Abstract
Implanting glaucoma tubes through the pars plana in the setting of a corneal transplant is becoming more common, and there are unique problems associated with such a procedure. A 42-year-old man with multiple previous eye surgeries presented with a nonfunctioning pars plana glaucoma tube. There was no view to the tube tip, but it was presumed to be clogged with fibrin. Intravitreal tissue plasminogen activator (tPA) was injected through the pars plana which resulted in intraocular pressure control without further surgery. This new application of intravitreal tPA has not been reported previously. Future research should investigate the optimal effective and safe dose of intravitreal tPA injection to relieve such occlusions.
Introduction
Penetrating keratoplasty (PKP) with concurrent anterior chamber placement of a glaucoma tube shunt is associated with a high rate of corneal decompensation.Citation1 Recently, the Cornea Glaucoma Implant Study Group demonstrated that in patients requiring a corneal transplant and a glaucoma tube shunt, the incidence of graft failure and immunologic rejection was decreased with pars plana insertion of the tube.Citation2 We describe a novel application of tissue plasminogen activator (tPA) in the management of an occluded pars plana glaucoma drainage device.
Case report
A 59-year-old African American male had a history of keratoconus with two prior PKPs, cataract extraction with lens implantation, and a failed trabeculectomy in his left eye. He presented with an opaque, vascularized cornea and secondary angle-closure glaucoma. His vision was hand motions and intraocular pressure (IOP) was 40 mmHg by Tonopen (Reichert, Depew, NY). Under general anesthesia, he underwent elective combined Eckardt temporary keratoprosthesis, pars plana vitrectomy, placement of an Ahmed Glaucoma Valve (New World Medical, Rancho Cucamonga, CA) through the pars plana and PKP.
On the first postoperative day, the IOP was 32 mmHg, the area over the Ahmed plate was flat, and the anterior chamber had diffuse fibrin formation. The following day, the IOP climbed to 48 mmHg despite oral acetazolamide as well as dorzolamide hydrochloride 2%, timolol maleate 0.5%, and brimonidine tartrate 0.15% eyedrops. Suspecting a kink in the tube or vitreous incarceration, the patient was returned to the operating room where the tube was flushed easily and was repositioned through a new sclerostomy along the pars plana.
The IOP improved initially, but by one week rose to 40 mmHg despite maximal medical therapy, and there was no elevation over the Ahmed plate (Figure ). The patient’s intense fibrinoid reaction in the anterior chamber, even on 100 mg of oral prednisone daily, precluded an adequate view to the tube and suggested that fibrin was occluding the tube lumen.
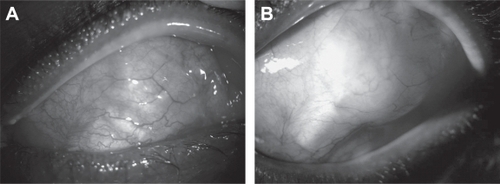
Figure 1 Slit lamp photographs of superotemporal bulbar conjunctiva of the left eye. (A) Before the intravitreal tPA injection, conjunctiva was flat over the Ahmed plate. Note the pericardium (Tutoplast, Costa Mesa, CA) and plate markings. (B) Two months following intravitreal tPA injection, there is a pseudocapsule over the functioning drainage device. Intraocular pressure is controlled with topical medications.
Recombinant tissue plasminogen activator (tPA, Genen-tech Inc, South San Francisco, CA) was injected with a 30-gauge needle 3.5 mm posterior to the limbus. A total of 0.1 cc (12.5 μg) was injected. The next day, the IOP was 9 mmHg, and the bleb over the Ahmed plate was elevated. Five months later, visual acuity improved to 20/50, and IOP was 17 mmHg on brimonidine tartrate 0.15% twice daily and betaxolol 0.25% twice daily. The corneal graft was clear, a pseudocapsule had formed around the Ahmed plate and the tip of the Ahmed tube was well-visualized (Figure ).
