Abstract
Interest in marine natural products has allowed the discovery of new drugs and trabectedin (ET-743, Yondelis), derived from the marine tunicate Ecteinascidia turbinata, was approved for clinical use in 2007. It binds to the DNA minor groove leading to interferences with the intracellular transcription pathways and DNA-repair proteins. In vitro antitumor activity was demonstrated against various cancer cell lines and soft tissue sarcoma cell lines. In phase I studies tumor responses were observed also in osteosarcomas and different soft tissue sarcoma subtypes. The most common toxicities were myelosuppression and transient elevation of liver function tests, which could be reduced by dexamethasone premedication. The efficacy of trabectedin was established in three phase II studies where it was administered at 1.5 mg/m2 as a 24 h intravenous infusion repeated every three weeks, in previously treated patients. The objective response rate was 3.7%–8.3% and the tumor control rate (which included complete response, partial response and stable disease) was obtained in half of patients for a median overall survival reaching 12 months. In nonpretreated patients the overall response rate was 17%. Twenty-four percent of patients were without progression at six months. The median overall survival was almost 16 months with 72% surviving at one year. Predictive factors of response are being explored to identify patients who are most likely to respond to trabectedin. Combination with other agents are currently studied with promising results. In summary trabectedin is an active new chemotherapeutic agents that has demonstrated its role in the armamentarium of treatments for patients with sarcomas.
Soft tissue sarcomas
Soft-tissue sarcomas are a highly heterogeneous group of tumors with a low incidence. They account for 1% of all adult and 15% of pediatric malignancies.Citation1,Citation2 At least 50 different subtypes are distinguished, each with its specific biology and clinical outcome. The majority of these tumors are presumably derived from mesoderm and categorized by the normal tissue they resemble. As they are uncommon, however, they are subsumed under the collective term “soft-tissue sarcoma” and therapeutically approached in similar ways.
Despite adequate local treatment, up to one half of patients develop distant metastases. Most of these patients with advanced (ie, not resectable) or metastatic disease die from the disease after a median survival time from diagnosis ranging between eight to 12 months.Citation3 The most common approach in all histological subtypes is to use doxorubicin and ifosfamide.Citation4 Doxorubicin remains the reference in first line therapy with response rate of 20%–30% in large randomized trials.Citation4–Citation6 As a monotherapy, ifosfamide yielded response rate similar to doxorubicin.Citation5–Citation8 It is widely used as second-line therapy after anthracycline failure with a response rate in the 10%–20% range.Citation8,Citation9
Combining these agents might be more effective but has not been shown to improve survival in a significant way compared to their use as single agents.Citation6 Following suggestions that these agents may have a dose-response relationship,Citation9–Citation11 various phase-I and -II trials were performed in which they were administered at high doses, yielding response rates of 40%–66%Citation12–Citation15,Citation16 leading to median overall survival of up to 24 months in some studies. There are also suggestions that applying regimens with high response rates may render an initially inoperable tumor operable, thereby improving the outcome.Citation17 But in two recent randomized trials,Citation18–Citation20 neither the response rate nor the overall survival could be improved by the intensification of chemotherapy, even if the progression-free survival was increased in one study.Citation18
In recent years, progress has been made in understanding the clinical and biological complexity of sarcomas,Citation21,Citation22 such that oncologists have increasingly been able to define customized therapies. Paclitaxel has been found to be active mainly in patients with angiosarcomas.Citation23 Docetaxel combined with gemcitabine has been shown to induce a 53% response rate in leiomyosarcomas of gynecological origin.Citation24 Topoisomerase inhibitors are active for rhabdomyosarcomas. Citation25 And the identification of genetic abnormalities with the presence of fusion genes that are strongly associated with specific sarcoma subtypes has contributed towards understanding the biology of these tumors, and has facilitated their diagnosis. It has also opened new avenues for therapies targeted against the transcription pathways induced by these fusion proteins.Citation26,Citation27
In the past years, the interest in marine natural products has provided new possibilities of drug discovery.Citation28 The first clinical agent derived from nucleosides obtained from marine sponge was cytosine arabinoside. Other marine compounds are in development such as aplidine obtained from the Mediterranean tunicate A. albicans or bryostatin from the bryozoan Bugula neritina. But trabectedin (ET-743, Ecteinascidin-743) is the first marine anticancer drug approved for clinical use in the European Union since 2007.
