Abstract
Purpose
To follow the changes in the electroretinograms (ERGs) in a patient with primary intraocular lymphoma (PIOL) who had a complete remission after chemotherapy.
Methods
ERGs were recorded in a 41-year-old woman with PIOL during and after complete remission with chemotherapy. The patient was diagnosed with PIOL from both the ocular signs and the medical history of cranial lymphoma.
Results
The ERGs were depressed in the subject. The amplitudes of the bright white flash b-waves were smaller than the a-waves, resulting in a “negative type” ERG. Six weeks after the beginning of chemotherapy, the ocular changes had resolved, and the ERGs, although not of the “negative type”, still showed signs that the amplitude had not returned to normal levels.
Conclusion
The negative type ERGs indicated that the inner retina had been damaged to a greater extent than the outer retina. In the convalescent stage, when the ocular manifestations were resolved, the ERGs were still not fully recovered. Although only one case was studied, we suggest that ERGs can be used to evaluate and follow patients with a PIOL.
Introduction
A primary intraocular lymphoma (PIOL) is a subtype of primary non-Hodgkin’s lymphomas of the central nervous system in which the retina, vitreous, and/or optic nerve head may be involved.Citation1–Citation3 Patients with a PIOL typically present with a form of uveitis and vitritis that is unresponsive to corticosteroid therapy, thus the so-called uveitis masquerade syndrome. This can occur together with, or independently of, a primary cerebral nervous system lymphoma. The disease has a poor prognosis, and patients normally die as a result the growth of the cerebral lymphoma with a mean survival of 20 months from the diagnosis of the ocular disorder.Citation4
As best we know, electroretinography (ERG) has not been used to follow the changes in retinal function during the course of PIOL. We present the changes in the ERGs during and after a complete remission of PIOL with chemotherapy.
Case report
The patient, a 41-year-old woman, had been diagnosed with a primary intracranial malignant lymphoma (non-Hodgkins, diffuse medium-sized B cell lymphoma) for three years. She presented with a 3-week history of blurred vision and photophobia, primarily in her right eye. Her best-corrected visual acuities were 20/60 OD and 20/20 OS. The intraocular pressure was normal in both eyes. Slit-lamp examination showed mild vitritis in the right eye, and ophthalmoscopy showed no abnormalities.
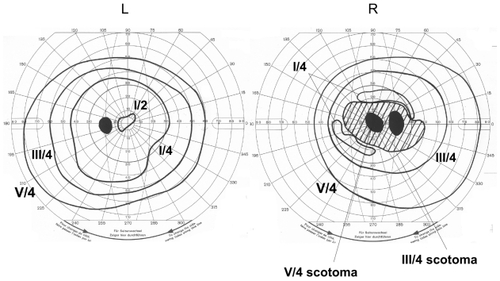
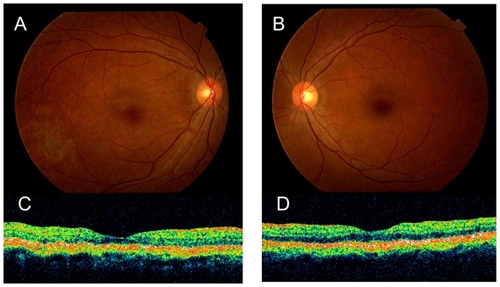
After 3 weeks of observation the right fundus had developed whitish exudates, massive subretinal infiltration from a macular lesion, and slight swelling of the optic disc. Cells were detected in the anterior chamber, but the fundus of the left eye was normal (). The Goldmann visual field of the right eye had a dense central relative scotoma, but was almost normal in the left eye ().
Figure 1 Fundus photograph of the right A) and the left eyes B). The right fundus shows whitish exudates, massive subretinal infiltration under the macular lesion, and slight disc swelling. The left fundus is normal. Fluorescein angiography of the right C) and left eyes D) Slight leakage of fluorescein can be seen on the right optic disc. The left eye is normal. Optical coherence tomography of the macular area of the right E) and left eye F). Massive subretinal infiltration is present in the right eye. The left eye is normal.
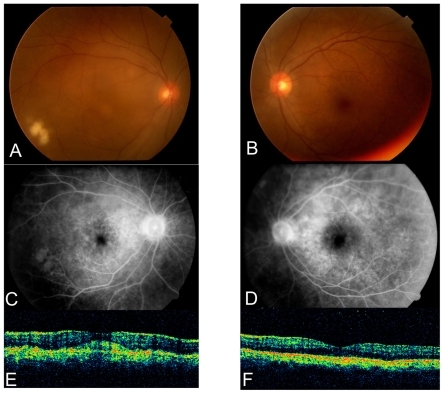
Figure 2 Goldmann perimetry showing a central scotoma in the right eye. The visual field of left eye is normal.
