Abstract
Pars plana vitrectomy (PPV) is growing in popularity for the treatment of primary rhegmatogenous retinal detachment (RD). PPV achieves favorable anatomic and visual outcomes in a wide variety of patients, especially in pseudophakic RD. A growing number of clinical series, both retrospective and prospective, have demonstrated generally comparable outcomes comparing PPV and scleral buckling (SB) under a variety of circumstances. The Scleral Buckling Versus Primary Vitrectomy in Rhegmatogenous Retinal Detachment (SPR) study is a multicenter, randomized, prospective, controlled clinical trial comparing SB versus PPV. This study should provide useful guidelines in the future. At this time, the choice of SB versus PPV should be based on the characteristics of the RD, the patient as a whole, and the experience and preference of the individual retinal surgeon.
Introduction
Primary rhegmatogenous retinal detachment (RD) remains an important cause of visual loss (). The fundamental principles of retinal attachment surgery are well defined. Specifically, all retinal breaks are identified and treated, and vitreous traction is relieved as part of the surgical strategy. The two most common re-attachment procedures performed today are scleral buckling (SB) and pars plana vitrectomy (PPV) (CitationSchwartz and Flynn 2006). Pneumatic retinopexy (PR) is appropriate for selected superior detachments (CitationTornambe 1997). Laser demarcation (CitationVrabec and Baumal 2000) and observation (CitationBrod et al 1995) may be considered in rare circumstances. PPV () is growing in popularity for the treatment of primary RD (CitationSPR Study Group 2003). The current manuscript will review the published literature on the topic and offer guidelines based on the evidence available today.
Figure 1 Primary rhegmatogenous retinal detachment, left eye, with a flap retinal tear at 1:00.
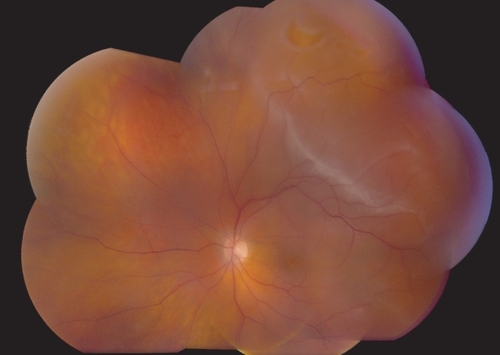
Figure 2 Pars plana vitrectomy (PPV) for rhegmatogenous retinal detachment, utilizing wide-field imaging and small-gauge transconjunctival sutureless instrumentation.

Theoretical considerations
Successful retinal attachment surgery requires effective treatment of retinal breaks and relief of vitreoretinal traction (CitationSchwartz and Mieler 2004). Traditionally, SB was considered the procedure of choice for primary RD. SB is the most well-established technique, and has the longest published follow-up data (CitationSchwartz et al 2002). SB has a high single-operation success rate (SOSR) and is considered for many primary retinal detachments, except cases with very posterior breaks and cases in which placing the buckling elements is too technically difficult, such as eyes with thin sclera, prior strabismus surgery, glaucoma drainage devices, etc. Additional relative contraindications to SB alone (without PPV) include giant retinal tear, proliferative vitreoretinopathy (PVR) grade C, and significant vitreous opacity or hemorrhage.
However, PPV is growing in popularity as a first-line procedure for primary RD, especially in pseudophakic patients (CitationLois and Wong 2003, CitationSPR Study Group 2003). PPV has several advantages over SB (). Perhaps the major benefit of PPV is the potential for an improved view of the retinal periphery, allowing increased identification of retinal breaks. Some authors have advocated the use of transretinal injection of trypan blue (CitationJackson et al 2007) to facilitate intraoperative localization of retinal breaks. PPV removes vitreous opacities, and allows concomitant cataract surgery or posterior capsulotomy, if necessary to further improve visualization. PPV allows for more controlled drainage of subretinal fluid, either with perfluorocarbon liquids or internal drainage techniques (CitationBrazitikos et al 2003). This may achieve complete intraoperative retinal attachment (particularly important for giant retinal tears) without the risk of hemorrhage or retinal incarceration inherent in external drainage procedures. PPV is unlikely to cause significant motility disturbances, and is frequently less painful than SB. PPV is less likely to cause significant refractive changes than SB in pseudophakic eyes, although some phakic eyes will develop nuclear sclerosis and induced myopia following PPV.