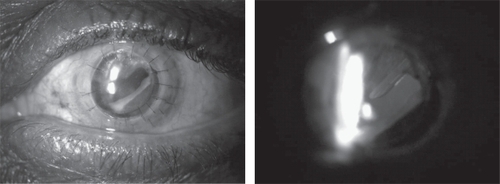
Figure 2 Slit lamp photographs of the left eye taken two months postoperatively. (A) Clear corneal graft with optic capture of a MA60AC (Alcon, Fort Worth, TX) intraocular lens. (B) The tip of the Ahmed tube in the anterior vitreous cavity is not occluded, as visualized by retroillumination.
Discussion
Tissue plasminogen activator (tPA), a stimulator of fibrinolysis, has been used both subconjunctivally and intracamerally following glaucoma surgery since 1992.Citation3 There are no prior reports of intravitreal tPA injection following glaucoma surgery.
Zalta and colleagues reported the largest study using intracameral tPA for occluded or near-occluded limbal glaucoma drainage devices with 89% of subjects (n = 36) achieving success, defined as avoiding the need for additional glaucoma surgery.Citation4 In their study, patients received a mean of 1.6 injections with a mean tPA dose of 15.9 ± 9.9 μg per injection. Six patients had significant complications (severe hyphema, hypotony, anterior chamber flattening), which all occurred after injections that were administered within 5 days after glaucoma surgery.
An important consideration with a pars plana glaucoma tube after corneal surgery, as in our case, is that the tube tip may not be visible in the immediate postoperative period due to corneal edema and/or anterior chamber fibrin. Zalta and colleagues only used tPA on patients who had a visibly occluded or visibly near-occluded tube, defined as fibrin or blood within 2 mm of the tube tip.
Tissue plasminogen activator already has other intraoperative and postoperative uses for the retinal surgeon, such as in displacing submacular hemorrhages, reducing post-vitrectomy fibrin formation, and maintaining patent inferior iridectomies in eyes with silicone oil.Citation5 However, in both animal studies and one human case report, photoreceptor toxicity was noted following 50 μg of intravitreal tPA.Citation6,Citation7
Our case demonstrates successful application of intravitreal tPA in a nonfunctioning pars plana Ahmed tube. Our patient achieved IOP control without further intraocular surgery. This innovation is particularly relevant because of the increasing frequency of implanting Ahmed tubes through the pars plana.
We conclude that intravitreal tPA is a useful option for patients with nonfunctioning pars plana glaucoma tubes due to fibrin. The procedure can avoid a reoperation on an already inflamed and vulnerable postsurgical eye. Future investigation should be directed towards the optimal effective and safe dose of intravitreal tPA, taking into consideration that the medicine will quickly leave the eye once patency of the glaucoma tube is reestablished.
Acknowledgements
Martha Moszczynski, BA and Rachel Revilla-Groh, BS; digital imaging specialists of the Department of Ophthalmology, Columbia University. The authors report no conflicts of interest in this work.
References
- Al-TorbakAGraft survival and glaucoma outcome after simultaneous penetrating keratoplasty and Ahmed Glaucoma Valve implantCornea200322194712658081
- RitterbandDCShapiroDTrubnikVPenetrating keratoplasty with pars plana glaucoma drainage devicesCornea2007261060617893534
- SzymanskiAPromotion of glaucoma filter bleb with tissue plasminogen activator after sclerectomy under a clotInt Ophthalmol199216387901428577
- ZaltaAHSweeneyCPZaltaAKIntracameral tissue plasminogen activator use in a large series of eyes with valved glaucoma drainage implantsArch Ophthalmol200212014879312427061
- KameiMEstafanousMLewisHTissue plasminogen activator in the treatment of vitreoretinal diseasesSemin Ophthalmol200015445010749314
- ChenSNYangTCHoCLRetinal toxicity of intravitreal tissue plasminogen activator: case report and literature reviewOphthalmology2003110704812689889
- HrachCJJohnsonMWHassanASRetinal toxicity of commercial intravitreal tissue plasminogen activator solution in cat eyesArch Ophthalmol20001186596310815158