Abstract
Uveitis is an inflammatory, putative Th1-mediated autoimmune disease that affects various parts of the eye and is a leading cause of visual loss. Currently available therapies are burdened with toxicities and/or lack definitive evidence of efficacy. Voclosporin, a rationally designed novel calcineurin inhibitor, exhibits a favorable safety profile, a strong correlation between pharmacokinetic and pharmacodynamic response, and a wide therapeutic window. The LUMINATE (Lux Uveitis Multicenter Investigation of a New Approach to TrEatment) clinical development program was initiated in 2007 to assess the safety and efficacy of voclosporin for the treatment, maintenance, and control of all forms of noninfectious uveitis. If LUMINATE is successful, voclosporin will become the first Food and Drug Administration-approved corticosteroid-sparing agent for this condition.
Introduction
Uveitis, an inflammatory, Th1-mediated autoimmune disease affecting various parts of the eye, is a significant cause of visual loss. The condition accounts for 2.8% to 10% of all cases of blindness, including approximately 30,000 new cases of legal blindness in the United States each year (CitationNussenblatt 1990; CitationGritz and Wong 2004). A recent report estimates the incidence of uveitis at more than 50 cases per 100,000 person-years, with a prevalence of 115 per 100,000 persons (CitationGritz and Wong 2004).
Corticosteroids (topical, systemic, locally injected, or corticosteroid-eluting implants) are the current mainstay of therapy and the only Food and Drug Administration (FDA)-approved treatment for uveitis. Although often highly effective, chronic corticosteroid use, whether administered systemically or locally, is burdened with well-known, serious adverse events (AEs) including osteoporosis, metabolic disturbances, diabetogenicity and obesity, elevated blood pressure, and impaired wound healing. A number of currently available immunosuppressive agents (eg, antimetabolites, T-cell inhibitors, alkylating agents) are commonly employed as steroid-sparing therapies; however, randomized controlled clinical trials on the use of these agents in uveitis patients are broadly lacking (CitationJabs and Karamursel 2005). Moreover, many of these agents are associated with significant, serious AEs. Therefore, immunosuppressive agents with proven efficacy and an acceptable safety profile are a much needed addition to the therapeutic armamentarium for the management of this serious disease.
Voclosporin
Description/mechanism of action
Voclosporin (Lux Biosciences, Inc. Jersey City, NJ) is a rationally designed novel calcineurin inhibitor (CitationIsotechnika, Inc., 2008) currently in phase 2/3 clinical development for noninfectious uveitis. The inventor of the compound, Isotechnika, Inc., (Edmonton, Canada), is concurrently developing the drug for plaque psoriasis and the prevention of allograft rejection (CitationNo authors listed 2007).
Voclosporin is a next-generation calcineurin inhibitor. Calcineurin inhibitors are potent immunosuppressants that reversibly inhibit T-cell proliferation and prevent release of proinflammatory cytokines by blocking the activity of the calcium-regulated serine-threonine phosphatase calcineurin, an enzyme found in cell cytoplasm (CitationSchreiber and Crabtree 1992; CitationDumont 1996). Calcineurin inhibitors also block lymphokine production and release, fibroblast proliferation, and vascular endothelial growth factor expression (CitationDumont 1996; CitationHo et al 1996; CitationCho et al 2002). After entering the lymphocyte, calcineurin inhibitors bind intracellularly to immunophilins and form complexes that subsequently bind to and inhibit calcineurin (CitationSchreiber and Crabtree 1992; CitationStalder et al 2003). This process prevents translocation to the nucleus of the cytoplasmic component of the nuclear factor of activated T cells (NFAT), which in turn impairs transcription of the genes encoding interleukin-2 (IL-2) and other lymphokines (CitationSchreiber and Crabtree 1992; CitationHo et al 1996).