Table 1 Pars plana vitrectomy (PPV) versus scleral buckling (SB)
Disadvantages and complications may also occur with PPV for primary retinal detachment (). PPV increases the risk of new retinal breaks (CitationAl-Harthi et al 2005), cataract formation (CitationLing et al 2005), and intraocular pressure elevation (CitationLee et al 2004). If perfluorocarbon liquids are used, they may be retained in the vitreous cavity or subretinal space (CitationRoth et al 2004). Rare complications may include retinal incarceration into a sclerotomy (CitationStopa and Toth 2006), displacement of a laser in situ keratomileusis (LASIK) flap (CitationTosi et al 2005), and direct retinal trauma during air-fluid exchange (CitationYang et al 2006).
PPV is somewhat more technically difficult in phakic patients, because access to the vitreous base is impeded by the crystalline lens. Wide-angle viewing systems and external scleral indentation from a surgical assistant may be helpful (CitationWeichel et al 2006). Perfluorocarbon liquids may be used to stabilize the posterior retina during these maneuvers (CitationBrazitikos et al 2003). Removing peripheral vitreous with 25 gauge vitrectomy instrumentation can be difficult and sometimes impossible. Therefore, many surgeons prefer either 23 gauge or 20 gauge vitrectomy instrumentation for this purpose. In addition, concomitant SB or pars plana lensectomy may be considered.
Traditional teaching held that PPV for primary retinal detachment had too many disadvantages, but recent published case series have called this concept into question. These are summarized in . PPV without SB was traditionally believed to have a low SOSR in patients with inferior breaks. However, recent series have demonstrated favorable results with PPV for these patients (CitationSharma et al 2004; CitationMartinez-Castillo, Boixadera, et al 2005CitationMartinez-Castillo, Verdugo, et al 2005). PPV was traditionally believed to require long-acting intraocular gas (or silicone oil) tamponade, especially for inferior breaks. However, recent case series have documented generally favorable results using air tamponade or even aqueous tamponade (CitationMartinez-Castillo, Boixadera et al 2005; CitationMartinez-Castillo, Verdugo et al 2005; CitationMartinez-Castillo et al 2007). PPV was traditionally believed to require some degree of face-down positioning for inferior breaks, but a recent case series demonstrated favorable outcomes with very limited positioning requirements (CitationMartinez-Castillo et al 2007).
Table 2 Pars plana vitrectomy: traditional teaching versus current literature
An alternative approach to inferior, more complex RDs (large and more posterior tears, advanced proliferative vitreoretinopathy, etc.) is the use of intermediate-term, heavier-than-water tamponade agents. Some authors have advocated the use of retained intravitreal perfluorocarbon liquids, either alone or in combination with silicone oil, for post-operative internal tamponade (CitationRofail and Lee 2005; CitationAsensio-Sanchez et al 2007). The combination of perflurohexyloctane (F6H8) and silicone oil has been advocated by some authors (CitationRizzo et al 2006). Heavy silicone oil (Oxane HD, Bausch and Lomb, Toulouse, France) also has demonstrated some efficacy (CitationWolf et al 2003). Neither perfluorohexyloctane nor heavy silicone oil is available for routine clinical use in the United States at this time.
Clinical studies
The first report of PPV without concomitant SB to treat RD was published in 1985 (CitationEscoffery et al 1985). Since that time, numerous case series have been published (). In general, the outcomes (SOSR and visual acuity) appear comparable to those achieved with SB for a wide variety of patients. The poorest outcomes were reported in series which contained patients with chronic detachments and evidence of PVR.
