Abstract
Topical anesthetics have evolved from a simple solution of cocaine to creams, ointments, gels, liposomal preparations, and to the latest sophisticated patches and peels. Topical anesthetics are essential for performing diagnostic, therapeutic, and cosmetic dermatology procedures. These anesthetics noninvasively deliver anesthesia in locally required areas. In this review, we present an overview on the mechanism of precutaneous absorption of skin and address the composition, duration of onset of anesthetic effect, uses, and side effects that are applicable for the products. Also discussed are the novel advances of using heat to enhance penetration of the anesthetic as seen in Synera™ patch and delivery of anesthesia using a peel method as seen in the yet to be US Food and Drug Administration-approved S-Caine peel.
Introduction
For centuries, topical application of medications has mostly been utilized for the treatment of localized skin diseases. Topical treatment was meant to treat the disease state locally with little or no systemic effects (CitationCleary 1984). This review focuses on the products available for producing the local anesthetic effects necessary for performing diagnostic, therapeutic, and cosmetic dermatologic procedures.
The first topical anesthetic discovered was cocaine. It was extracted from the leaves of Erythroxylon coca, a plant originally found in South America (CitationRitchie and Greene 1980). For centuries the natives had chewed the leaves for their euphoric effects (CitationDyke and Byck 1982). Nieman first isolated cocaine alkaloid in its pure form in 1859 (CitationFink 1985) and noted its ability to numb the tongue (CitationFaulconor and Keys 1965), and Koller was the first to use it as a topical anesthetic for eye surgery (CitationBerger 2000). An ideal topical anesthetic produces effective anesthesia within minutes when applied to intact skin, has prolonged duration of action, and has minimal side effects. Another potential benefit of using topical anesthetics is avoiding disruption of anatomical landmarks. Over the past 150 years, topical anesthetics have evolved from a simple solution of cocaine to creams, ointments, gels, liposomal preparations, and to the latest sophisticated patches and peels. Iontophoresis and sonopheresis have also been utilized to enhance the anesthetic delivery.
Anatomy of skin and percutaneous absorption
Delivery of a drug through the skin is a complex process, and this can be better appreciated by briefly reviewing the anatomy of the skin. Skin is an effective barrier and its vital role is to prevent the ingress or egress of compounds across it. When this barrier function is compromised for any reason, it results in loss of body fluids and also becomes a port of entry for microorganisms into the body as seen in burns patients and various dermatological conditions. Therefore, skin plays a key role in protecting the body from various environmental insults, both biological and chemical (CitationBucks and Maibach 2002). The skin is composed of the outermost epidermis, which is avascular, and the dermis, which is vascular, and which contains the free nerve endings that are responsible for pain sensation. Hence, the target area for the anesthetic action is the dermis. The pilosebaceous, apocrine, and eccrine glands originate in the dermis. These glands penetrate through the epidermis to reach the surface of the skin. The dermis is further supported by subcutaneous fat and muscle beneath. The superficial layer of epidermis is the stratum corneum. Stratum corneum is almost impermeable and responsible for the barrier function of the skin. It plays a vital role in the absorption of drugs. Stratum corneum therefore provides the rate-limiting step in the penetration process (CitationBarry et al 1987).
When a drug is applied to intact skin, it first has to traverse through the stratum corneum, and to do this, the drug has to partition from the vehicle into the stratum corneum. As stratum corneum is lipophilic, usually a drug in its base form is ideal. The viable part of epidermis and the dermis are hydrophilic, and the drug has to be in an ionized state for optimal permeation. When the drug arrives at the interface of stratum corneum and the viable epidermis, it has to partition into the hydrophilic tissue. On further penetration, the drug has to partition into the dermis that is again hydrophilic. Enroute through the layers of the skin, the drug undergoes metabolism by enzymes present in the skin to more active or inactive compounds. Some of the drug interacts with binding sites forming a depot. The drug on further penetration reaches subcutaneous tissue and muscle. These tissues may also act as a depot leading to sustained release (CitationSchuplein 1978; CitationFlynn 1979; CitationChien 1982; CitationSchaefer et al 1982; CitationGuy and Hadgraft 1984; CitationBronaugh and Maibach 1985; CitationMarty et al 1985; CitationBucks et al 2002).
The penetration of drugs through the skin involves diffusion via transcellular and intercellular pathways, and via hair follicles and sweat glands. The permeation through the appendages allows diffusional leakage into the epidermis and penetration directly into the dermis. This is supposedly the fastest route for hydrophilic molecules. However, the major transport pathway is through the intercellular lipid domains. (CitationKatz and Poulsen 1971; CitationKatz 1973; CitationPoulsen 1973; CitationIdson 1976; CitationHiguchi 1977).