Voclosporin was developed by modification of the functional group on the amino acid residue at position 1 of the cyclosporin A (CsA) molecule () (CitationDumont 2004). The result is a more predictable pharmacokinetic profile than that of CsA (CitationYatscoff et al 2002; CitationAbel et al 2003; CitationWasel et al 2006) and an approximately 4-fold greater inhibitory potency as measured by the in vitro calcineurin inhibition assay. (CitationAbel et al 2004; CitationAspeslet et al 2004). Results of phase 1, phase 2, and phase 3 clinical trials indicate that voclosporin exhibits a well correlated pharmacokinetic/pharmacodynamic (PK/PD) relationship (–) (CitationYatscoff et al 2002; CitationAbel et al 2003; CitationWasel et al 2006). The utility of systemically administered voclosporin for the prevention and treatment of experimental autoimmune uveoretinitis (EAU) in rats has been reported recently (CitationCunningham et al 2007).
Figure 1 Comparison of structures of voclosporin (left) and cyclosporin A (right).
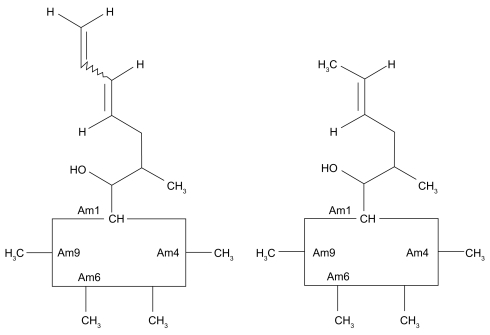
Figure 2 Comparison of calcineurin inhibition of voclosporin versus CsA.
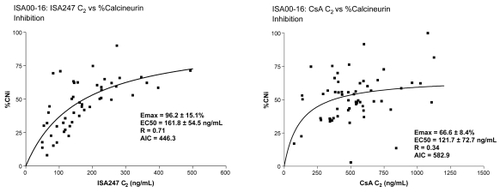
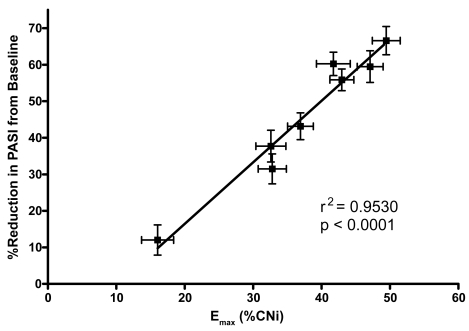
Figure 3 Emax versus reduction in PASI in phase 3 psoriasis study.
Clinical trials with voclosporin
The PK/PD profile of voclosporin has been evaluated in six phase 1 studies in healthy volunteers. Doses in single-dose studies ranged from 0.25 mg/kg to 4.5 mg/kg, and in multiple-dose studies, from 0.25 mg/kg bid to 1.5 mg/kg bid. Voclosporin exhibited good bioavailability, rapid absorption (median time to maximum [Tmax] < 2 hours), and first-order pharmacokinetics indicated by linear increases in area under the curve (AUC) and maximum concentration (Cmax) as a function of dose. Whole blood concentration profiles indicated multiphasic elimination after 24 hours. In a multiple-dose study of 0.25 mg/kg and 0.5 mg/kg bid for 10 days, the T1/2 was 6.9 to 7.8 hours on Day 1 and 30.1 to 33.2 hours on Day 13, indicating an approximate 4-fold accumulation of voclosporin whole blood levels on Day 13 (CitationIsotechnika, Inc., 2008).
Voclosporin undergoes extensive first-pass hepatic metabolism via hydroxylation and N-demethylation reactions to active metabolites. Cytochrome P450 3A4/5 acts as the primary enzyme involved in phase I of the metabolism of voclosporin (CitationFreitag et al 2006; CitationIsotechnika, Inc., 2008). Voclosporin inhibits the activity of P450 3A4, but not CYP2D6 or CYP2C9. Based on animal studies, fecal excretion is the primary route of elimination. voclosporin should be taken on an empty stomach to ensure adequate drug concentration, based on results of a pharmacokinetic study that indicate a food effect on the rate and extent of drug absorption (CitationIsotechnika, Inc., 2008).
