Abstract
Toxoplasma retinochoroiditis in pregnancy may create considerable patient anxiety and is a dilemma for the treating ophthalmologist. A case report highlighting this clinical issue is presented followed by a review of the literature. Consensus in relation to the management of toxoplasma retinochoroiditis in pregnancy is lacking and is discussed.
Keywords:
Case report
A 31-year-old immunocompetent female in the 9th week of her first pregnancy attended the emergency eye clinic with a one-week history of painless blurred vision in the right eye.
Previous ocular history included right toxoplasma retinochoroiditis when aged 11 years, and an episode of undiagnosed blurred vision in the same eye three years previously. She was otherwise in good general health.
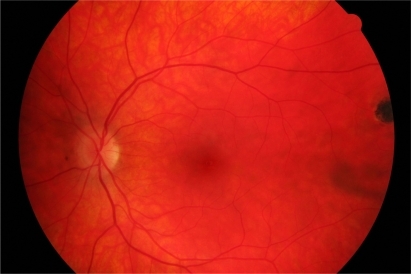
On examination, best-corrected visual acuity was 6/18 RE and 6/6 LE. There was no ciliary injection in the right eye. 3+ cells with keratitic precipitates were present in the right anterior chamber. Posterior synechiae were absent. 1+ vitreous cells with vitreous veils were present. Fundoscopy showed a raised pale ‘satellite lesion’ at the right macula with three adjacent chorioretinal scars. The optic disc was mildly swollen (). An inactive scar was also evident in the temporal fundus of the left eye ().
Figure 1 Recurrent toxoplasma retinochoroiditis. A ‘satellite lesion’ associated with pre-existing retinochoroidal scars is present at the right macula. The lesion became inactive over a period of several weeks. The acute retinochoroiditis extended temporally from the fovea.
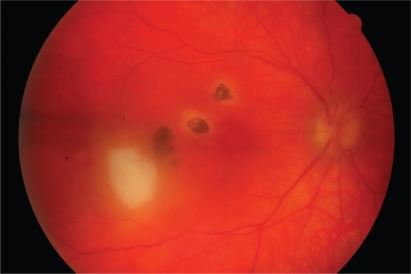
Figure 2 Inactive chorioretinal scar in temporal periphery of left eye.
We diagnosed recurrent ocular toxoplasmosis with macular involvement. Investigations at presentation included negative toxoplasma immunoglobulin M (IgM).
The patient was treated with intensive topical steroid and a mydriatic only, avoiding the use of systemic antimicrobial and steroid medications. The obstetric team maintained close surveillance on the pregnancy. Over the next few months, there was gradual clinical improvement and the topical steroids were slowly tapered. At 22 weeks of gestation, visual acuity had improved to 6/9 RE. The intraocular inflammation had settled and the retinal lesion appeared flatter with the edges starting to pigment. Five months after first presentation, the retinal lesion had become quiescent and visual acuity was 6/6.
Discussion
Toxoplasmosis is caused by the obligate intracellular protozoan Toxoplasma gondii.
Recurrent ocular disease is a common cause of posterior uveitis and may be sight-threatening, particularly if lesions involve the macula or severe intraocular inflammation is present. Immunocompetent patients usually have only one focus of active retinal disease. The retinitis usually resolves by two months, although associated intraocular inflammation may take longer.Citation1 The process underlying reactivation of the parasite in the retina is not known.
Pregnancy may create a change in the hormonal or immunological environment of the mother that favours reactivation of ocular toxoplasmosis.Citation2,Citation3 Bosch-Driesden and colleagues reported that seven (9%) of 82 women with ocular toxoplasmosis developed recurrences during pregnancy.Citation4 Reports are conflicting as to whether or not pregnancy is associated with more aggressive recurrences.Citation3,Citation5
It is accepted that primary infection in healthy women or reactivated infection in immunocompromised women can result in transplacental transmission if not treated, resulting in congenital toxoplasmosis.Citation6 Systemic treatment has been shown to decrease the rate of transmission as well as the incidence of congenital toxoplasmosis.Citation7 Management of such clinical scenarios is therefore more defined, and the use of toxic treatments more justifiable. Furthermore, most ophthalmologists would consider systemic treatment (including aggressive efforts with multiple therapy) in immunocompetent patients with ocular toxoplasmosis presenting with lesions involving the macula or in close proximity to the optic disc.
