Abstract
Background
To determine occurrence of features of intraoperative floppy iris syndrome (IFIS) during cataract surgery in patients taking systemic alpha-antagonists (AA).
Methods
We prospectively studied patients on AA and who underwent phacoemulsification. The following were recorded: pupil diameter preoperatively, iris flaccidity, iris prolapse and peroperative miosis.
Results
We studied 40 eyes of 31 subjects. Mean age was 78 years. Overall, 14 eyes (13 patients) showed signs of IFIS: 9/13 (69%) eyes of patients on tamsulosin, 1/18 (6%) eyes in the doxazosin group, 2/2 prazosin patients, 1/4 eyes in the indoramin group, and 1/2 eyes in two patients on a combination of doxazosin and tamsulosin. Most cases (92%) had only one or two signs of IFIS. Bilateral cataract surgery was undertaken in 9 patients but only one patient (on tamsulosin) had features of IFIS in both eyes, while 4 patients (2 on tamsulosin and 2 on other AA) showed signs of IFIS in one eye only, and 4 patients did not show IFIS in either eye.
Conclusion
Most AA were associated with IFIS, but it tends to present as a spectrum of signs rather than full triad originally described. Tamsulosin was most likely to be associated with IFIS; however, its intake does not necessarily mean that IFIS will occur. For patients on AA, the behavior of the iris intraoperatively in one eye is a poor predictor of the other eye. Surgeons should anticipate the occurrence of IFIS in any patient on AA.
Introduction
CitationChang and Campbell (2005a) were the first to describe the intraoperative floppy iris syndrome (IFIS) which is characterized by the triad of: a flaccid iris stroma that undulates and billows in response to ordinary intraocular fluid currents, a propensity for the floppy stroma to prolapse towards the phaco and side-port incisions despite proper wound construction, and progressive intraoperative pupil constriction despite standard preoperative pharmacologic measures designed to prevent this. They, and later other authors, found a strong association between IFIS and systemic use of tamsulosin, a selective α1A and α1D adrenergic receptor antagonist (AA) (CitationParssinen 2005).
CitationSchwinn and Afshari (2005a) later suggested that IFIS can be associated with other commercially available nonselective AA. Some case reports have implicated the use of alfuzosin and doxazosin with IFIS (CitationChang and Campbell 2005b; CitationSettas and Fitt 2006). However, a recent study has reported that nonselective AA are unlikely to be associated with IFIS (CitationChadha et al 2007). In this prospective descriptive study, we aim to determine the occurrence of the features of IFIS during cataract surgery in patients taking all types of AA.
Methods
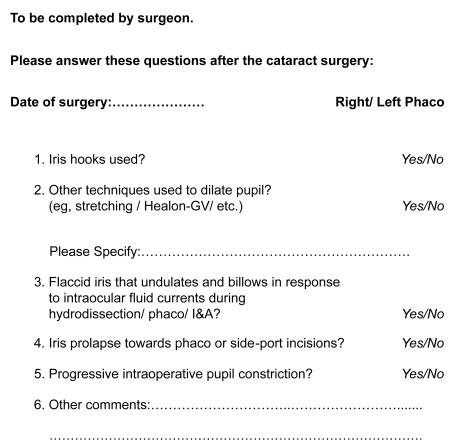
This is a prospective descriptive case series. Patients were enrolled at preoperative assessment for cataract surgery at a large university hospital ophthalmology department. Inclusion criteria were patients on alpha-blockers. Exclusion criteria were previous ocular trauma, surgery or pseudoexfoliation. Surgery was carried under the care of 6 consultants between March and October 2006. A standard pupil dilation regimen of 1 drop of cyclopentolate 1% and phenylephrine 2.5% was used. Pupil diameters pre and post-dilation were measured by two observers (OH and SI) using a pupil gauge, in the same lighting conditions (mesopic). All patients underwent phacoemulsification. The surgeon was not masked to the type of AA the patient was using. A standard questionnaire () was filled in by the surgeon after the surgery. Data was recorded from this questionnaire and by review of hospital notes. All methods have followed the Tenets of the Declaration of Helsinki. Patients continued taking their regular AA medications as usual before the surgery.
Figure 1 Alpha-blockers and intraoperative floppy iris syndrome surgeon questionnaire.
Demographics and AA used were recorded. Outcome variables were pre- and post-dilation pupil size, and intra-operative evidence of IFIS (iris flaccidity, tendency of iris to prolapse and miosis during surgery). Peroperative complication rates were also recorded.
Data were stored and analyzed by Excel (2000; Microsoft Corporation, Redmond, WA). Differences between numerical data for pupil size were assessed by the unpaired Student two-tailed t-test. A P-value of less than 0.05 was considered statistically significant.
