Abstract
Purpose
To investigate whether serum levels of soluble Fas (sFas) and interleukin-6 (IL-6) could function as an index of the efficacy of steroid pulse treatment, we examined the serum level of these proteins before and after steroid pulse treatment in thyroid-associated ophthalmopathy patients.
Methods
We gathered the blood of thyroid-associated ophthalmopathy patients before or after steroid pulse treatment, obtained serum with a centrifuge, and measured the serum levels of sFas and IL-6 by enzyme-linked immunosorbent assay (ELISA).
Results
There was no difference in serum IL-6 value between pre- and poststeroid pulse treatment. Serum sFas value was significantly decreased in both pre- and poststeroid pulse treatment. Furthermore, there was a recognizable improvement in the degree of the extraocular muscle thickening after treatment in cases in whom the serum sFas value was lower than 3 ng/ml prior to the beginning of the therapy. In patients who had a serum sFas value of more than 3 ng/ml, there was no improvement in the degree of thickening of the extraocular muscle.
Conclusions
Serum level of sFas is an accurate index of the outcome of steroid pulse treatment in thyroid-associated ophthalmopathy and may become a useful index to gauge the status of convalescence.
Introduction
Thyroid-associated ophthalmopathy is an autoimmune disease characterized by exophthalmos, increment of intraocular pressure, lid swelling, visual field loss, and diplopia. These symptoms appear with hyperthyroidism, however they are not, with the exception of the latter, always recognized. Sato demonstrated a cross section of the extraocular muscle in computed tomography, and reported a method to judge the effect of steroid pulse treatment of thyroid associated ophthalmopathy (CitationKenji et al 2003). Most of the reports indicate that there is no hematologically curative effect for this disease. However the fact that levels of soluble Fas (sFas) and interleukin-6 (IL-6) were reported to be extremely high in thyroid-associated ophthalmopathy (CitationSiddiqi et al 1999; Citationvan Lopik et al 1999), led us to speculate whether they could function as markers for the curative effect of therapy for this autoimmune disease.
Patients and methods
Thirty-one hospitalized patients (11 men and 20 women) suffering from thyroid-associated ophthalmopathy were examined at Sapporo Medical University Hospital between December, 1999 and January, 2000. The mean age of the patients was 48.67 years (range, 22 to 62), men 54 years (range, 41 to 62) and women 45.7 (range, 22 to 62). Patients were admitted to hospital on the basis of a clinical activity score of 4 or more, or diplopia, or deterioration in visual acuity within the previous three months (CitationHeufelder and Joba 2000). The treatment was as follows; 1000 mg intravenous methylprednisolone each day for four days and thereafter 30 mg administration of prednisolone each day for three days performed as 1 unit. The patients received 3 units in total. We obtained informed consent from the patients for preparation of the plasma samples before and after steroid pulse treatment. The serum was divided and used for each measurement of sFas and IL -6. The serum levels of sFas and IL-6 were measured with an SFAS enzyme-linked immunosorbent assay (ELISA) kit purchased from MBL company (Nagoya, Japan) and an IL-6 ELISA kit purchased from Dainippon Pharmaceutical Corporation, respectively. Each value was measured at an absorbance (vice-wavelength 620 nm) of 450 nm with an automatic spectrophotometer. We examined the degree of extraocular muscle thickness by a coronal 2 mm section the computed tomography (Aquilion, Toshiba Medical System, Japan) at pre- and poststeroid pulse treatment. The area of the greatest thickening of the selected extraocular muscle was used to assess the effect of steroid pulse treatment.
