Abstract
Objective:
To report on the use of intravitreal bevacizumab (an anti-vascular endothelial growth factor [VEGF] monoclonal antibody) as treatment of diffuse exudative retinal detachment due to ischemic central retinal vein occlusion (CRVO).
Design:
Interventional case report.
Patient:
A 27-year old woman on peritoneal dialysis because of end stage renal failure (ESRF) due to perinuclear antineutrophil cytoplasmic antibody (p-ANCA) associated vasculitis presented with acute unilateral blurred vision. Visual acuity (VA) rapidly deteriorated. Examination revealed the development of total bullous exudative retinal detachment following ischemic CRVO.
Intervention:
Two intravitreal injections of bevacizumab (2.5 mg/0.1ml) were administered followed by panretinal laser photocoagulation.
Main outcome measures:
VA, retinal detachment, and changes in macular edema.
Results:
Prompt significant resolution of exudative retinal detachment with a corresponding gradual improvement of VA from light perception to finger counting. At follow-up examination after 8-months, the retina remained attached.
Conclusion:
Intravitreal bevacizumab proved to be a useful treatment modality in diffuse exudative retinal detachment due to CRVO.
Introduction
Exudative retinal detachment is an uncommon complication of retinal vein occlusion (CitationSchatz et al 1976; CitationBattaglia Parody and Isola 1994). Bullous retinal detachment may respond to panretinal laser photocoagulation (PRP) (CitationSchatz et al 1976; CitationBattaglia Parody and Isola 1994) or to intravitreal triamcinolone acetonide injection (CitationKaracorlu et al 2005). This report describes a young woman with end stage renal failure (ESRF) due to perinuclear antineutrophil cytoplasmic antibody (p-ANCA) associated vasculitis who developed central retinal vein occlusion (CRVO) and very high bullous exudative retinal detachment. She was successfully treated with two intravitreal bevacizumab (AvastinR, Genentech, Inc., San Francisco, CA) injections. To the best of our knowledge, this has not been previously reported.
Case report
A 27-year old woman presented with a 3 day history of blurred vision in her right eye. Six months prior she was admitted with malignant hypertension (blood pressure of 240/140 mmHg and disc edema) and renal failure. Based on a positive p-ANCA with antimyeloperoxidase antibodies (MPO) 84 U/ml (normal < 5 U/ml) and renal biopsy, she was diagnosed as ESRF due to p-ANCA associated vasculitis. Peritoneal dialysis was begun. Treatment with high-dose steroids and azathioprine was initiated. Blood pressure was controlled by multiple antihypertensive drugs. The patient’s disc edema gradually resolved. Over the course of the following six months, basal disease activity subsided. She was well maintained on dialysis with serum hemoglobin of 11.2 g/dl, hematocrit 33.4%, total protein 6.9 g/dl, and albumin 3.8 g/dl.
On presentation, visual acuity (VA) was 6/30 (20/100) in her right eye and 6/8.5 (20/30) in her left eye. Anterior segments in both eyes were normal. Funduscopic findings revealed clinical characteristics of CRVO in the right eye and no abnormality in her left eye. A coagulation screen including activated protein C resistance, protein S, antiphospholipid antibodies, and homocystein was within normal limits. MPO levels were 6.8 U/ml on maintenance oral prednisone (5 mg/d) and azathioprine (50 mg/d). Fluorescein angiography (FA) performed after 3-days showed a nonischemic CRVO with mild macular edema.
Three weeks later the patient noticed further visual deterioration in her right eye. Examination revealed VA 6/120 (20/400), reduced color vision, mild positive relative afferent pupillary defect (RAPD), and an exacerbation of macular edema. Oral prednisone was increased to 20 mg per day. During the ensuing month, VA in the right eye declined to hand motion and RAPD became significantly positive. Severe optic disc and macular edema were seen and FA demonstrated severe ischemic CRVO with diffuse retinal leakage. At fifty days after first complaining of blurred vision, the patient’s VA had dropped to light perception only. A total very high bullous exudative retinal detachment was found without evidence of retinal break. The left eye’s VA, anterior segment, media, and retina were unaffected. Suspecting a relapse of her vasculitis (although MPO levels remained unchanged) a treatment trial of high-dose prednisone (60 mg/d) with an increase of azathioprine (100 mg/d) was attempted. After 2-days, no improvement was seen. As the patient was very reluctant to continue high-dose steroids due to previous severe cushingoid side effects, steroid therapy was rapidly tapered.