Table 3 Selected case series of pars plana vitrectomy for rhegmatogenous retinal detachment
Several retrospective series comparing SB, PPV, and/or combined SB/PPV have appeared in the past few years. These series describe a wide variety of clinical situations and are summarized in . The majority of these series found no statistically significant difference in SOSR among the various procedures. Similarly, visual results were generally comparable.
Table 4 Selected retrospective comparative trials
Similarly, an increasing number of prospective clinical trials are being reported, many of which are randomized. These are summarized in . Again, the majority of these studies found no statistically significant differences in either SOSR or visual results between the two treatment modalities.
Table 5 Selected prospective comparative trials
Other literature reviews have reported conflicting results. One meta-analysis of 29 published studies of pseudophakic RD reported that both PPV and combined PPV/SB were associated with higher SOSRs and better visual acuity outcomes than was SB alone (CitationArya et al 2006). However, another review of 9 published studies comparing PPV to SB found no statistically significant differences with respect to SOSR or visual results (CitationSaw et al 2006).
Another area of controversy regards risk of postoperative re-detachment and PVR. A recent statistical analysis reported that SB increased the risk of PVR, especially in pseudophakic cases (CitationRodriguez de la Rua et al 2005), which contrasted an earlier report indicating the reverse (CitationCowley et al 1989).
At this time, there has been no definitive prospective, randomized, controlled clinical trial comparing SB to PPV, and this question remains unresolved (CitationMcLeod 2004). The Scleral Buckling versus Primary Vitrectomy in Rhegmatogenous Retinal Detachment (SPR) study is a European multicenter, randomized, prospective, controlled clinical trial comparing PPV to SB (CitationHeimann 2001). The SPR study may be limited by the fact that a significant proportion of patients in the primary PPV group also received SB. As yet, no results have been published.
Conclusions
Although PPV was traditionally considered a second-line procedure for rhegmatogenous RD, there is a growing body of evidence that, in certain cases, PPV represents a reasonable primary approach. However, most of the current literature comes from small case series with limited follow-up and other methodological flaws. The upcoming SPR study should provide useful guidelines.
Therefore, in the absence of convincing study data, the choice of procedure for any individual patient should be left to the surgeon’s best clinical judgment, taking into account various factors such as the number, size, and position of retinal breaks; the lens status; the patient’s expected ability to cooperate with postoperative positioning requirements; available operating room equipment and staff; surgeon preference; and patient preference. By avoiding a regimented approach and adopting an individualized strategy, results of RD surgery may be optimized. Although some patients will not achieve re-attachment after the initial surgery, a variety of surgical techniques are successful in the vast majority of patients.
Support
Supported in part by NIH center grant P30-EY014801 and by Research to Prevent Blindness, New York, NY, USA.