Results of phase 1 trials indicate that the pharmacodynamic ability of voclosporin to inhibit calcineurin appears to be dose-proportional up to a maximum of 1 mg/kg bid for 10 days, after which the degree of inhibition plateaus (CitationIsotechnika, Inc., 2008). The efficacy of voclosporin in organ transplantation and psoriasis has been reported and is indicative of the potential scope of the compound in the treatment of immune disorders, including noninfectious uveitis.
In a phase 2a, 12-week, randomized, multicenter, open-label study, the primary endpoints of a low incidence of acute rejection and stable kidney function were maintained in 132 stable, post–renal transplant patients who were switched from CsA (Neoral®) to voclosporin (CitationYatscoff et al 2003; CitationDumont 2004). Further, voclosporin produced a level of immunosuppression comparable to CsA at 33% of the blood drug concentration. Strong correlations were seen between C0 (concentration of drug in plasma at the time of an instantaneous intravenous injection of a drug that is instantaneously distributed to its volume of distribution) and both AUC and calcineurin inhibition for voclosporin, but not for CsA ().
A 24-week, randomized, open-label, phase 2b trial in de novo renal transplant patients to compare the efficacy and safety of voclosporin and tacrolimus has recently completed enrollment. Starting doses were 0.4, 0.6, and 0.8 mg/kg bid for voclosporin and 0.05 mg/kg bid for tacrolimus, with doses titrated to target trough concentrations (CitationGaston et al 2006). In a recent safety update of the first 116 patients who completed ~4 months of therapy (range, 3.7 ± 2.2 to 4.5 ± 2.2 months), similar efficacy, as measured by biopsy-proven acute rejection episodes, was demonstrated between the two agents, as well as an acceptable safety profile. Excellent renal function was noted in all voclosporin dose groups (CitationBusque et al 2007).
In a 24-week randomized trial in 451 patients with moderate to severe plaque psoriasis, a statistically significant difference for voclosporin vs placebo was seen at weeks 12 and 24 in the Psoriasis Area and Severity Index (PASI 75) response, as well as a 2-point reduction in the Static Global Assessment score (CitationGupta et al 2006; CitationLangley et al 2006). Patients received placebo or voclosporin (0.2 mg/kg, 0.3 mg/kg, or 0.4 mg/kg bid) for 12 weeks, after which the placebo group was switched to voclosporin 0.3 mg/kg bid. Drug concentration was highly correlated with calcineurin inhibition (r = 0.79), and percent calcineurin inhibition was highly correlated with mean percent reduction in the efficacy endpoint (PASI; r = 0.86), illustrating the strong PK/PD correlation of voclosporin () (CitationGupta et al 2006).
Clinical safety of voclosporin
Voclosporin was well tolerated and safe in all single- and multiple-dose phase 1 trials in dosages up to 4.5 mg/kg, and in phase 2 and phase 3 trials in renal transplantation and psoriasis patients (CitationAspeslet et al 2001, Citation2004; CitationDumont 2004; CitationGaston et al 2006; CitationGuenther et al 2006; CitationIsotechnika, Inc., 2007a; CitationNo authors listed 2007). In phase 2 and 3 trials, the most common AEs, typically of low frequency and mild severity, were diarrhea, headache, and hypertension (CitationYatscoff et al 2003; CitationGaston et al 2006; CitationGuenther et al 2006). These events appeared to be dose-dependent. No significant changes in levels of cholesterol, triglycerides, or other biochemical parameters, or in new-onset diabetes or infectious complications, have been reported in studies to date.
Renal function, assessed by creatinine clearance, remained stable in patients in clinical trials, with few experiencing clinically significant changes. Specifically, in the phase 3 study in psoriasis, the highest mean change in serum creatinine in any dosing group (0.2, 0.3, or 0.4 mg/kg bid) at week 12 was 5.6% above baseline, which is considered to be within normal analytic and physiologic variation (CitationLangley et al 2006; CitationIsotechnika, Inc., 2007b; CitationNo authors listed 2007). A total of 5 patients (4 [4%] in the high-dose and 1 [1%] in the mid-dose group) withdrew due to a clinically significant decrease in kidney function (CitationNo authors listed 2007) At 24 weeks, there were no clinically significant changes in mean serum creatinine or glomerular filtration rate (GFR), but 5 (2%) patients withdrew due to changes in renal function (30% decrease in GFR confirmed) (CitationPapp et al 2004). After 60 weeks, mean serum creatinine remained stable, with clinically significant changes in kidney function occurring in 4% of patients (CitationIsotechnika, Inc., 2007b).