Trabectedin
Structure, mechanism of action, preclinical antitumor activity and phase I trials
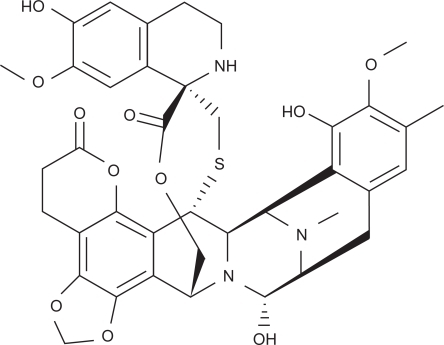
Trabectedin (ET-743, Ecteinascidin, Yondelis) is a DNA-binding agent derived from the marine tunicate Ecteinascidia turbinata, now obtained by a semi-synthetic process starting with the antibiotic cynosafracin B.Citation29,Citation30 The molecule is comprised of three fused tetrahydroisoquinoline rings () of which two are covalently and reversibly bound to the DNA minor groove by a guanine specific alkylation at the N2 position. This induces a DNA bending towards the major groove.Citation31,Citation32 The third ring, being unbound, could interact with nuclear proteins. The transcriptional activation of inducible genes is inhibited, depending on the presence of the DNA repair systems, particularly the transcription coupled nucleotide excision repair system.Citation33 The sensitivity to trabectedin is related to the presence of active repair mechanisms.Citation34 A cell cycle arrest at G2/M and apoptosis is induced through a p53-independent process.Citation35
Figure 1 Structure of trabectedin.
In vitro, trabectedin has a broad spectrum of activity in human primary tumor cells.Citation36 The drug was very active against several different sarcoma cell linesCitation37 and the results of activity in human tumor xenografts demonstrated activity in melanoma, non-small cell lung cancer and ovarian cancer.Citation38,Citation39
Pharmacokinetics and phase I studies
After infusion, trabectedin is rapidly cleared from plasma, undergoing an extensive hepatic metabolism mainly through the cytochrome P450 3A4.Citation40 Trabectedin has a high apparent volume of distribution and a half-life of approximately 90 hours.Citation41 It is mainly excreted in the feces but less than 1% is excreted unchanged in the urine or feces.Citation42
In phase I studies (), different schedules were investigated in patients with solid tumors. This schedules range from an intravenous infusion over 1, 3, 24, or 72 hours every three weeks to a weekly infusion for three out of a four-week cycle.Citation43–Citation47 The dose-limiting toxicities (DLT) were mainly hematological (neutropenia, thrombocytopenia) and fatigue. Grade 3–4 hepatic toxicities were also DLT in some but not all trials.Citation45,Citation46 DLT were transient and not cumulative. Nausea and vomiting were managed with 5HT3-antagonists. Fatigue or asthenia grade 3–4 was also frequently described (8% to 50%). Tumors responses were observed in soft tissue sarcoma, osteosarcoma, melanoma, and breast cancer.
Table 1 Dose-limiting toxicity (DLT) and maximum tolerated dose (MTD) in Phase I studies
Two schedules were recommended for further phase II studies: 1.5 mg/m2 as a 24-hour continuous infusion given every three weeks and 0.58 mg/m2 as a three-hour infusion given weekly for three out of four weeks.
Phase II studies of trabectedin in pretreated sarcomas
The efficacy of trabectedin was studied in four phase-II studies in pretreated soft tissue sarcoma from US and EuropeCitation48–Citation50 of which one was a randomized phase II study comparing two different schedulesCitation51 ().
Table 2 Efficacy and survival data of trabectedin in phase II trials
The first trial, published in 2004 by Yovine and colleagues,Citation48 investigated trabectedin 1.5 mg/m2 administered as a 24-hour continuous infusion. Fifty-four patients were enrolled and analyzed in two predefined groups. The first group of 26 patients was pretreated with only one or two single agents or one combination regimen and the second group of 28 patients were heavily pretreated with at least three chemotherapeutic agents or two combinations. The predominant histology was leiomyosarcoma (n = 22, of uterine origin (n = 8)), and liposarcoma (n = 6). Two partial responses (3.7% [95% confidence interval (CI): 0.5%–12.8%]) were reported and both had uterine leiomyosarcoma, four (7.4%) patients had a minor response, and nine (17%) patients had stable disease. Among the six responding patients, five received prior chemotherapy with ifosfamide and doxorubicin. The median progressionfree survival was 1.9 months after a median follow-up of 26 months. At three and six months, 38.8% and 24.1% of patients were progression-free, respectively. No difference was noted in progression-free survival between the two groups. But the less pre-treated patients had a longer median overall survival of 13.7 months versus 7.9 months. Overall, the median survival was 12.8 months with 30% of patients alive at two years.
Garcia-Carbonero and colleagues reported the results of the phase II study with trabectedin 1.5 mg/m2 administered as a 24-hour continuous infusion, conducted in 36 patients pretreated with up to two prior chemotherapy regimens.Citation50 Some histological subtypes were excluded as gastrointestinal stromal tumors (GIST), mesothelioma, osteosarcoma, carcinosarcoma, Kaposi’s sarcoma, or rhabdomyosarcoma. And the main histologies were leiomyosarcomas (n = 13), liposarcomas (n = 10), and synovial sarcomas (n = 6). One complete response (CR) was obtained in a patient with liposarcoma, and two partial responses (PR) in a patient with leiomyosarcoma and in a patient with liposarcoma, for an overall response rate of 8% (95% CI: 2%–23%). Two other patients had a minor response. The median time to progression was 1.7 months and the median overall survival was 12.1 months with an overall survival rate at one year of 53.1%.