References
- AfrashiFErakgunTAkkinC2004Conventional buckling surgery or primary vitrectomy with silicone oil tamponade in rhegmatogenous retinal detachment with multiple breaksGraefes Arch Clin Exp Ophthalmol24229530014714188
- AhmadiehHMoradianSFaghihiH2005Anatomic and visual outcomes of scleral buckling versus primary vitrectomy in pseudophakic and aphakic retinal detachment. Six-month follow-up results of a single operation. Report no. 1Ophthalmology1121421915961159
- Al-HarthiEAbboudEBAl-DhibiH2005Incidence of sclerotomy-related retinal breaksRetina25281415805903
- AryaAVEmersonJWEngelbertM2006Surgical management of pseudophakic retinal detachments: a meta-analysisOphthalmology11317243317011954
- Asensio-SanchezVMTorreblanca AgueraBMartinez-CalvoS2007Deposits of perfluorooctane after prolonged use as a post-operative vitreous substituteArch Soc Esp Oftalmol82241317443431
- BrazitikosPDAndroudiSD’AmicoDJ2003Perfluorocarbon liquid utilization in primary vitrectomy repair of retinal detachment with multiple breaksRetina236152114574244
- BrazitikosPDAndroudiSChristenWG2005Primary pars plana vitrectomy versus scleral buckle surgery for the treatment of pseudophakic retinal detachment: A randomized clinical trialRetina259576416340523
- BrodRDFlynnHWJrLightmanDA1995Asymptomatic rhegmatogenous retinal detachmentsArch Ophthalmol113103027639653
- CampoRVSipperlyJOSneedSR1999Pars plana vitrectomy without scleral buckle for pseudophakic retinal detachmentsOphthalmology10618111510485555
- ChengSFYangCHLeeCH2006Anatomical and functional outcome of surgery for primary rhegmatogenous retinal detachment in high myopic eyesEyeJul 21 [Epub ahead of print]
- CowleyMConwayBPCampochiaroPA1989Clinical risk factors for proliferative vitreoretinopathyArch Ophthalmol1071147512757544
- EscofferyRFOlkRJGrandMG1985Vitrectomy without scleral buckling for primary rhegmatogenous retinal detachmentAm J Ophthalmol99275813976804
- HeimannHHellmichMBornfeldN2001Design issues and implications. SPR study report no. 1Graefes Arch Clin Exp Ophthalmol2395677411585312
- HeimannHZouXJandeckC2006Primary vitrectomy for rhegmatogenous retinal detachment. An analysis of 512 casesGraefes Arch Clin Exp Ophthalmol26110
- JacksonTLKwanASLaidlawAH2007Identification of retinal breaks using subretinal trypan blue injectionOphthalmology1145879017123612
- JohannsonKMalmsjoMGhoshF2006Tailored vitrectomy and laser photocoagulation without scleral buckling for all primary rhegmatogenous retinal detachmentsBr J Ophthalmol9012869116837538
- LingCAWeiterJJBuzneySM2005Competing theories of cataractogenesis after pars plana vitrectomy and the nutrient theory of cataractogenesis. A function of altered aqueous fluid dynamicsInt Ophthalmol Clin451739816199976
- LeeEJ2004Use of nitrous oxide causing severe visual loss 37 days after retinal surgeryBr J Anaesth93464615220168
- LoisNWongD2003Pseudophakic retinal detachmentSurv Ophthalmol484678714499816
- Martinez-CastilloVBoixaderaAVerdugoA2005Pars plana vitrectomy alone for the management of inferior breaks in pseudophakic retinal detachment without facedown positionOphthalmology1121222615939475
- Martinez-CastilloVVerdugoABoixaderaA2005Management of inferior breaks in pseudophakic rhegmatogenous retinal detachment with pars plana vitrectomy and airArch Ophthalmol12310788116087841
- Martinez-CastilloVZapataMABoixaderaA2007Pars plana vitrectomy, laser retinopexy, and aqueous tamponade for pseudophakic rhegmatogenous retinal detachmentOphthalmology11429730217056117
- McLeodD2004Is it time to call time on the scleral buckle?Br J Ophthalmol881357915489471
- MikiDHidaTHottaK2001Comparison of scleral buckling and vitrectomy for retinal detachment resulting from flap tears in superior quadrantsJpn J Ophthalmol451879111313053
- OshimaYYamanishiSSawaM2000Two-year follow-up study comparing primary vitrectomy with scleral buckling for macula-off rhegmatogenous retinal detachmentJpn J Ophthalmol445384911033134