Therapeutic window of voclosporin
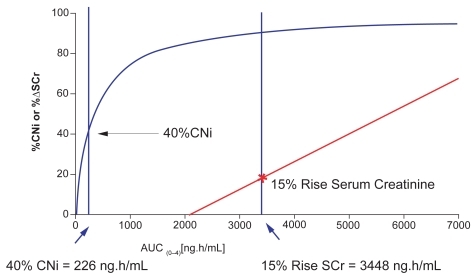
These safety data, combined with a predictable PK/PD relationship, suggest a broad therapeutic window for voclosporin. This is in stark contrast to the narrower therapeutic ranges of other calcineurin inhibitors, such as CsA and tacrolimus, which may require the use of therapeutic drug monitoring to correlate the parent substance and its metabolites with important clinical parameters (CitationStaatz and Tett 2004; CitationVollenbroeker et al 2005). Voclosporin achieved a clinically relevant range of calcineurin inhibition (40% to 70%) in phase 1 and 2a trials. Within this therapeutic range, no significant changes in creatinine clearance, mean arterial blood pressure, or serum magnesium levels have been observed. An effect of voclosporin on creatinine clearance has only been observed at a drug exposure >100% of that required to achieve 70% calcineurin inhibition (2250 vs 900 ng*h/mL) (CitationYatscoff et al 2002). More recent data indicate that 40% calcineurin inhibition is achieved with voclosporin at an AUC of 226 ng*h/mL, but a 15% rise in serum creatinine (the lower threshold of clinical significance) occurs only at an voclosporin AUC of 3448 ng*h/mL () (CitationYatscoff et al 2002; CitationIsotechnika, Inc., 2008).
Figure 4 Voclosporin therapeutic window for renal toxicity.
LUMINATE clinical trials program
Study rationale and objective
Although a number of corticosteroid-sparing immunomodulatory agents have been utilized in the treatment of uveitis over the past 2 decades, voclosporin is the first to enter into pivotal clinical trials for FDA-approval. This landmark program is being conducted in North America, Europe, and India, and will enroll over 500 patients.
The LUMINATE program comprises three randomized, double-blind, placebo-controlled, phase 2/3 trials in patients with noninfectious, sight-threatening uveitis that is active intermediate-, anterior and intermediate-, posterior-, or pan-uveitis (Study 1, LUMINATE Active); quiescent intermediate-, anterior and intermediate-, posterior-, or panuveitis in patients requiring systemic immunosuppresssion for disease control (Study 2, LUMINATE Maintenance); or active anterior in patients requiring systemic immunosuppression for disease control (Study 3, LUMINATE Anterior) (Protocol 1, 2, 3). The study designs and procedures are highly consistent with the corticosteroid-tapering paradigm used widely in clinical practice.
Enrollment criteria
summarizes selected inclusion and exclusion criteria for the three clinical trials. The primary enrollment criterion is the presence of noninfectious uveitis that is either uncontrolled despite systemic or periocular corticosteroid therapy, or that requires systemic or periocular corticosteroids and/or immunosuppressive agents for control (Protocol 1, 2, 3; Protocols 1–3 Amendments).
Table 1 Selected inclusion and exclusion criteria for the LUMINATE clinical trials program (Protocol 1, p. 22–24; Protocol 2, p. 22–25; Protocol 3, p. 20–23)
Study endpoints
The primary efficacy assessments largely follow the SUN Working Group guidelines for measurement of ocular inflammation in clinical trials (CitationJabs et al 2005). summarizes the primary and secondary endpoints for each study in the LUMINATE clinical trial program. The primary endpoint in LUMINATE Active is mean change from baseline in vitreous haze score, and in LUMINATE Anterior, mean change from baseline in anterior chamber cells. In LUMINATE Maintenance, the primary endpoint is inflammatory exacerbation, defined as a clinically significant deterioration from baseline of at least 2 grades in vitreous haze score and/or anterior chamber cells, and/or a deterioration in visual acuity of at least +0.3 LogMAR (Protocol 1, 2, 3; Protocol 1–3 Amendments). As secondary endpoints, all three trials examine changes in corticosteroid use, visual acuity, and quality of life.