The third study published by Le Cesne and colleaguesCitation49 was conducted in eight European centers by the European Organisation for Research and Treatment of Cancer (EORTC) and administered trabectedin at 1.5 mg/m2 as a 24-hour continuous infusion. One hundred and four patients were accrued with progressive soft tissue sarcomas excluding GIST. Most patients had leiomyosarcomas (n = 43), synovial sarcomas (n = 18), or liposarcomas (n = 10). There were eight partial responses (in leiomyosarcomas [n = 5], synovial sarcoma [n = 1], liposarcoma [n = 1], and malignant fibrous histiocytoma [n = 1]) and forty-five (40.5%) stable disease. Disease stabilization longer than six months was measured in 26% of patients. Of note the tumor control rate (defined as non progressing patients) reached 56% in leiomyosarcomas, 61% in synovial sarcomas, and 40% in liposarcomas. After a median estimated follow-up of 34 months, the median time to progression was 3.4 months. The progression-free rates at 3, 6, and 12 months were respectively 52%, 29%, and 17%. GIST histology has been evaluated separately. Among 28 patients none responded and the best effect was disease stabilization in nine patients. The median time to progression was less than two months allowing to conclude that trabectedin was ineffective in GIST when given alone with this schedule.Citation52
The results of these three phase IICitation48–Citation50 studies involving 183 patients were pooled and analyzed by Le Cesne.Citation53 Leiomyosarcoma remained the main histological subtype representing 41% of patients followed by liposarcoma in 14% and synovial sarcoma in 11%. Most patients (95%) were pretreated with anthacyclines or ifosfamide and 113 patients were resistant to anthracyclines, 81 resistant to ifosfamide, and 63 to both agents. The overall response rate was 7.7%. The clinical benefit, defined as the combination of the rate of objective response and of minor response and of stable disease, was 51.5%. The median overall survival was 10.3 months with an overall survival rate at one year of 47.5% and a progression-free survival rate at six months of 19.8%. The clinical benefit was similar in patients with bulky disease, with multiple pretreatments, with short previous progression-free survival or with early resistance to standard chemotherapy, suggesting the lack of cross resistance and a specific mechanism of action.Citation54
A phase II randomized trial was conducted in patients with liposarcoma or leiomyosarcoma after failure of anthracyclines and ifosfamide.Citation51 Two hundred seventy patients received either trabectedin at 0.58 mg/m2 as a 3 h weekly infusion, three out of four weeks or at 1.5 mg/m2 as a 24 h continuous infusion every three weeks. A significantly longer time to progression was achieved for the three weekly regimen reaching 3.7 months and 2.3 months for the weekly regimen (p = 0.0302, hazard ratio [HR]: 0.734). The median overall survival was 13.8 months for the three weekly and 11.8 for the weekly regimen. The clinical benefit favored the three weekly regimen even if not statistically significant (58% versus 44%). Neutropenia grade 3–4 was described in 47% and 13% on the three weekly and the weekly arm, respectively, but it did not translate to a different rate of febrile neutropenia (0.8%). Similarly grade 3–4 transaminitis (ALAT) was more frequent in the three weekly arm (48% versus 9%), but without clinical consequences.
The results of the compassionate use programs in an unselected population, even though most of them included leiomyosarcomas or liposarcomas, were very similar in term of efficacy and toxicity.Citation55–Citation59 And in a historical comparison, progression-free survival of trabectedin was better than the other active chemotherapeutic agents.Citation60
First line trabectedin in sarcomas
A phase II trial from Garcia-Carbonero and colleagues evaluated 36 patients with advanced or metastatic soft tissue sarcomas.Citation61 The main histological subtypes were leiomyosarcomas (n = 15) and liposarcomas (n = 9). One complete response and five partial responses were observed for an overall response rate of 17.1% (95% CI: 6.6%–33.6%). Responses occurred in three patients with liposarcoma, and one patient each with leiomyosarcoma, synovial sarcoma, and fibrosarcoma. One patient with a uterine leiomyosarcoma had a minor response. The median progression-free survival was 1.6 months and the progression-free rate at 6 months was 24.4%. Median overall survival was 15.8 months and overall survival at one year was 72%.
Tolerability
The toxicity profile encountered in the phase II trials was similar to the results observed in the phase I studies evaluating the 24-hour continuous infusion of trabectedin at the recommended dose. Myelosuppression and hepatic toxicity were the most frequently observed adverse events (). Despite neutropenia grade 3–4 in 33%–61% of patients, there was a low incidence of febrile neutropenia (6%–7%), quite different from other agents as doxorubicin (up to 19%)Citation18,Citation62 or ifosfamide regimens (up to 39%).Citation5,Citation8,Citation9 Thrombocytopenia and anemia grade 3–4 was seen in 9%–22% of pretreated patients, but not in first line therapy.