Transport of an anesthetic depends on its time-scale of permeation that is either steady state or transient diffusion, the pKa of the drug, molecular size, stability, binding affinity, solubility, partition co-efficient, integrity and thickness of stratum corneum, density of sweat glands and hair follicles, skin hydration, metabolism, and the vehicle effects (CitationRanade and Hollinger 2003). The pKa of an anesthetic is the pH at which a drug exists both in non-ionic (base) and ionic (salt) states in equal proportions (CitationCovino 1986). As mentioned earlier, base is the active form that permeates through the stratum corneum. The closer the pKa of the drug to the pH of the vehicle and the skin, the more of the drug is in its active base form and hence its penetration is higher (CitationSchaefer et al 1982).
For optimizing the percutaneous absorption of topically applied drugs, two strategies are utilized in formulations. The first strategy is using a vehicle or device which maximizes drug delivery into the skin without affecting the physiochemical properties of stratum corneum and the second is using penetration enhancers. These enhancers enter into the skin and alter it reversibly to promote the drug absorption. An ideal enhancer should be pharmacologically inert, non-toxic, non-irritating or non-allergenic, and a suitable solvent for the drug (CitationWoodford and Barry 1986; CitationBarry et al 1987).
Occlusion is a physical method utilized to enhance the permeation of the anesthetic through the skin. It impairs the passive transepidermal loss of water at the site of application, and increases water content of intercellular areas. This is responsible for increase in the hydrophilic character of the stratum corneum, reducing the stratum corneum–viable epidermis partition coefficient of the penetrant (CitationBucks and Maibach 2002).
Mechanism of cutaneous analgesia
The mechanism by which an anesthetic works is by inhibiting the initiation and propagation of nerve impulses. This is achieved by the base form of the drug by penetrating through the axolemma, the outer nerve sheet, and blocking the influx of sodium ions into the nerve cell, thereby dampening the generation of action potential.
Product review
EMLA
Eutectic mixture of local anesthetics (EMLA) is based on an eutectic mixture of two well known local anesthetics lidocaine and prilocaine. EMLA is an oil-in-water emulsion mixture. The oil phase consists of the eutectic mixture lidocaine and prilocaine. A eutectic mixture is one in which its constituents melt at room temperature and are present in liquid phase. Broberg when working with emulsion mixtures had first discovered this property serendipitously. He found that when lidocaine and prilocaine bases in crystalline form were mixed together, they became fluid at room temperature. This is secondary to lowering of the melting points of both the constituents in the mixture. This effect is best produced when the drugs were mixed in 1:1 ratio (CitationJuhlin and Evers 1990). With the discovery of eutectic mixture, an oil-in-water emulsion can be prepared with highest concentration of the active ingredients (CitationLycka 1992). In EMLA, the concentration of lidocaine and prilocaine achieved in the oil droplet is 80% though the overall concentration of both the active drugs is kept as low as 5% in the mixture. This is secondary to the emulsifiers present in the mixture. This reduction in concentration is responsible for decreased systemic toxicity (CitationWatson 1986).
Each gram of EMLA is composed of lidocaine 25 mg/ml and prilocaine 25 mg/ml, polyoxyethylene fatty acid esters that are emulsifiers, carboxypolymethylene that is a thickening agent, distilled water with pH adjusted approximately to 9, and without any preservative (CitationAstraZeneca 2004). It was released in the US in 1993 and is Food and Drug Administration (FDA)-approved for use only on procedures involving intact skin.
EMLA has to be applied under occlusive dressings like Tegaderm™, Saran-wrap™, or Band-aid™, which aids diffusion into the skin (CitationLycka 1992). The onset of anesthesia depends on anatomic location and duration of application. On face and thighs, for needle stick purposes, the onset is less than 25 minutes (CitationHolmes 1994). For procedures on mucous membranes involving oral and genitalia, the onset is in 5–15 minutes without occlusion (CitationRylander et al 1990). EMLA does not provide effective anesthesia on thick glabrous skin like palms and soles and is not recommended for procedures in these areas (CitationHuang and Vidimos 2000).
The recommended application time for adequate analgesia is at least 1 hour. For painful procedures like split skin grafting, the recommended application time is 2 hours (CitationLahteenmaki et al 1988). Maximum effect is reached at 2–3 hours of application time and lasts for at least 1–2 hours after removal (CitationAstraZeneca 2004). In several clinical trials, EMLA was found to produce adequate dermal analgesia when applied under occlusive dressing for 60 minutes, and inadequate analgesia when applied for 30 minutes only (CitationEvers et al 1985; CitationMcCafferty and Woolfson 1993; CitationGreenbaum and Bernstein 1994). EMLA forms as a depot in the stratum corneum during occlusion (CitationEvers et al 1985; CitationArendt-Nielsen and Bjerring 1988), which results in continued and even increase in analgesia 15–60 minutes after removal of the medication (CitationEvers et al 1985; CitationArendt-Nielsen and Bjerring 1988; CitationFriedman et al 1999). The onset of analgesia can be enhanced by pretreatment with low frequency ultrasound (55 KHz) before application of EMLA and it was found to be as early as 5 minutes (CitationKatz et al 2004). Rapid onset was also found when EMLA was applied for 20 minutes with heat (CitationLiu et al 2003).