After discussing treatment options with the patient and explaining to her the potential risks and benefits of bevacizumab, the patient signed a comprehensive informed consent form. On obtaining approval from the Ethics Committee of Meir Medical Center, she underwent a pars plana injection of 2.5 mg of bevacizumab. The injection was well tolerated without any untoward side effects. Topical antibiotic treatment was given for one week after the injection. Twenty-four hours after bevacizumab administration, a marked reduction in the amount of the subretinal fluid was seen. VA improved to counting fingers after two days. A week following injection only a residual inferior exudative retinal detachment remained and a continuous improvement in macular edema and optic disc swelling was seen. At the two months follow-up examination the macular and disc edema resolved completely and no exudative retinal detachment was noted in any part of the retina (, ). VA, however, did not improve beyond finger counting probably due to the severe perifoveal capillary drop out (). At the 3-months follow up examination a recurrent bullous subtotal exudative retinal detachment was found. An additional 2.5 mg of bevacizumab was injected into the vitreous cavity and one week later the retinal detachment reabsorbed completely. At this point panretinal laser photocoagulation was performed. At the last follow up (8-months), the retina has remained attached.
Figure 1 Two months after intravitreal bevacizumab injection; showing attached retina, retinal hemorrhages, and multiple cotton wool spots.
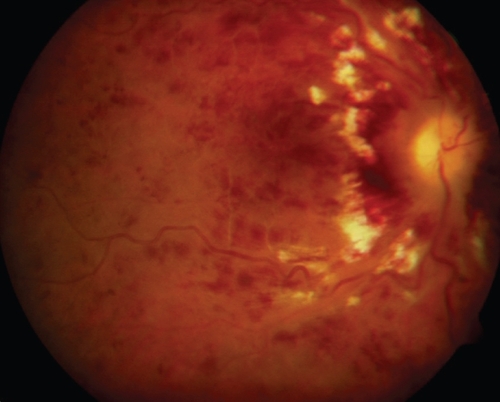
Figure 2 OCT 2 months after intravitreal bevacizumab injection showing no residual subretinal or intraretinal fluid in the macular area.
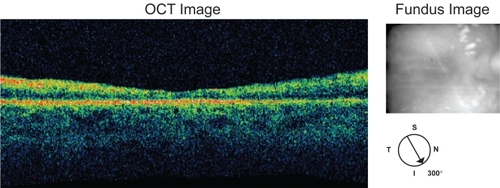
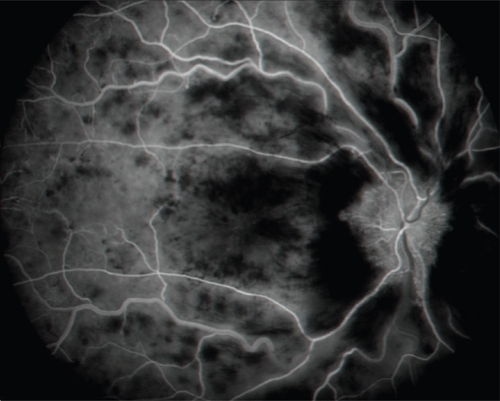
Figure 3 Fluorescein angiography 2 months after intravitreal bevacizumab injection (mid phase) showing drop out of retinal capillaries throughout the entire posterior pole.
Discussion
CRVO is a relatively common disorder affecting mainly adults over 50-years of age (CitationClarkson 1989). The most common risk factors are arterial hypertension and primary open angle glaucoma (CitationClarkson 1989). CRVO associated with systemic vasculitis has been described in the context of syphilis (CitationPrimo 1990) and human immunodeficiency syndrome (HIV) (CitationRoberts and Haefs 1992). Its occurrence, however, in the younger adult is rare. In this report, we present a young woman with ESRF due to p-ANCA vasculitis who developed a nonischemic CRVO which rapidly progressed to a severe ischemic CRVO. p-ANCA vasculitis as an etiology of CRVO is decidedly uncommon. A literature search has yielded only one other such case (CitationIshiguro et al 1999). The progression of nonischemic to ischemic CRVO with the development of an exudative retinal detachment is very infrequently seen in young patients. In our patient, CRVO occurred in the absence of any coagulation abnormality and in the presence of well controlled hypertension. Although no increase in antimyeloperoxidase antibody levels was documented at the time the CRVO appeared, it can be conjectured that the CRVO was probably caused by a localized vasculitis.