Table 3 Incidence of grade 3/4 toxicities in phase II trials
Liver toxicity was frequent, but not cumulative and rapidly reversible. Transaminase elevation at more than five times the normal range was described in 20% to 57% of pretreated and 30% of the nonpretreated patients. This toxicity could be improved by dexamethasone premedication. In xenografts models, the hepatotoxicity induced by trabectedin was markedly reduced or avoided after administration of metabolism modulators such as dexamethasone or beta-naphtoflavone 24 h before trabectedin.Citation63 The authors reported no difference in antitumor efficacy and hypothesized a decreased hepatic exposure to trabectedin, perhaps by regulation of hepatic metabolism.Citation64 In the clinic dexamethasone premedication was retrospectively analyzed by Grosso and colleagues.Citation55 Twenty-three patients treated with trabectedin 1.0 to 1.65 mg/m2 as a three-hour or 24-hour continuous infusion every 21 days did not receive premedication whereas 31 patients received dexamethasone 4 mg per os bid 24 hours before therapy. The incidence of grade 3–4 transaminitis was reduced from 70% to 3% of patients by the dexamethasone premedication. The incidence of neutropenia and thrombocytopenia was also less important at 10% and 0% instead of 39% and 35%, respectively. The antitumor activity was similar between the two groups and comparable to the ones reported in other phase II trials. The overall response rate was 9% and the median progression-free survival was 2.6 months.
The analysis of four treatment-related deaths in the European phase II studyCitation49 revealed a statistical correlation between these severe toxicities and liver dysfunction. The influence of patient characteristics and pathophysiological variables was analyzed in 69 patients treated in phase II studies.Citation65 The incidence of severe toxicity was significantly (p = 0.02) greater for patients with any baseline liver function test exceeding the upper limit of the normal range. Thus the administration of the full dose of trabectedin at 1.5 mg/m2 requires normal alkaline phosphatase and transaminase levels, checked before each cycle, and the dose should be reduced to 1.2 mg/m2 in case of abnormal bilirubin level, and more than 2.5 increase of transaminase or alkalin phosphatase above the normal range.
Other frequent toxicities included nausea, vomiting and fatigue that could be grade 3–4 in up to 9% of patients. Elevation of creatine phosphokinase (CK) has been reported in 26% of patients and a few cases of severe and fatal rhabdomyolysis have been observed in the phase I–II studies.Citation44,Citation48,Citation66 By an unknown mechanism, trabectedin induced necrosis of skeletal muscle resulting in subsequent release of intracellular contents leading to electrolyte imbalance, renal failure and death. Caution should be taken when used with other medications known to cause muscle injury as statins. CK is the most sensitive indicator of muscle injury and should be ≤2.5× upper limit of normal before each treatment and closely monitored during therapy.
Perspective
Predictive factors of response
The mechanism of action of trabectedin is not well understood, but it acts partially through interferences with the transcription pathways.Citation67–Citation69 The sensitivity of myxoid liposarcoma carrying a specific chromosomal translocation t(12; 16)(q13; p11) or t(12; 22)(q13; q12) that produce a DDIT3-FUS (DDIT3-EWSR1) fusion protein has been clinically recognized.Citation62 Under treatment, the tissue density changes were consistent with a decrease in cellularity before tumor shrinkage, suggesting that it has modulated adipocyte differentiation. Recent in vivo data confirmed that trabectedin was able to induce a cascade of events leading to the activation of adipogenesis differentiation in cell lines presenting similar fusion genes.Citation70 It opens interesting perspectives for the treatment of other translocation-related sarcomas and for the combination with other differentiating agents.
Trabectedin promotes DNA damage through its binding to N2 guanine in the minor groove causing a structural bending of DNA towards the major groove, and an unusual DNA helix distortion. This lesion is a substrate for the nucleotide excision repair (NER) pathway. In experimental models deficient cells in NER are insensitive to trabectedin.Citation71 Thus the mRNA levels expression of ERCC1 (NER machinery), XPD (NER machinery), BRCA1 and BRCA2 were analyzed in 92 sarcoma patients by Schoeffski and colleagues.Citation72 The six-month progression-free survival and median overall survival were improved for patients with high expression levels of ERCC1 (32% versus 15% and 12 months versus seven months, respectively). An increased six-month progression-free rate (33% versus 11%) and a longer median overall survival (15 versus five months) were significantly associated with low expression of BRCA1. No significant effect of XPD and BRCA2 was found on progression-free survival and overall survival. Some patients were highly sensitive to treatment when a high ERCC1 and a low BRCA1 expression were measured. They had a six-month progression-free survival of 50% and a median overall survival of 20.4 months. If the treatment of sarcomas by trabectedin should be based on a specific repair mechanism profile remains to be shown in a prospective study.