The duration of analgesia is influenced by the vascularity of the local area; the more vascular, the more clearance, and hence the wearing off effect happens sooner. For example, on the face, the duration of anesthetic effect is shortened (CitationArendt-Neilsen et al 1990; CitationLarsson et al 1996). The depth of an anesthetic effect depends mainly on the duration of application. When applied for 60 minutes, the depth of anesthetic effect was found to be 3 mm, and for 120 minutes of application time, the depth of anesthetic effect was found to be 5 mm (CitationBjerring and Arendt-Nielsen 1990). In a study evaluating anesthesia for punch biopsies, EMLA was found to provide effective anesthesia to a depth of 1–2 mm when applied for 60 minutes, 2–3 mm when applied for 120 minutes, and 6 mm when applied for 3–4 hours (CitationWahlgren and Quiding 2000). When EMLA was applied on intact skin under occlusive dressing and left for 3 hours and 24 hours, the plasma levels of both lidocaine and prilocaine were found to be well below systemic toxic level. The peak lidocaine levels were 1/20 and prilocaine levels were 1/36 of the systemic toxic levels (CitationAstraZeneca 2004). In a study involving 10 patients, when 5–10 g of EMLA was applied to chronic leg ulcers for a period of 24 hours, plasma concentrations of lidocaine and prilocaine were found to be less than 1/5th of those associated with toxic reactions (CitationStymne and Lillieborg 2001).
In dermatologic procedures, EMLA was found to be effective in relieving pain associated with shave (CitationShelley 1975) and punch biopsies (CitationJuhlin et al 1980), curettage of molluscum (CitationRosdahl et al 1988), split thickness skin grafting (CitationGoodacre et al 1988), chemical peels (CitationLycka 1991), epilation (CitationHjorth et al 1991), vascular laser treatments (CitationAshinoff and Geronemus 1990; CitationTan and Stafford 1992; CitationSherwood 1993), facial laser resurfacing (CitationRamos-Zabala et al 2004), laser hair removal (CitationGuardiano and Norwood 2005), excisional biopsy or curettage, and electro-surgery (CitationGupta and Sibbald 1996). EMLA has also been found to be useful prior to procedures like venepuncture in neonates (CitationHallen et al 1984; CitationKurien et al 1985; CitationMoller 1985), venous cannulation (CitationRussell and Doyle 1997), lumber puncture (CitationKapelushnik et al 1990), sharp wound debrediment, leg ulcers (CitationHolm et al 1990; CitationHolst and Kristofferson 1998; CitationLok et al 1999; CitationRosenthal et al 2001), decubitus ulcers, abscess revisions, post-op wounds, diabetic ulcers, burns (CitationBlanke and Hallern 2003), and post-burn pruritus in children when applied to newly healing intact skin (CitationKopecky et al 2001). EMLA did not provide effective anesthesia for procedures on external ear (CitationSarifakioglu et al 2004) As for those on oral mucosa, EMLA provided anesthesia only for superficial layers and for short term procedures only (CitationBernardi et al 1999). EMLA provided comparable anesthesia as LMX for hair removal with Nd: YAG 1064 nm laser (CitationGuardiano and Norwood 2005).
Local effects are initial transient blanching followed by erythema. This is secondary to the bi-phasic effect on cutaneous blood vessels at the application site. Blanching is seen in 1.5 hours of application secondary to vasoconstritive effect (this effect does not favor emergency venous cannulations), and this is followed by erythema in 2–3 hours of application resulting from vasodilatory effect (CitationBjerring et al 1989). Itching and edema can occur. With repeated applications, local reactions are exacerbated but resolve after stopping the medication (CitationEvers et al 1985; CitationWehle et al 1989). Contact urticaria (CitationWaton et al 2004) and dermatitis (CitationIsmail and Goldsmith 2005) have also been reported. Any contact with eye should be avoided as EMLA irritates the cornea and its high pH 9 may produce lesions similar to corneal abrasions and ulcerations (CitationBrahma and Inkster 1995; CitationEaglstein 1999; CitationMcKinlay et al 1999).
Plasma levels where toxic reactions seen are 6 μg/ml. In studies done in children older than 3 months of age, when EMLA was applied for 4 hours to intact skin, plasma levels of lidocaine were shown to be 0.155 μg/ml, and prilocaine were 0.131 μg/ml, which were well below the toxic levels (CitationEngberg et al 1987). A well documented major systemic side effect of using EMLA is methemoglobinemia produced secondary to prilocaine. This is due to the oxidation of iron in hemoglobin from ferrous to ferric state, decreasing the oxygen carrying capacity of hemoglobin. This results in cyanosis when levels reach around 5%–15% (CitationRussell and Doyle 1997). EMLA is not recommended in infants younger than 12 months of age who are on methemoglobinemia-inducing drugs, patients with glucose-6-phosphate dehydrogenase (G6PD) deficiency and with congenital or idiopathic methemoglobinemia (CitationAstraZeneca 2004). It should be used with caution in infants less than 3 months of age because of the incomplete maturation of nicotinamide adenine dinucleotide (NADH)-methemoglobinemia reductase system (CitationBrisman et al 1998). A maximum of 1 g for an hour of application is safe on intact skin of term neonates younger than 3 months (CitationRincon et al 2000). Central nervous system (CNS) toxicity was also reported in a toddler when excessive EMLA was applied over an extensive area prior to molluscum treatment (CitationJuhlin et al 1989).