Results
Thirty-one patients (40 eyes) were included in this study. Mean age (±standard deviation [SD]) was 78 (±7.4), and 58% were male and 42% were female. Only one patient was Asian and the rest were Caucasian.
shows the use of alpha-blockers in these patients.
Table 1 Alpha blocker treatment, indication, dosage, affinity to alpha receptor subtypes and gender
Pupil diameter
Pupil diameter means are shown in . There was no significant difference between the pre- and postdilation pupil sizes in the two groups (tamsulosin and nontamsulosin groups) (). There was no significant difference between diabetic and nondiabetic patients. However, the method used to measure pupil diameter in this study has significant intra- and interobserver variability and this limits the reliability of our values. Furthermore, a larger number of patients are required to detect a statistically significant difference between pupil diameters in the two groups.
Table 2 Mean pupil diameter (in millimeters) before and after dilation with cyclopentolate 1% and phenylephrine 2.5%
IFIS
Overall, 13 patients (14 eyes) showed some signs consistent with IFIS () and (). The majority of these patients (9 patients (10 eyes)) were on tamsulosin. The most frequent sign of IFIS was iris flaccidity; 11 of 14 cases, followed by iris prolapse 7 of 14 cases. In many cases intraoperative miosis was difficult to comment on as intraoperative intervention was used.
Figure 2 Incidence of intraoperative floppy iris syndrome (IFIS) with different alpha antagonists.
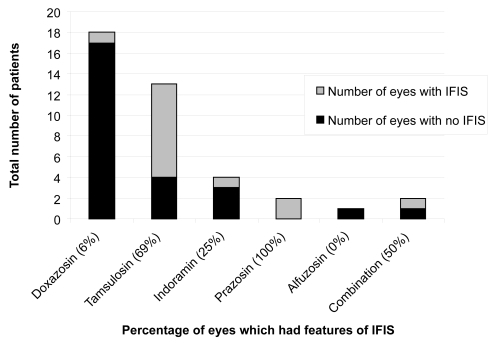
Table 3 Patients who had features of intraoperative floppy iris syndrome
Tamsulosin
In the tamsulosin group (13 eyes), 9 eyes (69%) showed at least one of the signs of IFIS (). The majority (7 eyes) showed only one of the signs of IFIS and two eyes showed 2 signs. None of the tamsulosin eyes showed the full-blown syndrome (although iris intervention was used in several cases which would prevent all the signs of IFIS becoming manifest). Eight eyes in this group (62%) had some intra-operative intervention to minimize the effect of IFIS. Iris hooks were used in 6 eyes and intracameral phenylephrine was used in 2 (including one patient as a precaution, who showed no signs of IFIS.
Nontamsulosin AA
In the doxazosin group (18 eyes), only 1 eye (6%) demonstrated the IFIS triad. The rest of the irides behaved normally intra-operatively. Interestingly, the two patients, who were taking prazosin, showed signs of IFIS and one of them needed intracameral phenylephrine to stabilize the iris. Only 1 eye (25 %) in the indoramin group showed signs of IFIS that required insertion of iris hooks to minimize iris billowing. The only patient with a history of alfuzosin use in this series showed normal iris behavior intraoperatively.
Effect of simultaneous use of two alpha-blockers
Two patients were on both tamsulosin and doxazosin. One eye of one of these patients showed signs of IFIS.
Bilaterality of IFIS
Bilateral cataract surgery was undertaken in 9 patients (18 eyes) in this series. Only one patient showed signs of IFIS in both eyes and that patient was on tamsulosin. Four patients (62%) showed signs of IFIS in one eye only (2 on tamsulosin, 1 on doxazosin, and 1 on indoramin). Four patients did not show signs of IFIS in either eye (1 on tamsulosin, 2 on doxazosin, and 1 on indoramin) ().
Table 4 Occurrence of intraoperative floppy iris syndrome (IFIS) in patients who had bilateral cataract surgery.
Gender
Most patients who showed features of IFIS were male (92%). Only one female showed signs of IFIS (indoramin). All female patients were on doxazosin, except one who took indoramin ().
Diabetes mellitus
Two out of 13 (15%) patients with features of IFIS (one on prazosin and the other on combination of doxazosin and tamsulosin) had diabetes mellitus compared to 2/19 (10.5%) patients in the non-IFIS group. However, the number of subjects was too small to perform any meaningful statistical test.
Intraoperative complications
No significant complications were documented in our series.