However, reactivation of toxoplasma retinochoroiditis threatening vision during the first trimester of pregnancy in a healthy female presents a difficult management problem. This view is supported by the results of a US survey of 457 ophthalmologists in which almost 25% of retinal subspecialists and 40% of general ophthalmologists were “not sure” how they would manage a pregnant patient with recurrent ocular toxoplasmosis and normal immune function.Citation8
We reviewed the published evidence so that we could determine an optimal management strategy and, at the same time, provide the patient with information to address her concerns about any increased risk to both her own health and that of her unborn child from treatment or nontreatment. We found the published studies fell broadly into three main categories: (1) clinical and laboratory diagnosis to support or preclude intervention, (2) the risk of fetal infection associated with reactivated ocular toxoplasmosis in the mother, and (3) the risk of not treating the mother vs potential teratogenicity associated with some antitoxoplasma agents. The literature review was based on comprehensive Medline and Embase searches generating references on ocular toxoplasmosis published predominantly in the last 20 years.
Investigations
Diagnosis of ocular toxoplasmosis is primarily based on clinical findings. However, a wide spectrum of clinical features may be present making the distinction with other causes of retinochoroiditis problematic.Citation9 In some cases, difficulty may exist in differentiating primary and reactivated ocular disease, thereby making the evaluation of the risk of transplacental transmission and the need for therapy difficult to assess.Citation10
It is well accepted that the role of serological investigation in the management of ocular toxoplasmosis is limited.Citation11 However, serological tests may be used as supportive evidence to confirm the suspected clinical diagnosis, particularly in complex cases. Such investigations may also be warranted in pregnant patients in whom there is a conflict between the potential benefits of treatment and the risk of treatment toxicity to the fetus.
Serological changes in acute systemic infection include the presence of anti-T. gondii IgM in serum and a rising or significantly raised level of anti-T. gondii IgG.Citation12 Anti-T. gondii IgM levels may be detectable for at least 18 months following acute infection.Citation11 Detection of anti-T. gondii IgA in serum has also been reported to be helpful in the diagnosis of recently acquired infections.Citation12 The high prevalence of anti-T. gondii IgG in an asymptomatic, ‘normal’ population makes the value of its detection somewhat limited.Citation13
In patients with retinochoroidal reactivation, there are often no serological changes to aid the clinician, and the diagnosis is weighted on clinical examination. Peripheral parasitemia is typically negative, suggesting reactivation is localized to the eye. Invasive procedures have been used to determine intraocular antibody production or to detect T. gondii DNA by polymerase chain reaction (PCR) of aqueous or vitreous humor samples.Citation14 However, obtaining ocular tissue solely for the purpose of diagnosis is not yet common or established practice in the UK.Citation15
IgG dominates the intraocular antibody response against the parasite.Citation16 Intraocular production of anti-T. gondii IgG has been more frequently noted in patients with recurrent than primary ocular toxoplasmosis (isolated retinal lesions not arising from scars). The presence of intraocular anti-T. gondii IgA antibodies during recurrent disease may provide an important additional tool.Citation12,Citation16 The detection of T. gondii DNA in aqueous or vitreous humor is more frequently found in patients with primary ocular toxoplasmosis than in those with recurrent disease.Citation12,Citation14
Risk of fetal transmission
Ocular disease is mainly associated with the chronic phase of infection with T. gondii, but may also occur during the acute phase of systemic infection (lasting several months) when anti-T. gondii IgM is still detectable. During primary maternal toxoplasmosis, fetal infection occurs as a result of maternal parasitemia and subsequent involvement of the placenta. The first trimester is associated with the lowest rate of fetal transmission, but carries the greatest risk of severe congenital disease (ie, there is an inverse relationship).