Usage of EMLA is contraindicated in the presence of history of amide sensitivity, liver disease, and skin diseases like atopic dermatitis, or psoriasis (CitationJuhlin and Rollman 1984). In the later it is secondary to higher rates of absorption from inflamed areas.
TAC solution
Tetracaine, adrenaline (epinephrine), and cocaine (TAC) solution is a dermal anesthetic. They are used for open wounds, such as lacerations and abrasions, to provide anesthetic effect prior to wound repair. The original formulation of TAC solution consisted of tetracaine 0.5%, 0.05% epinephrine 1:2000, and 11.8% cocaine in normal solution. At this concentration, each ml of TAC solution contains 5 mg tetracaine, 0.5 mg epinephrine, and 118 mg cocaine. Since 1980, TAC solution has been used as an alternative to infiltrative anesthesia with lidocaine for repair of minor superficial lacerations (CitationPryor et al 1980; CitationAnderson et al 1990, CitationHuang and Vidimos 2000). It was found to work better for scalp and facial lacerations than on extremities (CitationHegenbarth et al 1990). The same was found when different formulations of TAC solution were compared (CitationBonadio and Wagner 1988b; CitationSmith and Barry 1990; CitationVinci and Fish 1996). TAC solution was 95% effective in providing anesthesia prior to repair of lacerations on face and neck in children, with no adverse events even on application to an area with a length of 5 cm and a depth of 5 mm (CitationBonadio and Wagner 1988a). TAC solution is applied to the laceration with a cotton ball or gauze pad soaked in the solution (CitationGrant and Hoffman 1992).
For a laceration up to 5 cm in length, the recommended dosing of TAC solution is from 2–5 ml. One dosing regimen is as per weight, 0.09 ml/kg of TAC solution that contains approximately 10 mg/kg of cocaine (CitationHegenbarth et al 1990). Another regimen suggests 1 ml of TAC solution per cm of laceration (CitationCannon et al 1989). Application for at least 20 minutes prior to suturing produced effective anesthesia in children (CitationOrdog and Ordog 1994).
Effectiveness can be determined clinically by visible blanching (CitationNichols et al 1987; CitationHegenbarth et al 1990; CitationAnderson et al 1990). The epinephrine and cocaine in the preparation produce vasoconstriction leading to a prolonged presence of the drug at the site of application, inhibiting the absorption of the drugs into systemic circulation, resulting in fewer systemic effects (CitationRussell and Doyle 1997).
TAC solution is not recommended for usage on mucous membranes, burn areas, or large abrasions due to the risk of rapid absorption leading to systemic toxicity. It is also not recommended for areas supplied by terminal arterioles (CitationMcCafferty et al 1989; CitationRussell and Doyle 1997).
Very low plasma levels of cocaine were detected on application of 3 ml of TAC solution for 15 minutes in 75% of children. Tetracaine levels were not detected (CitationTerndrup et al 1992). Urine drug screen was found to be positive for cocaine for up to 36–48 hours after usage of TAC solution (CitationAltieri et al 1990).
Local adverse effects of TAC solution were thought to be due to the combined vasoconstrictive effects of epinephrine and cocaine. As a result of this, blood circulation is decreased at the application site, which leads to a decrease in tissue defenses. There is a possibility for an increased risk of wound infection and thereby decreased healing capacity of the wound (CitationBarker et al 1982; CitationGrant and Hoffman 1992). This could eventually lead to wound dehiscence in extreme cases (CitationGalvin and De Simone 1976; CitationGosnold 1977; CitationRutherford and Spence 1980; CitationAlkan et al 1984). It is also contraindicated for usages anywhere near the eye area as it was found to produce corneal abrasions (CitationBonadio and Wagner 1990).
Systemic reactions were reported when TAC solution was applied at or near the mucous membranes. This is secondary to the rapid and uninhibited absorption of cocaine and tetracaine from the mucosa. As the individual components are toxic by themselves, in combination their toxicities are much more potentiated. Severe adverse events including respiratory distress, seizures (CitationWehner and Hamilton 1984; CitationTipton et al 1989) and death (CitationJacobsen 1987; CitationDailey 1988) have been reported.
Because of the potential for systemic absorption of cocaine and resulting side effects, and because cocaine is a regulated drug, TAC solution is not FDA-approved. New formulations without cocaine have been tried to compare their efficacy against TAC solution. At the same concentrations, TAC without cocaine was found to be less effective than the original TAC solution (CitationSchaffer 1985). The same result was found when TAC solution was compared with tetracaine alone (CitationWhite et al 1986).