Results
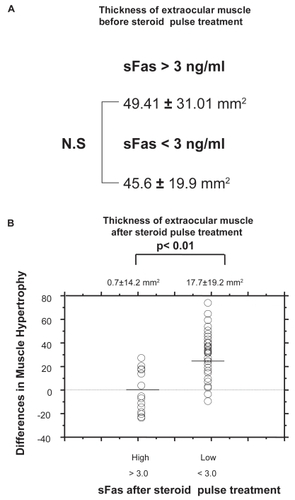
shows the maximum area of the extraocular muscle of each patient at before and after steroid pulse treatment. The extent of the extraocular muscle had decreased after treatment in comparison with before therapy. The difference in the degree of thickness of the extraocular muscle subsequent to treatment was statistically significant (p < 0.001). Before treatment, the serum level of sFas was 2.4 ± 0.9 ng/ml, whereas after treatment it was 2.1 ± 0.9 ng/ml. The serum level of sFas revealed a significant difference between before and after treatment (p < 0.01). The serum level of IL-6 was 20.2 ± 11.1 pg/ml after treatment, however the value before treatment was 17.3 ± 6.9 pg/ml, indicating no significant difference. The changes in serum level of sFas in each patient are shown in . As can be seen, after the therapy there were two groups of patients: those exhibiting changed serum levels of sFas and those showing no change. Patients with a high level of sFas prior to treatment tended to have a similarly high level even after steroid pulse treatment. Two categories of sFas values were disclosed, a high value group in both pre- and poststeroid pulse treatment and another one (). A decrease in sFas value was recognized after steroid pulse treatment in the patients who had a low sFas value before steroid pulse treatment, whereas patients with a high level maintained this level after steroid pulse treatment. shows the relationship between improvement in the degree of thickening of the extraocular muscle and sFas at pre- and poststeroid pulse treatment. In cases in whom sFas level was less than 3 ng/ml before steroid pulse treatment, the average width of the cross section of extraocular muscle was 45.6 ± 19.9 mm2, and in cases in whom sFas level was more than 3 ng/ml this average cross-section was 49.41 ± 31.01 mm2. As shown in , no significant difference was found in the width of the cross-sectional area of the extraocular muscle between these 2 groups. A comparison of the more than 3 ng/ml and less than 3 ng/ml sFas groups in terms of improvement in the degree of the extraocular muscle thickness revealed an average of 17.7 ± 19.2 mm2 and 0.7 ± 14.4 mm2 for the width of the cross-sectional area of the extraocular muscle, respectively (). This represented a significant improvement in the low level sFas group by steroid pulse treatment (p < 0.001). The value of IL-6 increased in only 2 subjects after treatment, and in all the other subjects there were hardly any changes at all ().
Figure 1 This shows the degree of extraocular muscle thickening in coronal slice pre- and poststeroid pulse treatment.
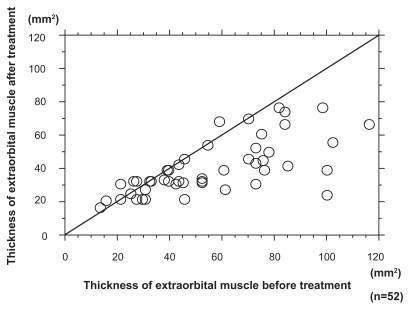
Figure 2 We gathered serum from pre- and poststeroid pulse treatment patients and measured sFas/IL-6. A shows the changes in sFas value. Student t-test revealed the value of sFas to be significantly decreased following steroid pulse treatment (student t test, p < 0.01). B shows the changes in IL-6. IL-6 did not decrease in either pre- or poststeroid pulse treatment.
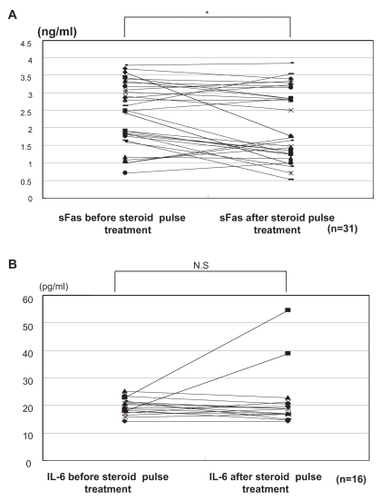
Figure 3 This shows the serum level of sFas before and after steroid pulse treatment.