- RizzoSGenovesi-EbertFBeltingC2006The combined use of perfluorohexyloctane (F6H8) and silicone oil as an intraocular tamponade in the treatment of severe retinal detachmentGraefes Arch Clin Exp Ophthalmol2447091616550400
- Rodriguez de la RuaEPastorJCAragonJ2005Interaction between surgical procedure for repairing retinal detachment and clinical risk factors for proliferative vitreoretinopathyCurr Eye Res301475315814473
- RofailMLeeLR2005Perfluoro-n-octane as a postoperative vitreo-retinal tamponade in the management of giant retinal tearsRetina2589790116205570
- RoiderJHoeraufHHagerA2001[Conventional ablation surgery or primary vitrectomy in complicated retinal holes]Ophthalmologe988879111594233
- RothDBSearsJELewisH2004Removal of retained subfoveal perfluoro-n-octane liquidAm J Opthalmol1382879
- SaliconeASmiddyWEVenkatramanAFeuerW2006Management of retinal detachment when no break is foundOphthalmology11339840316406538
- SawSMGazzardGWagleAMLimJAu EongKG2006An evidence-based analysis of surgical interventions for uncomplicated rhegmatogenous retinal detachmentActa Ophthalmol Scand846061216965489
- SchmidtJCRodriguesEBHoerleS2003Primary vitrectomy in complicated rhegmatogenous retinal detachment. A survey of 205 eyesOphthalmologica2173879214573970
- SchwartzSGFlynnHW2006Primary retinal detachment: scleral buckle or pars plana vitrectomy?Curr Opinion Ophthalmol1724550
- SchwartzSGKuhlDPMcPhersonAR2002Twenty-year follow-up for scleral bucklingArch Ophthalmol120325911879136
- SchwartzSGMielerWF2004Management of primary rhegmatogenous retinal detachmentComp Ophthalmol Update528594
- SharmaAGrigoropoulosVWilliamsonTH2004Management of primary rhegmatogenous retinal detachment with inferior breaksBr J Ophthalmol881372515489475
- SharmaYRKarunanithiSAzadRV2005Functional and anatomic outcome of scleral buckling versus primary vitrectomy in pseudophakic retinal detachmentActa Ophthalmol Scand83293715948779
- SpeicherMAFuADMartinJP2000Primary vitrectomy alone for repair of retinal detachments following cataract surgeryRetina204596411039419
- SPR Study Group2003View 2. The case for primary vitrectomyBr J Ophthalmol87784712770983
- StangosANPetropoulosIKBrozouCG2004Parsplana vitrectomy alone vs vitrectomy with scleral buckling for primary rhegmatogenous pseudophakic retinal detachmentAm J Ophthalmol138952815629285
- StopaMTothCA2006A method to free retina and vitreous from intra-operative incarceration in the sclerotomyRetina261070117151496
- TewariHKKedarSKumarA2003Comparison of scleral buckling with combined scleral buckling and pars plana vitrectomy in the management of rhegmatogenous retinal detachment with unseen retinal breaksClin Exp Ophthalmol314037
- TornambePE1997Pneumatic retinopexy: the evolution of case selection and surgical technique. A twelve-year study of 302 eyesTrans Am Ophthalmol Soc95551789440187
- TosiGMTilanusMAEgginkC2005Flap displacement during vitrectomy 24 months after laser in situ keratomileusisRetina251101316340545
- VrabecTRBaumalCR2000Demarcation laser photocoagulation of selected macula-sparing rhegmatogenous retinal detachmentsOphthalmology1071063710857823
- WeichelEDMartidisAFinemanMS2006Pars plana vitrectomy versus combined pars plana vitrectomyscleral buckle for primary repair of pseudophakic retinal detachmentOphthalmology11320334017074564
- WickhamLConnorMAylwardGW2004Vitrectomy and gas for inferior break retinal detachments. Are the results comparable to vitrectomy, gas, and scleral buckle?Br J Ophthalmol881376915489476
- WolfSSchonVMeierPWiedemannP2003Silicone oil-RMN3 mixture (“heavy silicone oil”) as internal tamponade for complicated retinal detachmentRetina233354212824833
- YangSSMcDonaldHREverettAI2006Retinal damage caused by air-fluid exchange during pars plana vitrectomyRetina26334816508435