The formulations that were found to be equally effective as TAC solution are: LAT containing 4% lidocaine, adrenaline 1:2000, and 1% tetracaine in both children (CitationErnst et al 1995a; CitationSchilling et al 1995) and adults (CitationErnst et al 1995b); lidocaine 5%–epinephrine 1:2000-containing solution (CitationBlackburn et al 1995); tetraphen containing 1% tetracaine with 5% phenylephrine (CitationSmith et al 1997); and bupivanor containing bupivicaine and norepinephrine (CitationSmith et al 1996). EMLA was found to be superior to TAC, though EMLA is recommended only for intact surfaces (CitationAnderson et al 1990).
Amethocaine
Amethocaine is a 4% tetracaine gel and was first synthesized in 1928 by Eisleb. It has to be applied under occlusive dressing. Tetracaine is a lipophilic compound and it easily diffuses through the stratum corneum because of this property (CitationCovino 1986). This intrinsic property is responsible for rapid onset of anesthetic effect within 40 minutes (CitationLawson et al 1995). Due to the same property, it is held as a reservoir in the skin, which is responsible for sustained release resulting in a prolonged duration of action of approximately 4 hours (CitationMcCafferty et al 1989). In dermatology, for pulsed dye laser treatment of port-wine stains, amethocaine was found to be significantly better in reducing pain when compared with EMLA (CitationMcCafferty et al 1997). This was a randomized, double-blind and placebo-controlled study involving 29 patients. The amethocaine preparation was found significantly better than EMLA, p < 0.05 by visual analog scale (VAS) pain scoring system and p < 0.005 by verbal rating score (VRS) pain scoring system. The results from this study seem to be reliable based on the p values. It was not found to be effective when compared with placebo either during or after photodynamic therapy for small lesions of superficial basal cell carcinoma, Bowen’s disease or actinic keratosis (CitationHolmes et al 2004).
When compared with placebo, amethocaine gel was found to provide good analgesic action for skin puncturing procedural pain in neonates (CitationMoore 2001). When used prior to minor surgical procedures like venous cannulation in both adults (CitationMolodecka et al 1994) and children (CitationLawson et al 1995), amethocaine was found to be as effective as EMLA. Amethocaine was efficacious for relieving pain prior to venepuncture in children when compared with placebo (CitationJain and Rutter 2000). However, in procedures like heel prick blood sampling (newborns) (CitationJain et al 2001), arterial puncture (CitationTran et al 2002), it was not effective in reducing pain. For radial artery cannulation in adults, topical amethocaine provided comparable anesthetic effect as with lidocaine infiltration (CitationOlday et al 2002).
The most common local effect was erythema. Other effects were itching and edema, although not commonly seen (CitationO’Connor and Tomlinson 1995). Secondary to absent or very low systemic levels upon topical application; systemic adverse effects are rarely seen. In a study involving 10 subjects on topical application of amethocaine, three subjects had plasma concentrations of 0.20 mg liter−1 without any significant side effects. The absence of side effects was concluded to be secondary to slow absorption and tissue hydrolysis of amethocaine after topical dermal application (CitationMazumdar et al 1991).
A new micro emulsion formulation of amethocaine in preclinical studies done in rats was found to be promising in providing rapid and effective anesthetic effect against heat and mechanical stimulus when compared with amethocaine gel, EMLA, lidocaine infiltration, or nothing (CitationArevalo et al 2004). A novel patch, made of hydroxypropylcellulose discs containing tetracaine (1 mg × cm2) and surrounded by a low tack pressure-sensitive adhesive backing layer was found to be effective in reducing pain prior to venepuncture in both term and pre-term infants (CitationLong et al 2004).
LMX (ELA-Max)
LMX is a topical liposomal formulation containing 4% or 5% lidocaine. Liposomes have similar structure as cell membrane, made up of lipid bi-layers. This structure enhances the penetration of the drug, leading to rapid onset of action (CitationFinkel et al 2002) and prevents metabolic degradation at the application site, which leads to a prolonged duration of action (CitationBucalo et al 1998), and also helps in sustained release of the drug (CitationYun et al 2002).
LMX 4% is available over the counter and is FDA-approved for temporary relief of pain and itching associated with minor cuts, minor burns, sunburn, and insect bites. The 5% preparation needs prescription and has been approved for anorectal pain. Both the preparations can be used without occlusion unlike EMLA, but if cooperation is an issue as faced in pediatrics, LMX can be used under occlusion with tegaderm and is supplied as 5 g tubes for this purpose. Each gram of LMX contains lidocaine 40 mg, vitamin E acetate, propylene glycol, benzyl alcohol, lecithin, cholesterol, carbomer 940, triethanolamine, polysorbate 80, and purified water (CitationHuang and Vidimos 2000).
LMX provides effective anesthesia prior to various procedures when applied for 30 minutes without occlusion unlike EMLA which needs 60 minutes with occlusion to get the same effect (CitationAltman and Gildenberg 1999; CitationEremia and Newman 2000; CitationKleiber et al 2002; CitationEichenfield et al 2002; CitationSmith and Gjellum 2004; CitationKoh et al 2004). Onset of LMX has been found to be further enhanced by pretreatment with erbium: yttrium-aluminum-garnet laser (CitationYun et al 2002).