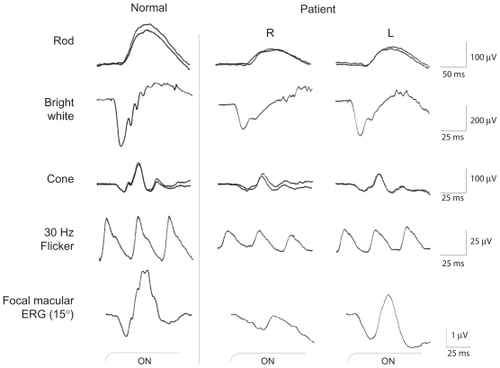
Full-field ERGs were recorded according to International Society for Clinical Electrophysiology of Vision (ISCEV) standards.Citation5 The scotopic, bright white, cone, and 30 Hz flicker ERGs 3 weeks after the initial visit are shown in . The amplitudes of the different ERG components were reduced in both eyes, but to a greater extent in the right eye. The amplitude of the bright white flash b-waves was distinctly reduced, and was smaller than the a-waves, resulting in the “negative type” ERG in both eyes. This indicated that the functional depression was greater in the inner retina than the outer retina.Citation6
Figure 3 Full-field ERGs (rod, bright white, cone and 30 Hz flicker) recorded according to International Society for Clinical Electrophysiology of Vision (ISCEV) standards. Compared to the normal ERGs, the amplitudes of all components were reduced especially in the right eye. Focal macular ERGs elicited by a 15 degree stimulus spot were recorded from both eyes (bottom row). A marked reduction of amplitude can be seen in the right eye.
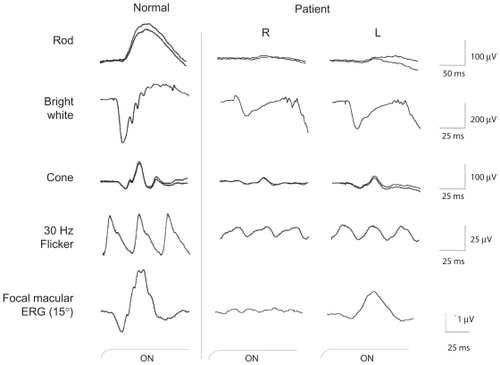
Focal macular ERGs were recorded to assess macular function as described in Miyake et al.Citation7 The ERG from the right eye was almost nonrecordable, and that of left eye was about one-half the normal amplitude (; Focal macular ERGs).
Because of the rapid decrease in the visual acuity of the right eye to 20/600, and the increasing retinal infiltration and exudations since the previous examination, diagnostic vitrectomy was performed (). Cytological examination of the vitreal specimen did not show any abnormal lymphocytes or monocytes, in addition to which flow cytometry did not show monoclonality. The cytokine analysis was negative without a specific increase in the IL10/IL6 ratio. Although the results of the cytological examinations were negative, a primary intraocular lymphoma was strongly suspected.
Figure 4 Fundus photograph after vitrectomy of the right eye. The retinal infiltrates and exudates have progressed in the right eye within one week since the previous examination. The left eye fundus had no abnormality.
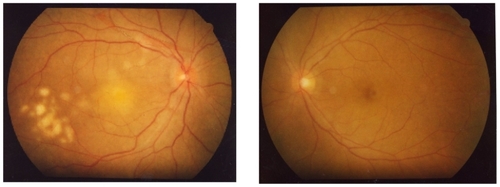
Eight weeks after the first visit, chemotherapy with cyclophosphamide, cytosine arabinoside, etoposide, and dexamethasone was started. Four days after the treatment, the visual symptoms and ophthalmoscopic appearance of the fundus improved. Six weeks after beginning chemotherapy, her best-corrected visual acuity improved to 20/20 in both eyes. The ocular lesions were completely resolved, leaving atrophic pigmentary changes (). A relative central scotoma still remained in the right eye, but the visual field sensitivity had improved. The cells in the anterior chamber of the left eye had also disappeared.
Figure 5 Fundus photography of the right A) and the left eye B) one month after chemotherapy. The ocular lesions have completely resolved leaving atrophic pigmentary changes. Optical coherence tomography of the macular area of the right C) and the left eye D) shows that the massive subretinal infiltration of the right eye has disappeared.