Combinations
Combination treatments with doxorubicin,Citation73 irinotecan,Citation74 and paclitaxelCitation75 were evaluated in preclinical studies showing synergistic effects against sarcomas. Trabectedin was combined with doxorubicin,Citation76,Citation77 pegylated liposomal doxorubicin,Citation77 paclitaxel,Citation78 and capecitabineCitation79 in phase I studies involving patients with solid tumors. The DLT were essentially myelosuppression and hepatotoxicity.
In sarcomas a phase I study combining doxorubicin and trabectedin reported that the maximum tolerated dose was 60 mg/m2 and 1.1 mg/m2 respectively. Preliminary pharmacokinetics of both agents were not significantly modified by the combination. Because of severe neutropenia at the first dose level, granulocyte colony-stimulating factor had to be added subsequently. The dose limiting toxicities were neutropenia and thrombopenia. Dose reduction was required in 51% of patients for trabectedin and 27% for doxorubicin. Among the 41 treated patients, five achieved a partial remission and 34 had a disease stabilization that lasted more than six months in 15 patients.Citation77
Conclusion
The marine-derived DNA-binding protein trabectedin induces DNA damage and transcriptional interference, which are dependent on the presence of DNA-repair systems. In phase I studies, the optimal dose and schedule of administration of trabectedin was 1.5 mg/m2 as a 24 h intravenous continuous infusion every three weeks. In pretreated patients, the three phase II studies involving 183 patients showed response rate up to 10% with disease control achieved in approximately 50% and a median overall survival of one year. Significant activity was also found in first line therapy with a response rate of 17% and 72% of patients surviving at one year. The treatment is generally well tolerated at the recommended dose. The most frequent severe toxicities were neutropenia, thrombocytopenia, and transient increase of hepatic tests. These adverse events were not cumulative and were rapidly reversible. Dexamethasone premedication reduced the hepatotoxicity and the myelosuppression. A better understanding of the mechanisms of action of trabectedin and its effect on transcription pathways make it a good candidate for combination with other chemotherapeutic agents or targeted therapy.
Disclosure
The authors report no conflicts of interest in this work.
References
- ClarkMAFisherCJudsonIThomasJMSoft-tissue sarcomas in adultsN Engl J Med200535370171116107623
- CasaliPGJostLSleijferSVerweijJBlayJYSoft tissue sarcomas: ESMO clinical recommendations for diagnosis, treatment and follow-upAnn Oncol200819Suppl 2ii89ii9318456783
- Adjuvant chemotherapy for localised resectable soft-tissue sarcoma of adults: meta-analysis of individual data. Sarcoma Meta-analysis CollaborationLancet1997350164716549400508
- EdmonsonJHRyanLMBlumRHRandomized comparison of doxorubicin alone versus ifosfamide plus doxorubicin or mitomycin, doxorubicin, and cisplatin against advanced soft tissue sarcomasJ Clin Oncol199311126912758315424
- LoriganPVerweijJPapaiZPhase III trial of two investigational schedules of ifosfamide compared with standard-dose doxorubicin in advanced or metastatic soft tissue sarcoma: a European Organisation for Research and Treatment of Cancer Soft Tissue and Bone Sarcoma Group StudyJ Clin Oncol2007253144315017634494
- SantoroATurszTMouridsenHDoxorubicin versus CYVADIC versus doxorubicin plus ifosfamide in first-line treatment of advanced soft tissue sarcomas: a randomized study of the European Organization for Research and Treatment of Cancer Soft Tissue and Bone Sarcoma GroupJ Clin Oncol199513153715457602342
- SerroneLZeuliMPapaldoPNardoniCPacettiUCognettiFIfosfamide and epirubicin combination in untreated sarcomas: two treatment schedulesOnkologie20012446546811694773
- NielsenOSJudsonIvan HoeselQEffect of high-dose ifosfamide in advanced soft tissue sarcomas. A multicentre phase II study of the EORTC Soft Tissue and Bone Sarcoma GroupEur J Cancer200036616710741296
- Le CesneAAntoineESpielmannMHigh-dose ifosfamide: circumvention of resistance to standard-dose ifosfamide in advanced soft tissue sarcomasJ Clin Oncol199513160016087541449
- CernyTLeyvrazSvon BrielTSaturable metabolism of continuous high-dose ifosfamide with mesna and GM-CSF: a pharmacokinetic study in advanced sarcoma patients. Swiss Group for Clinical Cancer Research (SAKK)Ann Oncol1999101087109410572607
- O’BryanRMLuceJKTalleyRWGottliebJABakerLHBonadonnaGPhase II evaluation of adriamycin in human neoplasiaCancer197332184716773
