum, 100–200 mmHg. Using the karate chop technique (CitationJacob et al 2002), the nucleus is chopped and removed (). Cortical wash-up is then accomplished using the bimanual I/A (0.7 mm set) technique (). During this whole procedure, gas-forced infusion is used.
Figure 2 Nucleus removal completed.
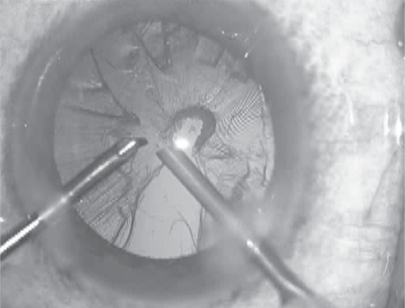
Figure 3 0.7 mm bimanual irrigation aspiration probe used for removal of cortex.
Surgical results
Standard surgical technique was uniformly performed by a single surgeon (AA) for cataract extraction of 20 adult eyes with grade 2 nuclear sclerosis and 5 adult eyes with grade 3 nuclear sclerosis. There were 15 (60%) males and 10 (40%) females. The mean age was 62.3-years ± 6.3, (range, 52 to 76-years). No intraoperative complications were observed. The subjective ease of surgery remained same as when performing bimanual phacoemulsification through the previously available larger bore instruments (eg, 0.9 and 1.1 mm). One eye with grade 3 nuclear sclerosis had mild central striate keratopathy at the first postoperative day which resolved by end of one week. Six months after surgery, 92% of the patients had a best corrected visual acuity (BCVA) of 20/20 and 96% had ≥20/25. One patient developed CME which resolved with treatment to a final BCVA of 20/25. The other patient who had grade 3 nuclear sclerosis pre-operatively had a final BCVA of only 20/200 and was found to have dry ARMD with geographic atrophy secondary to which there was no further improvement in BCVA.
Conclusion
We described application of the smallest incision technique, the Microphakonit using the gas-forced infusion for cataract removal. With the technology and future availability of flexible IOLs that can go easily through an incision less than 1 mm, the small incision technique of the Microphakonit can become an option for the ophthalmic surgeon and a benefit for the patient.
Disclosure
The authors have no financial or proprietary interest in any product mentioned herein. Supported in part by NIH/NEI grant EY-14793 (vision core); and an unrestricted grant to MUSC-SEI from Research to Prevent Blindness, Inc., New York, NY.
References
- AgarwalAJacobSAgarwalAT2007Combating endophthalmitis with microphakonit and no anaesthesia techniqueJ Cataract Refract Surg(In press).
- AgarwalAAgarwalSAgarwalAT1998aNo anesthesia cataract surgeryAgarwalAAgarwalSAgarwalATPhacoemulsification, Laser cataract surgery and foldable IOL’s1st edJaypeeIndia14454
- AgarwalAAgarwalSAgarwalAT1998bPhakonit: A new technique of removing cataracts through a 0.9 mm incisionAgarwalPhacoemulsification, Laser cataract surgery and foldable IOL’s1st edJaypeeIndia13943
- AgarwalAAgarwalSAgarwalAT2000Phakonit and laser phakonit: Lens surgery through a 0.9 mm incisionAgarwalPhacoemulsification, Laser cataract surgery and foldable IOL’s2nd edJaypeeIndia20416
- AgarwalAAgarwalSAgarwalAT2002Antichamber collapserJ Cataract Refract Surg28108512106702
- JacobSAgarwalAAgarwalS2002Trypan blue as an adjunct for safe phacoemulsification in white cataractJ Cataract Refract Surg2818192512388035