Discussion
Our study confirms the association between tamsulosin and IFIS as was initially described (CitationChang and Campbell 2005a). Sixty-nine percent of eyes of patients on tamsulosin showed signs of IFIS which is similar to the incidence of 57% quoted by CitationChadha and colleagues (2007) but significantly less than the 100% risk quoted by CitationChang and Campbell (2005a) in their prospective study. The fact that 31% of eyes did not demonstrate any features of IFIS means that other cofactors (eg, physiological response to AA, pharmacodynamics, pharmacokinetics, systemic or ocular pathology) may play role in which patients get IFIS. IFIS cases could have been under-reported because of use of prophylactic intraoperative measures, short exposure to AA and different threshold of reporting IFIS by different surgeons. However, the rate of IFIS incidence in our study is similar to Chang’s larger study, in which surgeons also were allowed to use intraoperative prophylactic measures.
Two recent studies have studied the effect of AA on pupil diameter. The first study showed that AA (alfuzosin, doxazosin, naftopidil, prazosin, tamsulosin, and terazosin) can inhibit the mydriatic effect of phenylephrine, in vivo in rabbits (CitationMichel et al 2006). Moreover, this study showed that this inhibition can be achieved with AA doses very similar to those required to produce their desired therapeutic effect on lowering the intraurethral pressure. Also in rabbits that did not receive phenylephrine, all AA induced miosis at considerably higher doses but tamsulosin was more potent than the others which could be attributed to its affinity to α1A receptors. The second study looked at the effect of tamsulosin and alfuzosin effect on pupil diameter in humans. Pupil diameter decreased under mesopic and scotopic light after treatment with tamsulosin, but only scotopic pupil diameter decreased after treatment with alfuzosin (CitationAltan-Yaycioglu 2007). Both drugs had no significant effect on dilated pupil measurements. In our study, there was no significant difference in the mesopic and dilated pupil diameter between the two groups (tamsulosin and other AA groups).
The association between IFIS and other commercially available AA (alfuzosin, doxazosin, indoramin, prazosin, and terazosin) is less clear due to the fact that these medications, with the exception of doxazosin, are less commonly used in clinical practice. There is one case report (CitationMuqit and Menage 2006) and one case series (CitationChadha et al 2007) describing the association of IFIS with doxazosin. In our series, 4 out of 25 patients taking AA other than tamsulosin had features of IFIS. To our knowledge, this is the first study to show any association between IFIS and prazosin or indoramin. The numbers are small but may indicate a difference in the incidence of IFIS with different AA: both of the patients on prazosin had features of IFIS yet only one of 18 patients on doxazosin and one eye of two patients on indoramin had signs consistent with IFIS. The only patient on alfuzosin had stopped the drug a few months previously and did not have signs of IFIS. We did not have any patients on terazosin; however, in the CitationChadha and colleagues (2007) series there was one patient on this AA but they did not have IFIS.
Diabetes mellitus was slightly more prevalent in the IFIS group but we cannot comment on statistical significance due to the small numbers involved. CitationChadha and colleagues (2007) reported no evidence that diabetes contributes to features of IFIS although it was associated with small pupil. However, we did not find a significant difference in pupil size after dilation between diabetic and nondiabetic patients probably due to the small number of diabetic subjects.
There may be an important element of individual susceptibility to IFIS but is the occurrence of this syndrome consistent between eyes in any given individual? Interestingly, this does not seem to be the case. Of the four patients on tamsulosin undergoing bilateral cataract surgery, only one had IFIS in both eyes and two had IFIS in only one eye. Similarly, of the five patients on other alpha-blockers who underwent bilateral cataract surgery, the two who showed features of IFIS had it in one eye only. This different behavior in the two eyes of the same patient has also been reported by other authors including Schwinn and Afshari (CitationManvikar and Allen 2006; CitationSchwinn and Afshari 2006). It is difficult to explain given that individual susceptibility, drug kinetics, and drug dose would have been expected to be similar for both eyes. However, there could have been different surgical wound construction techniques and fluid flow mechanics since different surgeons have been involved and this could explain, in part, IFIS predisposition as a local event (CitationSchwinn and Afshari 2006). Of the four patients who had bilateral cataract surgery and unilateral IFIS, 2 showed signs of IFIS in the first eye and 2 in the second. In all 4, the fellow eye showed no features of IFIS during surgery and required no prophylactic measures. These findings suggest that surgeons should be aware of the possible occurrence of IFIS in second eye surgery of patients on all types of AA even if there were no IFIS features in the first eye.
It is also of interest that only one of the two patients on combined tamsulosin and doxazosin treatment showed features of IFIS. There have been no previous reports regarding the occurrence of IFIS in patients receiving combinations of AA. However, the numbers are too small to reach any conclusion.