In dermatologic procedures, LMX has been tested and found to be effective as topical anesthetic prior to hair removal procedures using laser (CitationEremia and Newman 2000) and high-energy pulsed light source devices (CitationAltman and Gildenberg 1999). However, both studies lacked good sample size and blinding. The latter study also did not involve randomization. In a recent double-blind and randomized study which evaluated the hair removal using Nd: YAG 1064 nm laser, both LMX and EMLA showed similar efficacy in reducing pain when applied for the same time period of 30 minutes (CitationGuardiano and Norwood 2005). In a comparative clinical trial with EMLA and placebo groups for medium-depth chemical peeling involving 10 patients, both LMX and EMLA showed equal efficacy in reducing the pain when applied for the same period of time without any clinical or histopathological difference between the treatment and control group (CitationKoppel et al 2000).
In randomized clinical studies in children comparing LMX and EMLA, the former was found to be safe and provided effective anesthesia in 30 minutes prior to intravenous (IV) insertions (CitationKleiber et al 2002; CitationKoh et al 2004) and venipuncture (CitationEichenfield et al 2002). In another study involving children, LMX provided similar pain and anxiety reduction during peripheral intravenous (PIV) insertion in children when compared with injected buffered lidocaine (CitationLuhmann et al 2004).
LMX has been found to be safe with very minor and few side effects. The local effects were transient blanching and erythema. The amount of lidocaine absorbed systemically depends on the duration and surface area of application. The recommendation in children is that the area of application should not be larger than 100 cm2 in a child weighing less than 10 kg or between 10–20 kg for a single application of LMX. Systemic effects are seen when plasma levels of lidocaine are over 5 μg/ml. The serum levels of lidocaine are in the range of 0.05–0.16 μg/ml when 60 g of LMX has been applied topically for 3 hours over an area of 400 cm2 of skin (CitationHuang and Vidimos 2000). These levels are very low when compared with the toxic levels and hence very low profiles of any serious adverse events were noticed.
As of now, LMX has the advantage of faster onset of anesthetic effect, no occlusion required, low profile of side effects, and no risk of methemoglobinemia when compared with EMLA. More studies are required to establish its efficacy prior to other dermatologic procedures.
Betacaine–LA
Betacaine LA contains lidocaine, prilocaine, dibucaine, and phenylephrine (a vasoconstrictor) in petrolatum base. The exact concentration of the ingredients is not revealed as it is a proprietary anesthetic. Concentration of lidocaine and prilocaine are four times that found in EMLA and therefore should be used cautiously (CitationFriedman, Mafong, et al 2001a).
In adults, betacaine–LA is not recommended to be used for areas more than 300 cm2 and is also not recommended for children (CitationFriedman, Mafong, et al 2001a). It can be applied without occlusion for 30–45 minutes to get adequate analgesia. The only comparative study with betacaine–LA was done under occlusion for 60 minutes, along with EMLA, LMX, and tetracaine. Anesthetic effect was assessed with Q-switched Nd: YAG laser at 1064 nm after 60 minutes of application time and 30 minutes after removal. Its efficacy was found to be superior to control at the end of 60 minutes, and 30 minutes after removal of the medication. Both EMLA and LMX were found to be more efficacious than betacaine– LA (CitationFriedman et al 1999). However, this is a weak study as it involves a small sample size (n = 12), lacks randomization, and involves subjective reporting of pain sensations.
Topicaine
Topicaine contains 4% or 5% lidocaine in a hydro-ethanolic gel micro emulsion delivery system. It is made up of lidocaine base 4% or 5% in a gel composed of water, ethanol, glycerin, jojoba oil, aloe vera oil, glyceryl monolaureate, benzyl alcohol, carbomer 940, and ethylenediamine tetraacetic acid (EDTA). Both formulations can be obtained without prescription.
Four percent topicaine is recommended for usage only on intact skin under occlusion. Five percent can be used with or without occlusion. As per manufacturer, topicaine produces effective analgesic effect when applied for 30–60 minutes prior to a procedure. The recommended maximum area of application in adults is less than 600 cm2 and in children it is less than 100 cm2.
Topicaine is being used extensively in the field of cosmetic dermatology. It is indicated for pain relief prior to procedures like electrolysis, waxing, laser hair removal, permanent make up, tattoos, collagen injections, botox injections, hair transplants, laser treatment of telengectiasis, and acid peels. The 5% formulation can also be used for anorectal pain relief.
Topicaine’s efficacy was tested in a randomized, double-blind, controlled trial with EMLA and LMX 5 after application for 30 minutes with laser-induced pain stimuli using Q-switched Nd: YAG laser at 1064 nm. Topicaine and LMX 5 produced effective anesthesia after a 30 minute application time. However, topicaine and EMLA seemed to produce the highest anesthetic effect 30 minutes after removal.