- FrustaciSBuonadonnaAGalligioniEIncreasing 4’-epidoxorubicin and fixed ifosfamide doses plus granulocyte-macrophage colony-stimulating factor in advanced soft tissue sarcomas: a pilot studyJ Clin Oncol199715141814269193334
- MaurelJFraJLopez-PousaASequential dose-dense doxorubicin and ifosfamide for advanced soft tissue sarcomas: a Phase II trial by the Spanish Group for Research on Sarcomas (GEIS)Cancer20041001498150615042685
- PatelSRVadhan-RajSBurgessMAResults of two consecutive trials of dose-intensive chemotherapy with doxorubicin and ifosfamide in patients with sarcomasAm J Clin Oncol1998213173219626808
- ReichardtPTilgnerJHohenbergerPDorkenBDose-intensive chemotherapy with ifosfamide, epirubicin, and filgrastim for adult patients with metastatic or locally advanced soft tissue sarcoma: a phase II studyJ Clin Oncol199816143814439552049
- LeyvrazSZweifelMJundtGLong-term results of a multicenter SAKK trial on high-dose ifosfamide and doxorubicin in advanced or metastatic gynecologic sarcomasAnn Oncol20061764665116500907
- JudsonISystemic therapy of soft tissue sarcoma: an improvement in outcomeAnn Oncol200415Suppl 4iv193iv19615477307
- Le CesneAJudsonICrowtherDRandomized phase III study comparing conventional-dose doxorubicin plus ifosfamide versus high-dose doxorubicin plus ifosfamide plus recombinant human granulocyte-macrophage colony-stimulating factor in advanced soft tissue sarcomas: A trial of the European Organization for Research and Treatment of Cancer/Soft Tissue and Bone Sarcoma GroupJ Clin Oncol2000182676268410894866
- VermaSYounusJStys-NormanDHaynesAEBlacksteinMDose-intensive chemotherapy with growth factor or autologous bone marrow/stem cell transplant support in first-line treatment of advanced or metastatic adult soft tissue sarcoma: a systematic reviewCancer20081121197120518224666
- FayetteJPenelNChevreauCPhase III trial of standard versus dose-intensified doxorubicin, ifosfamide and dacarbazine (MAID) in the first-line treatment of metastatic and locally advanced soft tissue sarcomaInvest New Drugs2009116[Epub ahead of print]
- DirixLYVan OosteromATSoft tissue sarcoma in adultsCurr Opin Oncol19991128529510416881
- FayetteJBlayJYGenetic predictors for drug resistance in soft tissue sarcoma: a review of publications in 2004Curr Opin Oncol20051737037515933471
- FataFO’ReillyEIlsonDPaclitaxel in the treatment of patients with angiosarcoma of the scalp or faceCancer1999862034203710570428
- HensleyMLMakiRVenkatramanEGemcitabine and docetaxel in patients with unresectable leiomyosarcoma: results of a phase II trialJ Clin Oncol2002202824283112065559
- CosettiMWexlerLHCallejaEIrinotecan for pediatric solid tumors: the Memorial Sloan-Kettering experienceJ Pediatr Hematol Oncol20022410110511990694
- RiggiNCironiLSuvaMLStamenkovicISarcomas: genetics, signalling, and cellular origins. Part 1: The fellowship of TETJ Pathol200721342017691072
- SuvaMLCironiLRiggiNStamenkovicISarcomas: genetics, signalling, and cellular origins. Part 2: TET-independent fusion proteins and receptor tyrosine kinase mutationsJ Pathol200721311713017703479
- MolinskiTFDalisayDSLievensSLSaludesJPDrug development from marine natural productsNat Rev Drug Discov20098698519096380
- MartinezEJCoreyEJA new, more efficient, and effective process for the synthesis of a key pentacyclic intermediate for production of ecteinascidin and phthalascidin antitumor agentsOrg Lett2000299399610768205
- CuevasCPerezMMartinMJSynthesis of ecteinascidin ET-743 and phthalascidin Pt-650 from cyanosafracin BOrg Lett200022545254810956543
- ErbaEBergamaschiDBassanoLEcteinascidin-743 (ET-743), a natural marine compound, with a unique mechanism of actionEur J Cancer2001379710511165136
- Zewail-FooteMHurleyLHEcteinascidin 743: a minor groove alkylator that bends DNA toward the major grooveJ Med Chem1999422493249710411470
- TakebayashiYPourquierPZimonjicDBAntiproliferative activity of ecteinascidin 743 is dependent upon transcription-coupled nucleotide-excision repairNat Med2001796196611479630
- SoaresDGEscargueilAEPoindessousVReplication and homologous recombination repair regulate DNA double-strand break formation by the antitumor alkylator ecteinascidin 743Proc Natl Acad Sci U S A2007104130621306717656556
- GajateCAnFMollinedoFDifferential cytostatic and apoptotic effects of ecteinascidin-743 in cancer cells. Transcription-dependent cell cycle arrest and transcription-independent JNK and mitochondrial mediated apoptosisJ Biol Chem2002277415804158912198119