Table 2 Primary, secondary, and additional endpoints of the LUMINATE clinical trial programTable Footnote* (Protocol 1, p. 18; Protocol 2, p. 18; Protocol 3, p. 17)
Study design/methodology
All studies are phase 2/3 prospective, multicenter, double-masked, placebo-controlled, parallel-group, randomized trials in patients ≥13 years of age. Enrollment at approximately 60 sites in North America, Europe, and India is expected to range from 100 for LUMINATE Anterior to approximately 210 and 220, respectively, for LUMINATE Active and LUMINATE Maintenance. In each study, patients will be randomized in a 2:2:2:1 ratio to 1 of 4 treatments: voclosporin at a dose of 0.2, 0.4, or 0.6 mg/kg bid, or placebo (Protocol 1, 2, 3).
Patients will be assessed at baseline and at weeks 2, 4, 8, 12, 16, 20, and 24 with an optional 24 week extension in the LUMINATE Active and Anterior studies; in the LUMINATE Maintenance study, assessments will be made at baseline and at weeks 2, 6, 10, 14, 18, 22, and 26 with an optional 24 week extension. Assessments include best corrected visual acuity, slit lamp exam and tonometry, dilated fundus exam, graded assessments of vitreous haze and AC cells, quality of life, and selected laboratory assessments that include CBC with differential, serum chemistry, lipid profile, and renal and liver function tests. Optical coherence tomography will be performed in the LUMINATE Active and Anterior studies while fluorescein angiography will be performed only in the former. Endothelial cell density (ECD) will be measured as a safety parameter in the LUMINATE Maintenance study (Protocols 01, 02, 03 – p12). All three trials include a standardized algorithm for tapering systemic and topical corticosteroids (Protocol 1, 2, 3).
Study treatment will be discontinued and rescue therapy administered if (1) patients with active noninfectious uveitis experience either a deterioration of at least 1 grade in vitreous haze or AC cells at week 4 or show no improvement from baseline by week 8, or (2) patients with quiescent noninfectious uveitis experience a study endpoint (ie, inflammatory exacerbation) (Protocol 1, 2, 3).
Rationale for dose selection
Preclinical and clinical data suggest that approximately 50% calcineurin inhibition (achieved with voclosporin at a dosage of 0.4 mg/kg bid) leads to a meaningful clinical effect (CitationAspeslet et al 2004; CitationGupta et al 2006). This was demonstrated in a recently conducted randomized double-blind placebo-controlled study of patients with plaque psoriasis in which voclosporin (0.4 mg/kg bid) produced 50% calcineurin inhibition and proved to be both effective and well tolerated. A dosage of 0.2 mg/kg in that study was associated with 30% calcineurin inhibition and found to be subtherapeutic (CitationGupta et al 2006; CitationLangley et al 2006).
PK/PD modeling of calcineurin inhibition suggests that bracketing the 0.4 mg/kg bid dosage with dosages of 0.2 mg/kg bid and 0.6 mg/kg bid would offer a sufficiently wide interval for dose ranging, resulting in approximately 30% to 70% calcineurin inhibition (Protocol 1, 2, 3). This dose ranging will allow investigation of any correlation between the amount of drug administered and the impact on various parameters of uveitis (eg, inflammation, macular thickening) and, ultimately, on clinical efficacy.
Additional protocol features
Optical coherence tomography
The potential effect on retinal macular thickness by voclosporin will be evaluated by means of optical coherence tomography (OCT) in the LUMINATE Active and Anterior studies. Baseline measurement in addition to measurements over the course of the trials will be undertaken.
Fluorescein angiography
Macular hyperfluorescence will be evaluated in the LUMINATE Active study as assessed by fluorescein angiography.