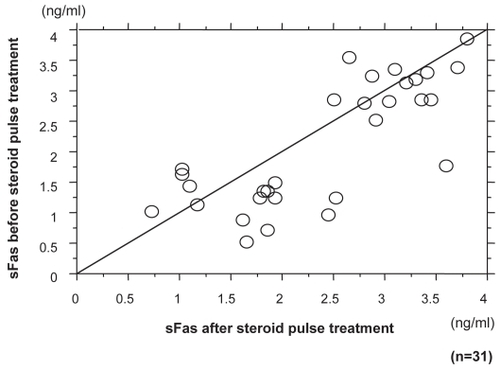
Figure 4 A shows the cross-section area of extraocular muscle before steroid pulse treatment. No significant difference in the cross-section area of extraocular muscle was observed between subjects with sFas levels of less than 3 ng/ml and those with more than 3 ng/ml. B shows those with sFas level of less than 3 ng/ml after steroid pulse treatment disclosed improvement in extraocular muscle thickness (Man-Whitney’s U test).
Discussion
A rise in IL-6 due to autoimmune disease has been reported (CitationUysal et al 1999). The increase of IL-6 can lead to a proliferation of hemaocytes, immunoresponse, inflammatory reaction, and an increase in the number of cells in the nervous system. In thyroid-associated ophthalmopathy, accumulation of glycosaminoglycan to orbital adipose tissue and connective tissue of the extraocular muscle is seen by histopathology along with lymphocyte permeation to the tissues (CitationProphet et al 2001), and there are some reports of a rise in the serum level of IL-6 at the same time (CitationWakelkamp et al 2000; CitationKozora et al 2001). IL-6 production can be controlled by steroid treatment. The fact that IL-6 is associated etiologically with thyroid-associated ophthalmopathy (CitationSiddiqi et al 1999). It means that measurement of IL-6 is useful for the treatment of this disease (CitationWakelkamp et al 2000). However, in our experiment, since serum IL-6 level hardly changed after steroid pulse treatment, except in two cases, it appears that its use as a marker for the curative effect of steroid pulse treatment in thyroid-associated opthalmopathy is dubious. sFas is thought to be produced as a result of a living body protective reaction against apoptosis in Fas/sFas (CitationCheng et al 1994). Ohtsuka reported a normal control serum level of sFas was 0.93 (SD 0.32) ng/ml, and a the high level of sFas in the extraocular muscle thickening group of his study and an association between extraocular muscle disorder and sFas was suggested (CitationOhtsuka and Hashimoto 2000). In our study, a serum level of sFas of less than 3 ng/ml and a decrease in sFas value after steroid pulse treatment was indicative of a significant improvement in the degree of thickening of the extraocular muscle. When sFas was over 3 ng/ml after treatment, improvement in the degree of thickening of the extraocular muscle did not occur, even though steroid pulse treatment had been performed. Our results suggest that the pretreatment level could be useful as a predictive parameter of the curative response to the steroid pulse therapy for thyroid-associated ophthalmopathy.
Disclosure
The authors report no conflicts of interest.
References
- ChengJZhouTLiuC1994Protection from Fas-mediated apoptosis by a soluble form of the Fas moleculeScience26351541759627510905
- HeufelderAEJobaW2000Thyroid-associated eye diseaseStrabismus81011110980691
- KenjiOSatoAKawaguchiSHashimotoM2003Effect of steroid pulse therapy with and without orbial radiotherapy on Grave’s opthalmopathyAm J Opthalmol13528590
- KozoraELaudenslagerMLemieuxA2001Inflammatory and hormonal measures predict neuropsychological functioning in systemic lupus erythematosus and rheumatoid arthritis patientsJ Int Neuropsychol Soc77455411575596
- OhtsukaKHashimotoM2000Serum levels of soluble Fas in paitents with Graves’ophthalmopathyBr J Ophthalmol84103610611108
- ProphetHMaticGBWinklerRE2001Two cases of refractory endocrine ophthalmopathy successfully treated with extracorporeal immunoadsorptionTherapeutic Apheresis5142611354299
- SiddiqiAMonsonJPWoodDF1999Serum cytokines in thyrotoxicosisJ Clin Endocrinol Metab84435910022397
- van LopikTHartMBMBoeijeL1999Patients with systemic lupus erythematosus with high plasma levels of sFas risk relapseJ Rheumatol266079918241
- UysalARCorapciogluDTonyukukVC1999Effect of octreotide treatment on Graves’ ophthalmopathyEndocrin J465737
- WakelkampIMGerdingMNVan Der MeerJW2000Both Th1- and Th2-derived cytokines in serum are elevated in Graves’ ophthalmopathyClin Exp Immunol121453710971510