- IzbickaELawrenceRRaymondEIn vitro antitumor activity of the novel marine agent, ecteinascidin-743 (ET-743, NSC-648766) against human tumors explanted from patientsAnn Oncol199899819879818072
- LiWWTakahashiNJhanwarSSensitivity of soft tissue sarcoma cell lines to chemotherapeutic agents: identification of ecteinascidin-743 as a potent cytotoxic agentClin Cancer Res2001729081111555609
- ValotiGNicolettiMIPellegrinoAEcteinascidin-743, a new marine natural product with potent antitumor activity on human ovarian carcinoma xenograftsClin Cancer Res19984197719839717828
- HendriksHRFiebigHHGiavazziRLangdonSPJimenoJMFairclothGTHigh antitumour activity of ET743 against human tumour xenografts from melanoma, non-small-cell lung and ovarian cancerAnn Oncol1999101233124010586342
- BrandonEFMeijermanIKlijnJSIn vitro cytotoxicity of ET-743 (Trabectedin, Yondelis), a marine anti-cancer drug, in the Hep G2 cell line: influence of cytochrome P450 and phase II inhibition, and cytochrome P450 inductionAnticancer Drugs20051693594316162970
- van KesterenCCvitkovicETaammaAPharmacokinetics and pharmacodynamics of the novel marine-derived anticancer agent ecteinascidin 743 in a phase I dose-finding studyClin Cancer Res200064725473211156226
- BeumerJHRademaker-LakhaiJMRosingHLopez-LazaroLBeijnenJHSchellensJHTrabectedin (Yondelis, formerly ET-743), a mass balance study in patients with advanced cancerInvest New Drugs20052342943616133794
- ForouzehBHidalgoMDenisLPhase I and pharmacokinetic study of the marinederived DNA minor groove binder ET-743 on a weekly × 3 every-4-week schedule in patients with advanced solid malignanciesProc Am Soc Clin Oncol200120Abstract # 373
- RyanDPSupkoJGEderJPPhase I and pharmacokinetic study of ecteinascidin 743 administered as a 72-hour continuous intravenous infusion in patients with solid malignanciesClin Cancer Res2001723124211234874
- TaammaAMissetJLRiofrioMPhase I and pharmacokinetic study of ecteinascidin-743, a new marine compound, administered as a 24-hour continuous infusion in patients with solid tumorsJ Clin Oncol2001191256126511230466
- TwelvesCHoekmanKBowmanAPhase I and pharmacokinetic study of Yondelis (Ecteinascidin-743; ET-743) administered as an infusion over 1 h or 3 h every 21 days in patients with solid tumoursEur J Cancer2003391842185112932661
- Villalona-CaleroMAEckhardtSGWeissGA phase I and pharmacokinetic study of ecteinascidin-743 on a daily × 5 schedule in patients with solid malignanciesClin Cancer Res20028758511801542
- YovineARiofrioMBlayJYPhase II study of ecteinascidin-743 in advanced pretreated soft tissue sarcoma patientsJ Clin Oncol20042289089914990645
- Le CesneABlayJYJudsonIPhase II study of ET-743 in advanced soft tissue sarcomas: a European Organisation for the Research and Treatment of Cancer (EORTC) soft tissue and bone sarcoma group trialJ Clin Oncol2005235768415659504
- Garcia-CarboneroRSupkoJGManolaJPhase II and pharmacokinetic study of ecteinascidin 743 in patients with progressive sarcomas of soft tissues refractory to chemotherapyJ Clin Oncol2004221480149015084621
- MorganJALe CesneAChawlaSYondelis Sarcoma Study GroupRandomized phase II study of trabectedin in patients with liposarcoma and leiomyosarcoma (L-sarcomas) after failure of prior anthracylines (A) and ifosfamide (I)J Clin Oncol200725620Supplement18SASCO Annual Meeting Proceedings Part I Vol 25, No 18S (June 20 Supplement), 10060.
- BlayJYLe CesneAVerweijJA phase II study of ET-743/trabectedin (‘Yondelis’) for patients with advanced gastrointestinal stromal tumoursEur J Cancer2004401327133115177491
- Le CesneAMissetJLDemetriGConsistent evidence of activity of ecteinascidin (ET-743) in pretreated, advanced soft tissue sarcoma (ASTS): results from a pooled analysis of three pivotal phase II clinical trials (p2ct) and safety profile of a 24 h infusion scheduleEuropean Journal of Cancer200137S34S
- D’IncalciMJimenoJPreclinical and clinical results with the natural marine product ET-743Expert Opin Investig Drugs20031218431853
- GrossoFDileoPSanfilippoRSteroid premedication markedly reduces liver and bone marrow toxicity of trabectedin in advanced sarcomaEur J Cancer20064214849016737808
- HuyghGClementPMDumezHEcteinascidin-743: evidence ofactivity in advanced, pretreated soft tissue and bone sarcoma patientsSarcoma20065628217496996
- GrossoTrabectedin in Soft Tissue Sarcomas (STS) carrying a chromosomal translocation: an exploratory analysisSeattle, WA13th CTOS meetingNov 1–3, 2007Abstract # 900 2007.