Some authors have suggested stopping AA before elective cataract surgery to reduce the risk of complications due to IFIS (CitationManvikar and Allen 2006; CitationSchwinn and Afshari 2006). A recent survey reported that 68% of consultants in the UK had patients discontinue tamsulosin preoperatively, but they found no consistent benefit from this protocol (CitationNguyen 2007). In our series, all patients continued their AA treatment and there were no intraoperative complications. This is most likely due to the use of intraoperative measures (eg, iris hooks and intracameral phenylephrine) to limit the effect of IFIS features which is in agreement with other authors (CitationManvikar and Allen 2006; CitationNguyen 2007). Intraoperative prophylactic measures in our study were performed at the beginning of surgery which could have influenced the number of reported IFIS cases and their severity. However, in 8 of 14 eyes which developed IFIS, prophylactic measures were used but iris flaccidity and prolapse were still observed in some of these cases to make diagnosis of IFIS possible. Intraoperative measures were used only in 4 of 26 eyes which did not have IFIS.
The major limitations in our study include the factor that a number of different surgeons were involved who may have had different thresholds for diagnosing the features of IFIS. However, the fact that our IFIS incidence in the tamsulosin group is similar to the incidence quoted in the literature suggests that we were diagnosing IFIS appropriately. Also, surgeons were allowed to use intraoperative prophylactic measures against IFIS which could have led to masking of IFIS signs in some patients. Again, however, the fact that our IFIS incidence in the tamsulosin group is similar to the literature suggests that this was not a problem. Another limitation was that the surgeon was not masked to the type of AA. This could have resulted in detection bias in the nontamsulosin group because of a lower threshold for reporting IFIS in association with AA other than tamsulosin.
Other confounding factors can influence the occurrence of IFIS such as the duration of AA therapy. The preoperative questionnaire was taken at least four weeks before surgery. The actual duration of therapy was not included in our questionnaire. However, the actual minimum duration of exposure to AA that is required to cause IFIS is not known yet. This may explain the fact that not all patients on an AA developed IFIS. However, a recent report found that IFIS can happen after 2 weeks of starting tamsulosin treatment (CitationChang et al 2007). Finally, co-existing systemic illnesses other than diabetes (eg, cardiovascular diseases, autonomic nervous dysfunction) and other systemic medications that could have some side effects on iris behavior can influence IFIS presentation.
In conclusion, the trends suggest that a larger study into the incidence of IFIS in patients on alpha-blockers other than tamsulosin and doxazosin is warranted. In the meantime, all surgeons should be aware of the possible occurrence of IFIS in one of both eyes of any patient on AA.
Disclosure
The authors report no conflicts of interest in this work.
References
- Altan-YayciogluRYayciogluOGulU2007The effects of two systemic alpha1-adrenergic blockers on pupil diameter: a prospective randomized single-blind studyNaunyn Schmiedebergs Arch Pharmacol37519920317394035
- ChadhaVBoroohaSTeyA2007Floppy iris behaviour during cataract surgery: associations and variationsBr J Ophthalmol9140216943229
- ChangDFCampbellJR2005aIntraoperative floppy iris syndrome associated with tamsulosinJ Cataract Refract Surg316647315899440
- ChangDFCampbellJR2005bReply: Intraoperative floppy iris syndrome associated with tamsulosin [letter]J Cataract Refract Surg312241
- ChangDFOsherRHWangL2007Prospective multicenter evaluation of cataract surgery in patients taking tamsulosin (flomax)Ophthalmology1149576417467530
- ManvikarSAllenD2006Cataract surgery management in patients taking tamsulosin staged approachJ Cataract Refract Surg3216111417010855
- MichelMCOkutsuHNoguchiY2006In vivo studies on the effects of alpha1-adrenoceptor antagonists on pupil diameter and urethral tone in rabbitsNaunyn Schmiedebergs Arch Pharmacol3723465316489448
- MuqitMMMenageMJ2006Intraoperative floppy iris syndrome [letter]Ophthalmology1131885617011965
- NguyenDQSebastianRTKyleG2007Surgeon’s experiences of the intra-operative floppy iris syndrome in the United KingdomEye21443417057648
- ParssinenO2005The use of tamsulosin and iris hypotony during cataract surgeryActa Ophthalmol Scand83624616188009
- SchwinnDAAfshariNA2005α1-Adrenergic antagonists and floppy iris syndrome: tip of the iceberg?Am J Ophthalmol112205960
- SchwinnDAAfshariNA2006Alpha(1)-Adrenergic receptor antagonists and the iris: new mechanistic insights into floppy iris syndromeSurv Ophthalmol515011216950249
- SettasGFittAW2006Intraoperative floppy iris syndrome in a patient taking alfuzosin for benign prostatic hypertrophyEye201431216498436