Local effects are mild, which include erythema, edema, and blanching. Topicaine’s usage is contraindicated in patients with amide sensitivity. More studies are needed to establish the efficacy, tolerability and safety profile of topicaine (CitationFriedman, Mafong, et al 2001b; CitationESBA 2005).
Iontophoresis
Iontophoresis is a method of enhancing the transport of topically applied drugs using a mild electric current to increase the permeability of charged drugs through the skin. This process is utilized for delivery of drugs like lidocaine, epinephrine, methylprednisolone succinate, dexamethasone phosphate, antivirals, and antibiotics (CitationGangarosa et al 1995). The drug to be delivered is placed at an electrode of the same polarity at or near the surface of the treatment area. The positively charged drug is placed at the anode and the negatively charged drug is placed at the cathode. A mild direct current is passed, which travels through the skin, through the interstitial fluids, and back to the skin, which is collected by a return electrode. The ions of the drug traverse through the same path as the current (CitationGangarosa et al 1995; CitationZimmer and Ashburn 2001). Iontophoresis was found to enhance the penetration of the drug by 20–60-fold when compared with topical application (CitationGangarosa et al 1995).
Lidocaine iontophoresis has been found to be 80% to 100% effective in providing anesthetic action prior to procedures like injections, abrasions, laser surgery, and cautery. This procedure was not found to be efficacious in providing enough anesthesia for dermal excisions, for procedures that involve more than 1cm, and for procedures done on hands and feet (CitationMaloney et al 1992).
With lidocaine iontophoresis, the onset of action is within 10 minutes. The onset of anesthetic effect was not decreased by increasing the concentration of lidociane (CitationOshima et al 1994), and the anesthetic effect lasted for 15 minutes (CitationKundu and Achar 2002). The depth of anesthesia was found to be 1–2 cm (CitationLener et al 1997). The plasma levels of lidocaine were < 1.0–1 μg/ml after 10 minutes of iontophoresis application. This did not change even when higher concentrations of lidocaine were used (CitationOshima et al 1994).
In dermatologic procedures, iontophoresis has been found to be a safe and an effective technique for topical anesthesia in both children and adults. It was found to be useful for performing procedures in children like shave biopsy, curettage, injection, punch biopsy (CitationZempsky and Parkinson 2003a). This was a multicenter, randomized, placebo-controlled, double-blind study in 60 children evaluating the efficacy and safety of lidocaine iontophoresis. Ninety-four percent in treatment reported no pain when compared with 7% of patients in the placebo group (p < 0.001). This is a good quality study and the results seem to be reliable. It was used in adults prior to performing shave biopsy (CitationZempsky and Parkinson 2003b). In this study, 41 patients were evaluated in a single center, randomized, double-blind, and placebo-controlled fashion. This is a very good study and the results seem to be reliable as 90% of patients in the treatment group reported no pain when compared with 10% of the patients in the placebo group (p < 0.001). In a comparative clinical study with EMLA, both provided effective and complete anesthesia, however the onset of anesthetic effect with iontophoresis had been much more rapid (within 30 minutes) (CitationGreenbaum and Bernstein 1994). It has also been shown to provide effective anesthesia prior to pulsed dye laser application of port wine stains (CitationNunez et al 1997).
Iontophoresis has also been found to provide rapid and effective anesthesia in various procedures. It has been found useful prior to lumbar puncture performed in emergency department (CitationStrout et al 2004). When compared with placebo both in children and adults prior to venous cannulation was found to provide safe and effective anesthesia (CitationMiller et al 2001; CitationZempsky et al 2004). This was again confirmed in another study when done in children alone (CitationRose et al 2002). In a comparative study with EMLA, iontophotesis was found to be inferior in efficacy but onset was much faster with iontophoresis (CitationSquire et al 2000; CitationMoppett et al 2004). Iontophoresis was also found efficacious for IV placement (CitationAshburn et al 1997; CitationZempsky et al 1998; CitationGalinkin et al 2002), radial artery cannulation (CitationSherwin et al 2003), and PIV in both children and adults.
The local effects upon using iontophoresis were transient erythema and edema, blanching, itching (CitationZempsky and Parkinson 2003b; CitationStrout et al 2004), burning, and tingling sensation. There has been no reported systemic toxicity so far. The blood levels of lidocaine were found to be below 10 ng/mL without any systemic reactions in a study which evaluated the tolerability and systemic bioavailability in pediatric population (CitationKearns et al 2003). In another independent study the plasma levels of lidocaine in children after an average of 20 minutes of iontophoresis with lidocaine was found to be > 1.0 μg/ml. Less than 1.5 μg/ml was supposed to be within the normal range (CitationSchultz et al 2002).