The appearance of total exudative retinal detachment in our patient is a unique feature. Previous descriptions of cases having exudative retinal detachment as a complication of retinal venous occlusive disease were all characterized by partial retinal detachment (CitationSchatz et al 1976; CitationBattaglia Parody and Isola 1994; CitationKaracorlu et al 2005). This usually allowed treatment with laser photocoagulation with resultant reabsorption of the subretinal fluid. In our case, the detachment was highly bullous, involving the entire retina, a finding which precluded laser treatment. It began by an ischemic CRVO with diffuse capillary drop out at the entire retina including the macula, progressed to severe disc and macular edema and, within a week, a total bullous retinal detachment.
Rather than triamcinolone, we chose to treat our patient with intravitreal bevacizumab due to the relative failure of high-dose systemic steroids and fear of cataract formation in a young patient.
The pathogenesis of bullous retinal detachment remains speculative. CitationSchatz et al (1976) suggested that in severe capillary nonperfusion the ischemic retina provides a toxic stimulus to the patent retinal vessels causing capillary leakage. The severe venous obstruction and the lack of compensating veno-venous collaterals lead to a large volume of extra cellular fluid which exceeds the retina’s reabsorptive capacity and an exudative retinal detachment develops. Implicated etiological factors have included increased venous hydrostatic pressure and an impairment of the pumping activity of the retinal pigment epithelium (RPE) (CitationBattaglia Parody and Isola 1994).
We suggest that VEGF plays a main role in the development of exudative retinal detachment in CRVO. VEGF acts through a variety of pathways, many of which promote pathological neovascularization. In addition, VEGF is a powerful agonist of vascular permeability. Increased vascular permeability in response to VEGF may be due to formation of fenestrations in microvascular endothelium (CitationRoberts and Palade 1995). In severe retinal ischemia certain growth factors including VEGF are probably discharged into the vitreous. This will lead to extensive exudation from the retinal vessels including the vessels of the optic disc (the disc was very edematous prior to the detachment) exceeding the reabsorptive capability of the RPE pump. Counteracting the effects of VEGF by bevacizumab probably decreases the exudative volume thereby allowing the absorption of the subretinal fluid by the RPE pump. We postulate that the beneficial effect of laser treatment is due to its reduction of VEGF upon ablation of large parts of the ischemic retina. In contrast to what is currently thought, the pumping activity of the RPE is probably intact. We, therefore, imply that even in partial exudative detachment due to CRVO, prompt intravitreal injection of bevacizumab followed by laser PRP may act much better than the current accepted modality of laser photocoagulation alone.
References
- Battaglia ParodyMBIsolaV1994Branch retinal vein occlusion and exudative retinal detachment: pathological aspectsOphthalmologica20829318145981
- ClarksonJG1989Central retinal vein occlusionRyanSJRetina, Vol 2. Medical RetinaSt LouisCV Mosby Co4216
- IshiguroTYamachiIWadaA1999Case of ANCA-related nephritis complicated with central retinal vein occlusionNippon Naika Gakkai Zasshi10888979
- KaracorluMOzdemirHKaracorluS2005Resolution of serous macular detachment after intravitreal triamcinolone acetonide treatment of patients with branch retinal vein occlusionRetina258566016205564
- PrimoS1990Central retinal vein occlusion in a young patient with seropositive syphilisJ Am Optom Assoc618969022081833
- RobertsSPHaefsTM1992Central retinal vein occlusion in a middle – aged man with HIV infectionOphthalmol Vis Sci695679
- RobertsWGPaladeGE1995Increased microvascular permeability and endothelial fenestration induced by vascular endothelial growth factorJ Cell Sci1082369797673356
- SchatzHYannuzziLStraskyTJ1976Retinal detachment secondary to branch vein occlusion: Part IIAnn Ophthalmol81461711035069