It is generally accepted that there is no significant risk of transmission to the fetus where infection in the immunocompetent mother was acquired before conception, even if ocular disease reactivates during pregnancy. This is likely because reactivation is often localised within the eye, and any viable organism entering the blood would be attenuated rapidly due to the action of serum complement activated by circulating antitoxoplasma IgG.
However, the possibility of risk of transmission from mother to child associated with infection acquired months or years prior to conception cannot be excluded unequivocally, albeit that this is likely to be a very rare occurrence.Citation17,Citation18 This view is based on a small number of case reports suggesting women with inactive retinal scars due to toxoplasmosis, or who were known to have long-standing antitoxoplasma IgG antibodies, are also at risk of transmitting this disease to the fetus.Citation17,Citation19 This finding could be accounted for by a down-regulation of the T-cell-mediated immune response that is observed during pregnancy.Citation20 Another explanation put forward is that re-infection or new infection with a different strain of the parasite may occur.Citation21 This has not been demonstrated conclusively by laboratory studies as current serologic tests are not subtype-specific, but suggested indirectly by the presence of rising titers of maternal IgG and/or IgM.Citation17 It has also been suggested that maternal infection just preceding conception may lead to transmission, as the parasitemia may remain active even months after initial exposure.Citation17
Treatment considerations
The traditional approach for the treatment of sight-threatening ocular toxoplasmosis is to use multiple anti-parasitic drugs systemically with or without corticosteroids to reduce retinal scarring and limit damage caused by intraocular inflammation.Citation22 Vision, lesion location, lesion size, and vitreous inflammatory reaction have been identified as indications for systemic treatment.Citation23
There is no consensus regarding the best treatment regimen in nonimmunocompromised, nonpregnant patients.Citation23,Citation24 () Furthermore, it has been suggested that treatment may not alter the natural history of the disease, and may even do more harm than good.Citation1
Table 1 Therapeutic regimens of choice for typical cases of ocular toxoplasmosisTable Footnotea,Table Footnoteb
Unsurprisingly, therefore, the treatment of ocular toxoplasmosis during pregnancy creates an even greater challenge, as the therapeutic options are particularly limitedCitation3. In principle, drugs should only be prescribed in pregnancy if the expected benefit to the mother is thought to be greater than the risk to the fetus. Few if any medications are safe beyond all doubt, particularly in the first trimester when the risk of congenital malformation is greatest.
Ophthalmologists may be less willing to treat pregnant patients with recurrent disease due to concerns over treatment toxicity.Citation8 Consideration may be given to shortening the course of therapy, particularly in patients whose disease responds rapidly to treatment, or consider monotherapy.Citation23 The choice of therapy will depend on whether the maternal ocular infection is acquired or reactivated during pregnancy, and whether there is any evidence of congenital infection.
Ophthalmologists should consult with the patient’s obstetrician and an infectious disease specialist before considering systemic treatment in pregnancy for ocular toxoplasmosis. Patients should also be informed of their options including the benefits and theoretical risks of anti-toxoplasma medical therapy during the first trimester of pregnancy.