Although the rod and cone components of the full-field ERGs had improved after chemotherapy, the amplitudes had still not reached normal limits (). The recovery of the b-wave was greater than that of the a-wave in the bright flash ERG, and so the waveform was not of the “negative type” at this point.
Figure 6 Full field ERGs (rod, bright white, cone and 30 Hz flicker) and focal macular ERG recorded one month after chemotherapy. The ERG amplitudes of all components have increased after therapy but still remained smaller than normal ERGS in both eyes.
Three years after the therapy, the patient had no evidence of systemic disease or recurrence of the PIOL. The ERGs were greatly improved but the amplitudes had still not reached the normal range.
Discussion
We have followed a patient with a PIOL by electroretinography, who went into complete remission after chemotherapy. We found that the bright flash ERGs were the negative-type ERGs before chemotherapy. These ERG findings suggest that the inner retina was damaged more than the outer retina. As a differential diagnosis, we suspected endophthalmitis and uveitis, especially Beçhet’s disease. However, from the history of intracranial malignant lymphoma, and the clinical signs, we diagnosed the patient as having a PIOL, even though the vitreous biopsy did not detect any malignant cells or a change in the IL-10/IL-6 ratio. It is known that the interpretation of vitreous specimens is sometimes difficult, and more than 40% of vitrectomy specimens may be nondiagnostic. Citation8,Citation3
After chemotherapy, the b-wave recovered more quickly than the a-wave. These results indicate that the inner retinal damage was transient, and may have resulted from secondary inflammation due to the presence of tumor cells. In the convalescent stage, when the ocular manifestations were resolved, both full-field and focal macular ERGs were still not fully recovered.
Earlier histopathological studies of PIOL’s have mentioned an infiltration of malignant lymphoma cells into the subretinal space, which would be detected as whitish exudates, and could also lead to damage to the retina.Citation9,Citation10 In our case, a marked prolongation of the focal macular ERG in the right eye may have been as a result of photoreceptor damage caused by just such subretinal infiltration.
Conclusion
In conclusion, we recorded ERGs from a patient whose ocular findings and history indicated that she had PIOL. The full-field ERGs were reduced in the right eye, showing a the negative-type ERG. After chemotherapy, there was a recovery in both the ocular signs and the ERGs. Although our conclusions are based on only one case, we recommend that ERGs be used to diagnose and follow patients with a PIOL.
Acknowledgments
/disclosures
The authors report no conflicts of interest in this work, but acknowledge support from the Ministry of Education, Science, Sports and Culture, Japan – Grant number 18591913 (MK).
References
- TsaiTO’BrienJMMasquerade syndromes: malignancies mimicking inflammation in the eyeInt Ophthalmol Clin200242111513112189607
- ChanCCBuggageRRNussenblattRBIntraocular lymphomaCurr Opin Ophthalmol200213641141812441846
- CouplandSEHeimannHBechrakisNEPrimary intraocular lymphoma: a review of the clinical, histopathological and molecular biological featuresGraefes Arch Clin Exp Ophthalmol20042421190191315565454
- FreemanLNSchachatAPKnoxDLMichelsRGGreenWRClinical features, laboratory investigations, and survival in ocular reticulum cell sarcomaOphthalmology19879412163116393323986
- MarmorMFHolderGESeeligerMWYamamotoSInternational Society for Clinical Electrophysiology of VisionStandard for clinical electroretinography (2004 update)Doc Ophthalmol2004108210711415455793
- MiyakeYYagasakiKHoriguchiMKawaseYKandaTCongenital stationary night blindness with negative electroretinogram. A new classificationArch Ophthalmol19861047101310203488053
- MiyakeYShiroyamaNHoriguchiMOtaIAsymmetry of focal ERG in human macular regionInvest Ophthalmol Vis Sci1989308174317492759790
- CouplandSEBechrakisNEAnastassiouGEvaluation of vitrectomy specimens and chorioretinal biopsies in the diagnosis of primary intraocular lymphoma in patients with Masquerade syndromeGraefes Arch Clin Exp Ophthalmol20032411086087014605902
- ChanCCWallaceDJIntraocular lymphoma: update on diagnosis and managementCancer Control200411528529515377987
- GillMKJampolLMVariations in the presentation of primary intraocular lymphoma: case reports and a reviewSurv Ophthalmol200145646347111425352