Quality of life
Assessments will be performed in the LUMINATE program to examine the potential effect of treatment of uveitis with voclosporin on quality of life (QoL). Among the instruments to be used are the National Eye Institute Visual Functioning Questionnaire, the Euro QoL-5, and the Short Form Health Survey.
Conclusions: Potential impact of LUMINATE findings
The LUMINATE program possesses several unique design features that will make it a landmark among clinical trials of uveitis therapies. It is the first pivotal-stage program undertaken for marketing approval of a corticosteroid-sparing agent for the treatment, control, and maintenance of all forms of noninfectious uveitis. It is also the first program to examine the correlation between dose and effects on various parameters of uveitis, including inflammation, vision, macular thickness, and angiographic changes.
If the LUMINATE program is successful, voclosporin will become the first steroid-sparing immunosuppressive drug approved by the FDA for the treatment of uveitis.
These findings could have significant implications for other ophthalmic diseases that are characterized by inflammatory mechanisms (eg, dry eye syndrome, age-related macular degeneration, and diabetic retinopathy) and vascular leakage (eg, age-related macular degeneration and diabetic macular edema).
In summary, if voclosporin proves to be an effective and safer treatment for noninfectious uveitis, inflammation will be controlled, visual acuity will be maintained, and the need to take corticosteroids will be reduced or eliminated. Voclosporin could thus represent a new standard of care offering hope for patients with this devastating condition.
Disclosures
Eddy Anglade and Sidney Weiss are founders and shareholders of Lux Biosciences, Inc; Launa Aspeslet is a shareholder of Isotechnika, Inc.
References
- [No authors listed]2007ISA 247: trans-ISA 247, trans-R 1524, ISA(TX)247, ISAtx 247, ISATx247, LX 211, LX211, R 1524, R-1524Drugs R D81031217324008
- AbelMDAspesletLJFosterRT2003ISA247 A new generation calcineurin inhibitor [abstract]Proceedings of the International Association of Therapeutic Drug MonitoringBaselSwitzerland
- AbelMMullerFFreitagD20043D structure of ISA247 correlates with improved cyclophilin binding and calcineurin inhibition [abstract]Proceedings of the 3rd International Congress on ImmunosuppressionSan Diego, CA, USA150489
- AspesletLFreitagDTrepanierD2001ISA(TX)247: a novel calcineurin inhibitorTransplant Proc3310485111267185
- AspesletLFreitagDHuizingaRB2004Pharmacokinetics-pharmacodynamics and safety of Trans-ISA247: A novel immunosuppressant [abstract]Proceedings of the 3rd International Congress on ImmunosuppressionSan Diego, CA, USA150367
- BusqueSLaftaviMGastonR2007ISA247: Preliminary results of a phase IIb multicentre, de novo renal transplant trial [abstract]Proceedings of the American Transplant Congress May 6, 200749
- ChoMlChoCSMinSY2002Cyclosporine inhibition of vascular endothelial growth factor production in rheumatoid synovial fibroblastsArthritis Rheum461202912115224
- CunninghamMALiZChanCC2007Subcutaneous injections of LX211 prevent and reverse experimental autoimmune uveoretinitis in rats [poster]Proceedings of the Association for Research in Vision and Ophthalmology Annual MeetingMay 6th–10thFort Lauderdale, FL, USAB730
- DumontFJLiebermanRMukherjeeA1996Cyclosporine A and tacrolimus (FK-506) immunosuppression through immunophilin-dependent inhibition of calcineurin functionPrinciples of Drug Development in Transplantation and AutoimmunityNew YorkChapman and Hall1175205
- DumontFJ2004ISAtx-247 (Isotechnika/Roche)Curr Opin Investig Drugs554250
- FreitagDMayoPAspesletL2006The novel immunosuppressant ISA247 demonstrates a different metabolic profile than cyclosporine A in vitro and in vivo [abstract]Proceedings of the World Transplant CongressJuly 22nd–27thBoston, MA, USA2434