‘Classic therapy’ for ocular toxoplasmosis comprises a combination of pyrimethamine, sulfadiazine, and prednisolone. However, pyrimethamine should be avoided in pregnancy due to concerns about its potential for teratogenicity, especially in the first trimester.Citation3 Sulphonamides should be avoided in the third trimester, because they compete with bilirubin for serum proteins, causing kernicterus.Citation3 However, in continental Europe, both pyrimethamine and sulphonamides are used to treat ocular toxoplasmosis during pregnancy.Citation20
Consideration should be given to the use of other antimicrobials. Clindamycin, azithromycin and atovaquone have been routinely used for the treatment of nonophthalmic infectious diseases in pregnancy, and shown to be safe and effective.Citation25–Citation27 Clindamycin, which concentrates in ocular tissue and penetrates tissue cyst walls,Citation28 and azithromycinCitation29 may be effective alternative treatments for patients with ocular disease. It has been suggested that a combination of clindamycin and atovaquone, or a combination of clindamycin and azithromycin may be a safe alternative to the treatment of ocular toxoplasmosis in pregnant patients.Citation3
Spiramycin, which is only available on a named patient basis in the UK, is also considered a safe agent and is known to concentrate in the placenta, reducing the risk of transplacental infection in newly acquired infections.Citation30 However, spiramycin is not effective for ocular disease.Citation24
Pars plana vitrectomy may have a role in selected patients in removing antigenic proteins and inflammatory debris. Furthermore, intraocular antibiotics may be a useful alternative for pregnant patients with ocular toxoplasmosis, by reducing the risk of systemic toxicity.Citation31 Martinez and colleagues reported a case of a pregnant woman in the first trimester with sight-threatening reactivated ocular toxoplasmosis successfully managed with a combination of intravitreal clindamycin and dexamethasone and systemic sulfadiazine.Citation31
Summary
In conclusion, there is evidence to suggest that pregnancy is linked to the reactivation of ocular toxoplasmosis and pregnant women at risk should, therefore, be informed about this risk.Citation20
Pregnant women can be reassured that vertical transmission secondary to recurrent ocular disease is likely to be a rare event. It has been suggested that pregnant women at risk are monitored every three months by screening fundoscopy, and their offspring then followed systemically to exclude the presence of congenital infection. The detection of vertical transmission to the fetus is not straightforward, however.Citation20 Regular ultrasound examination may be appropriate to look for evidence of fetal involvement.Citation32
Serum antibody titers are of limited value in the confirmation of suspected recurrent ocular disease, and the diagnosis remains heavily weighted on clinical examination. There may be a role for intraocular fluid sampling in complex cases although this is rarely performed in the UK.
Guidelines are lacking regarding the most appropriate anti-parasitic regimens for the treatment of ocular toxoplasmosis, highlighting the need for larger cohort studies. It is not surprising, therefore, that the dilemma in choosing an appropriate treatment strategy for pregnant patients is compounded. New, effective ways are required to treat ocular toxoplasmosis while minimizing fetal toxicity to multiple drugs. In this regard, a combination of intravitreal and systemic therapy may be useful in treating patients with recurrent ocular toxoplasmosis in pregnancy with sight-threatening lesions.Citation31
In the case presented here, we chose, following consultation with the patient, not to use standard treatment despite the presence of a macular lesion. A good visual outcome was achieved. We hope that this article serves to highlight to ophthalmologists alternative management options when dealing with a more challenging case.
Disclosures
The authors report no conflicts of interest in this work.
References
- StanfordMRSeeSEJonesLVGilbertREAntibiotics for Toxoplasmic retinochoroiditis. An evidence-based systematic reviewAm J Ophthalmol20031105926931
