Abstract
Purpose
To report a case with anterior and posterior nodules associated with systemic sarcoidosis.
Methods
A patient with decreased vision underwent complete ophthalmologic examination, ultrasound biomicroscopy, fluorescein and indocyanine green (ICG) angiography.
Results
The patient presented a nodule of the iris of the OS and of the optic nerves of both eyes. Chest computed tomography and tissue biopsy established the diagnosis.
Conclusions
Fluorescein and ICG angiography are the only objective exams to demonstrate the extent of ocular involvement in a patient with sarcoidosis.
Case report
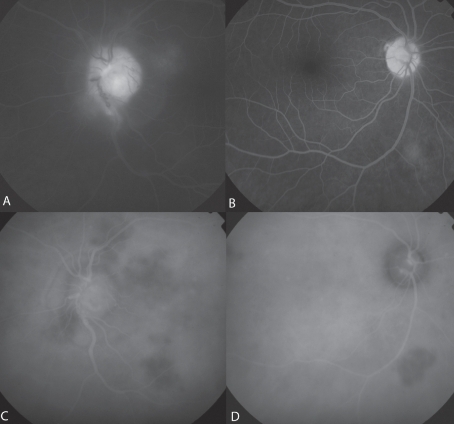
A 19-year-old black man noticed decreased vision in his OS for approximately 2 months. At presentation best-corrected visual acuity measured with a standard Snellen chart was 0.8 OS and 1.0 OD. Slit-lamp examination revealed the presence of a granulomatous nodule of the iris of the OS (), also detected by ultrasound biomicroscopy (UBM) (). Fundus examination showed a voluminous granuloma of the optic nerve of OS () and a granulomatous lesion of the OD, more visible on fluorescein angiography (), which shows optic disc leakage of OS and hyperfluorescence of OD. Multifocal choroidal lesions located in the posterior pole of the OS only visible with indocyanine green (ICG) were demonstrated ().
Figure 1 A, Large granuloma of the iris of OS. Keratic precipitates located on the lower part of corneal endothelium are also visible. B, Ultrasound biomicroscopy shows an homogenous, cystic-like lesion of the angle.
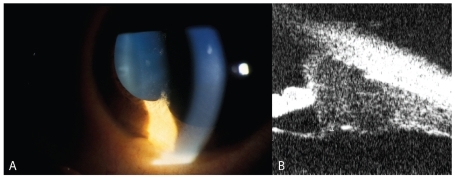
Figure 2 Fundus photograph OS shows the optic nerve granuloma caused by direct sarcoid tissue infiltration.
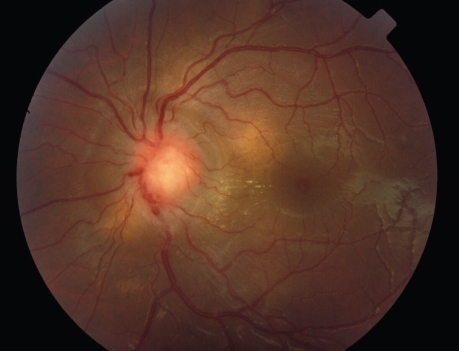
Figure 3 A, Late-phase fluorescein angiogram OS showing optic disc leakage secondary to uveitis. B, Late-phase fluorescein angiogram OD exhibits an hyperfluorescent area corresponding to the granuloma. C, Late-phase ICG angiogram OS reveals multiple choroidal hypofluorescent lesions of the posterior pole, optic disc leakage secondary to uveitis. D, Late-phase Indocyanine angiogram OD showing a single hypofluorescent area corresponding to the granuloma.
Systemic medical and laboratory work-up was performed in order to diagnose the granulomatous disease. Chest computed tomography showed hilar adenopathy. A tissue biopsy obtained from the nose proved the presence of noncaseating granuloma. The diagnosis of systemic sarcoidosis was established.
Sarcoidosis is a chronic multisystemic granulomatous disorder thought to result from an exaggerated cellular immune response to a variety of self antigens or nonself antigens (CitationNewman et al 1997). The disease affects predominantly the lungs and thoracic lymph nodes, skin and eyes (CitationMargolis 2007; CitationChan et al 2007). In this case report, the fluorescein angiography remains a standard technique for monitoring the posterior segment activity. However, only the ICG angiography was capable of demonstrating the widespread extent of choroidal involvement.
Disclosure
The authors report no financial support or conflicts of interest in this work.
References
- ChanSMHudsonMWeisE2007Anterior and intermediate uveitic cases referred to a tertiary centre in AlbertaCan J Ophthalmol42860418033328
- Margolis2007SarcoidosisCurr Op Ophthalmol184705
- NewmanLSRoseCSMaierLA1997SarcoidosisN Engl J Med3361223349110910