- GastonRBusqueSCantarovichMfor the PROMISE Study Investigators2006ISA247: A novel calcineurin inhibitor (CNI). A promising safety profile with enhanced efficacy [poster]Proceedings of the American Society of Nephrology,San Diego, CA, USA
- GritzDCWongIG2004Incidence and prevalence of uveitis in Northern California; the Northern California Epidemiology of Uveitis StudyOphthalmology11149150015019324
- GuentherLBarberKVenderR2006ISA247 Remains a safe and efficacious agent after 48 weeks of continuous therapy: interim results of the SPIRIT Extension Study [abstract]Proceedings of the American 15th Congress of the European Academy of Dermatology and VenereologyOctober 4th–8thRhodes, Greece950670
- GuptaATomiZKunynetzR2006Pharmacokinetics and pharmacodynamics of ISA247 in a Phase III, randomized, multicentre, double-blind, placebo-controlled study [abstract]Canadian Dermatology Association 81st Annual ConferenceJune 27th–July 2ndWinnipeg, Canada
- HoSClipstoneNTimmermannL1996The mechanism of action of cyclosporin A and FK506Clin Immunol Immunopathol803 Pt 2S40S458811062
- Isotechnika, Inc.2008Data on fileIsotechnika, Inc.Edmonton, Canada
- Isotechnika, Inc.2007aPhase I study summariesAccessed July 8, 2007 URL: http://www.isotechnika.com/in_development/isa247/how/
- Isotechnika, Inc.2007bPhase 3 Canadian Psoriasis StudyAccessed July 8, 2007 URL: http://www.isotechnika.com/in_development/isa247/psoriasis
- JabsAKaramurselE2005Immunosuppression for posterior uveitisRetina2511815655435
- JabsDANussenblattRBRosenbaumJT2005Standardization of Uveitis Nomenclature (SUN) Working Group. Standardization of uveitis nomenclature for reporting clinical data. Results of the First International WorkshopAm J Ophthalmol1405091616196117
- JabsDARosenbaumJTFosterCS2000Guidelines for the use of immunosuppressive drugs in patients with ocular inflammatory disorders: Recommendations of an expert panelAm J Ophthalmol13049251311024423
- LangleyRBissonnetteRSearlesG200624 Week results of a Phase III randomized, double-blind, multicentre, placebo-controlled study of ISA247 in plaque psoriasis [abstract]Canadian Dermatology Association 81st Annual ConferenceJune 27th–July 2ndWinnipeg, Canada
- NussenblattRB1990The natural history of uveitisInt Ophthalmol1430382249907
- PappKLangleyRBissonnetteR2004A Phase III, randomized, multicenter, double-blind, placebo-controlled study of ISA247 in plaque psoriasis patients [abstract]J Am Acad Dermatol54Suppl 1P33
- SchreiberSLCrabtreeGR1992The mechanism of action of cyclosporin A and FK-506Gr Immunol Today1313642
- StaatzCETettSE2004Clinical pharmacokinetics and pharmacodynamics of tacrolimus in solid organ transplantationClin Pharmacokinet436235315244495
- StalderMBirsanTHubbleRW2003In vivo evaluation of the novel calcineurin inhibitor ISATX247 in non-human primatesJ Heart Lung Transplant2213435214672749
- VollenbroekerBKochJHFobkerM2005Determination of cyclosporine and its metabolites in blood via HPLC-MS and correlation to clinically important parametersTransplant Proc371741415919451
- WaselNGuptaATomiZ2006Pharmacokinetics and pharmacodynamics of ISA247 in a Phase III randomized, multicenter, double-blind, placebo-controlled study [abstract]J Am Acad Dermatol54Suppl 1P36
- YatscoffRWBroskiAPAbelMD2002Phase 2 trial results of ISATX247, a novel calcineurin inhibitor with a therapeutic window [abstract]Proceedings of the IXI International Congress of The Transplantation SocietyMiami, FL, USA0471
- YatscoffRWAbelMDAspesletLJ2003Phase 2 randomized, multicenter, open-label study of ISA247 and Neoral in post-renal transplant patients [abstract]Proceedings of the American Transplant CongressWashington DC, USA1215