- HollandGNOcular toxoplasmosis: A global reassessment. Part I: Epidemiology and Course of disease. LX Edward Jackson Memorial LectureAm J Ophthalmol2003136697398814644206
- KumpLIAndroudiSNFosterCSOcular toxoplasmosis in pregnancyClin Exp Ophthalmol200533455460
- Bosch-DriessenLEBerendschotTTOngkosuwitoJVRothovaAOcular toxoplasmosis: clinical features and prognosis of 154 patientsOphthalmology200210986987811986090
- BraakenburgAMDRothovaAClinical features of ocular toxoplasmosis during pregnancyRetina20092962763019262434
- CouvreurJDesmontsGCongenital and maternal toxoplasmosis: A review of 300 congenital casesDev Med Child Neurol1962451953014023494
- DunnDWallonMPeyronFPetersenEPeckhamCGilbertRMother-to-child transmission of toxoplasmosis: risk estimates for clinical counsellingLancet19993531829183310359407
- LumFJonesJLHollandGNLiesegangTJSurvey of ophthalmologists about ocular toxoplasmosisAm J Ophthalmol2005140472472616226526
- de JongPTOcular toxoplasmosis: common and rare symptoms and signsInt Ophthalmol1989133913972697705
- ThulliezPDaffosFForestierFDiagnosis of toxoplasma infection in the pregnant woman and the unborn child: current problemsScand J Infect Dis199284Suppl1822
- HollimanREStevensPJDuffyKTJohnsonJDSerological investigation of ocular toxoplasmosisBr J Ophthalmol1991753533552043579
- OngkosuwitoJVBosch-DriessenEHKijlstraARothovaASerologic evaluation of patients with primary and recurrent ocular toxoplasmosis for evidence of recent infectionAm J Ophthalmol199912840741210577580
- RothovaAvan KnapenFBaarsmaGSKruitPJLoewer-SiegerDHKijlstraASerology in ocular toxoplasmosisBr J Ophthalmol1986706156223741830
- de BoerJHVerhagenCBruinenbergMEvaluation of serological and PCR analysis of intraocular fluids in the diagnosis of infectious uveitisAm J Ophthalmol19961216506588644808
- KijlstraALuyerdijkLBaarsmaGSAqueous humor analysis as a diagnostic tool in toxoplasma uveitisInt Ophthalmol1989133833862697703
- RondayMJHOngkosuwitoJVRothovaAKijlstraAIntraocular anti-toxoplasma gondii IgA antibody production in patients with ocular toxoplasmosisAm J Ophthalmol199912729430010088739
- DollfusHDureauPHennequinCCongenital toxoplasma chorioretinitis transmitted by preconceptionally immune womenBr J Ophthalmol199882144414459930281
- HennequinCCongenital toxoplasmosis acquired from an immune womanPediatr Infect Dis J19971675769002108
- SilveiraCFerreiraRMuccioliCNussenblattRBelfortRToxoplasmosis transmitted to a newborn from the mother infected 20 years earlierAm J Opthalmol20031362370371
- GarwegJGScherrerJWallonMKodjikianLPeyronFReactivation of ocular toxoplasmosis during pregnancyBJOG200511224124215663591
- HoweDKSibleyLDToxoplasma gondii comprises three clonal lineages: correlation of a parasite genotype with human diseaseJ Infect Dis1995172156115667594717
- RothovaABuitenhuisHJMeenkenCTherapy of ocular toxoplasmosisInt Ophthalmol1989134154192697708
- HollandGNLewisKGAn update on current practices in the management of ocular toxoplasmosisAm J Ophthalmol200213410211412095816
- HollandGNOcular toxoplasmosis: A global reassessment. Part II: Disease manifestations and management. LX Edward Jackson Memorial LectureAm J Ophthalmol2004137111714700638
- UgwumaduAReidFHayPNatural history of bacterial vaginosis and intermediate flora in pregnancy and effect of oral clindamycinObstet Gynecol200410411411915229009
- RamseyPSVaulesMBVasdevGMMaternal and transplacental pharmacokinetics of azithromycinAm J Obstet Gynecol200318871471812634646
- McGreadyRStepniwskaKEdsteinMDThe pharmacokinetics of atovaquone and proguanil in pregnant women with acute falciparum malariaEur J Clin Pharmacol20035954555212955371
- TabbaraKFO’ConnorGROcular tissue absorption of clindamycin phosphateArch Ophthalmol197593118011851191404
- RothovaABosch-DriessenLEHvan LoonNHTreffersWFAzithromycin for ocular toxoplasmosisBr J Ophthalmol199882130613089924338
- Stray-PedersenBTreatment of toxoplasmosis in the pregnant mother and newborn childScand J Infect Dis Suppl19928423311290070
- MartinezCEZhangDConwayMDPeymanGASuccessful management of ocular toxoplasmosis during pregnancy using combined intraocular clindamycin and dexamethasone with systemic sulfadiazineInt Ophthalmol19981999228588
- Gay-AndrieuFMartyPPialatJSourniesGDrier de LaforteTPeyronFFetal toxoplasmosis and negative amniocentesis: necessity of an ultrasound follow-upPrenat Diagn200323755856012868082