- DileoMFinal results of a phase II trial of 3-hr infusion trabectedin in patients with recurrent sarcomasIstanbul, Turkey31st ESMO CongressSept 29 – Oct 3, 2006Abstract # 524P 2006
- MohanVUpdated results of Phase II study of trabectedin (ET-743) in pretreated patients with advanced/ metastatic soft tissue sarcoma from a single instituteChicago, ILASCO American Society of Clinical Oncology, 44th Annual MeetingMay 30 – Jun 3, 2008Abstract # 21506 2008
- Van GlabbekeMVerweijJJudsonINielsenOSProgression-free rate as the principal end-point for phase II trials in soft-tissue sarcomasEur J Cancer20023854354911872347
- Garcia-CarboneroRSupkoJGMakiRGEcteinascidin-743 (ET-743) for chemotherapy-naive patients with advanced soft tissue sarcomas: multicenter phase II and pharmacokinetic studyJ Clin Oncol2005235484549216110008
- GrossoFJonesRLDemetriGDEfficacy of trabectedin (ecteinascidin-743) in advanced pretreated myxoid liposarcomas: a retrospective studyLancet Oncol2007859560217586092
- DonaldSVerschoyleRDGreavesPComplete protection by high-dose dexamethasone against the hepatotoxicity of the novelantitumor drug yondelis (ET-743) in the ratCancer Res2003635902590814522916
- DonaldSVerschoyleRDGreavesPOrrSJimenoJGescherAJComparison of four modulators of drug metabolism as protectants against the hepatotoxicity of the novel antitumor drug yondelis (ET-743) in the female rat and in hepatocytes in vitroCancer Chemother Pharmacol20045330531214669039
- PuchalskiTARyanDPGarcia-CarboneroRPharmacokinetics of ecteinascidin 743 administered as a 24-h continuous intravenous infusion to adult patients with soft tissue sarcomas: associations with clinical characteristics, pathophysiological variables and toxicityCancer Chemother Pharmacol20025030931912357306
- SkorupaABeldnerMKraftAMonteroAJFatal rhabdomyolysis as a complication of ET-743 (Yondelis) chemotherapy for sarcomaCancer Biol Ther2007671015101717611408
- FriedmanDHuZKolbEAGorfajnBScottoKWEcteinascidin-743 inhibits activated but not constitutive transcriptionCancer Res2002623377338112067978
- JinSGorfajnBFairclothGScottoKWEcteinascidin-743, a transcription-targeted chemotherapeutic that inhibits MDR1 activationProc Natl Acad Sci U S A2000976775677910841572
- MinuzzoMCeribelliMPitarque-MartiMSelective effects of the anticancer drug Yondelis (ET-743) on cell-cycle promotersMol Pharmacol2005681496150315961672
- ForniCMinuzzoMVirdisETrabectedin (ET-743) promotes differentiation in myxoid liposarcoma tumorsMol Cancer Ther2009844945719190116
- HerreroABMartin-CastellanosCMarcoEGagoFMorenoSCross-talk between nucleotide excision and homologous recombination DNA repair pathways in the mechanism of action of antitumor trabectedinCancer Res2006668155816216912194
- SchöffskiPDNA repair functionality modulates the clinical outcome of patients with advanced sarcoma treated with trabectedin (ET-743)Journal of Clinical Oncology2006 ASCO Annual Meeting Proceedings Part I2418S620Supplement20069522
- MecoDColomboTUbezioPEffective combination of ET-743 and doxorubicin in sarcoma: preclinical studiesCancer Chemother Pharmacol20035213113812783202
- RiccardiAMecoDUbezioPCombination of trabectedin and irinotecan is highly effective in a human rhabdomyosarcoma xenograftAnticancer Drugs20051681181516096428
- TakahashiNLiWWBanerjeeDScottoKWBertinoJRSequencedependent enhancement of cytotoxicity produced by ecteinascidin 743 (ET-743) with doxorubicin or paclitaxel in soft tissue sarcoma cellsClin Cancer Res200173251711595721
- SessaCPerottiANoberascoCPhase I clinical and pharmacokinetic study of trabectedin and doxorubicin in advanced soft tissue sarcoma and breast cancerEur J Cancer20081227[Epub ahead of print]
- von MehrenMSchilderRJChengJDA phase I study of the safety and pharmacokinetics of trabectedin in combination with pegylated liposomal doxorubicin in patients with advanced malignanciesAnn Oncol2008191802918497430
- PapadopoulosPhase I and pharmacokinetics (PK) study of sequential paclitaxel and trabectedin every 2 weeks in patients with advanced solid tumorsJ Clin Oncol2006ASCO Annual Meeting Proceedings Part I200624620Supplement18S2029
- GoreLPhase I combination study of trabectedin (T) and capecitabine (C) in patients with advanced malignanciesJ Clin Oncol2006ASCO Annual Meeting Proceedings Part I200624620Supplement18S2079