Synera™ (S-Caine Patch)
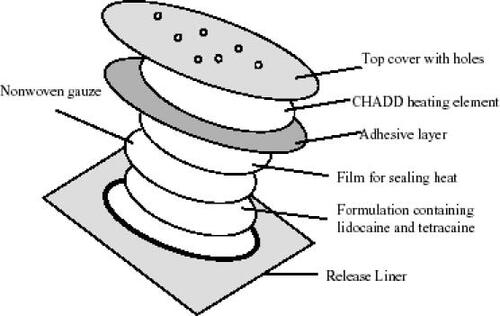
Synera™ is a novel patch system intended to deliver local anesthesia. This was originally developed under the name of S-Caine Patch by ZARS Pharma (Salt Lake City, UT, US), and was recently approved by FDA. It is now licenced to Endo Pharmaceuticals Inc (Chadds Ford, PA, USA). This is a lidocaine and tetracaine patch (L/T patch) built in with a heating element called CHADD (Controlled Heat-Assisted Drug Delivery), which is a disposable oxygen-activated system. The L/T patch without the CHADD system has been found to provide effective anesthetic effect for minor dermatology procedures in geriatric population (CitationSchecter 2005). The formulation is an emulsion in which the active ingredients are in oil phase as a eutectic mixture containing 70 mg of lidocaine and 70 mg of tetracaine in a ratio of 1:1 by weight. The inactive ingredients are polyvinyl alcohol, sorbitan monopalmitate, water, methylparaben, and propylparaben (Endo Pharmaceuticals Inc. Packet insert for Synera™). This system does not use any permeation enhancers. The total surface area of Synera patch is 50 cm2 out of which the active area is 10 cm2. Synera is indicated to be used on intact skin for providing local dermal anesthesia prior to superficial dermatological procedures and superficial venous access. It is not recommended for usage on mucous membranes (Endo Pharmaceuticals Inc. Packet insert for Synera™).
The CHADD patch uses a new technology that releases controlled heat to enhance the delivery of the drug. Heat is generated using a mixture of iron powder, activated carbon, sodium chloride, wood flour, and water (Endo Pharmaceuticals Inc. Packet insert for Synera™). This mixture is placed in a pouch made of filter paper. This is again sealed between 2 polymer films. One of the films has holes of precalculated size. Another membrane with tiny holes covers the heat generating chemical components. When this package is exposed to atmosphere, air flows through the holes present in the cover membrane at a controlled rate, into the heating mixture and initiates a chemical reaction that generates heat. The amount of heat generated and the duration of reaction depend on the number and size of the holes in the membrane, and the composition and amount of the chemicals in the pouch (See URL: http://www.zars.com/scainepatch.html).
The local anesthetics are packed in a shallow chamber below the CHADD patch and sealed in an airtight packet. When applied to the skin, the CHADD patch gets heated spontaneously and increases the temperature of the skin, thereby enhancing the permeation of the drugs through the epidermis (See URL: http://www.zars.com/scainepatch.html). This reduces the duration of onset of action of the local anesthetics. The heating element produces a temperature of 39°C to 41°C for 2 hours (CitationFriedman et al 2001a).
A picture of Synera patch is provided by ZARS on their website at http://www.zars.com/scainepatch.html ().
Figure 1 Illustration of Synera patch.
In a randomized, double-blind study, when Synera was compared with placebo, prior to minor dermatology procedures such as skin tag removal, superficial excision, electrodessication, keloid injection, and shave biopsies performed in adults, the patch proved to provide safe and effective anesthesia when applied for 30 minutes (CitationBerman et al 2005). In a similarly designed study conducted on 74 patients over the age of 65 years, Synera patch-treated patients had less pain than patients who received placebo (Endo Pharmaceuticals Inc. Packet insert for Synera™). The depth of anesthesia was found to be 6.8 mm with Synera and 4.7 mm with placebo. The anesthetic effect of the patch lasted for more than 120 minutes as opposed to 10 minutes with placebo. This was determined in a randomized, double-blind, placebo-controlled, two-period crossover trial involving 12 healthy adult volunteers between the ages of 18 and 50 years. (CitationShomaker et al 2000). It has also been found to be beneficial prior to venipuncture in children, adults, and the geriatric population. In an independent study among the pediatric population involving 64 children, in a randomized, double-blind, and placebo-controlled fashion, Synera was found to be safe and effective when applied for 20 minutes. The child’s pain was rated with the Oucher pain scale. Seventy-six percent of patients with this medication had less pain when compared with 20% of patients in the placebo group (p = 0.001) (CitationSethna et al 2005). This is a well balanced study with good sample size and results seem to be valid.
A 20 minute application of Synera patch showed less pain in three randomized, double-blind, placebo-controlled studies that were conducted among adults and the geriatric population to evaluate the degree of dermal analgesia prior to venipuncture. Pain was measured using 100 mm visual analog scale in all three studies. The first study (n = 21) showed median VAS scores of 1 and 9 for Synera and placebo treatments, respectively. The second study (n = 40) showed median VAS scores of 5 and 28 for Synera and placebo treatments, respectively. The third study (n = 21) showed median VAS scores of 1 and 9 for Synera and placebo treatments, respectively. The third study involved 40 subjects over the age of 65 years, and the median VAS scores for Synera and placebo treatments were 8 and 14, respectively. In another double-blind study conducted in 250 adult subjects, comparing Synera patch intact with heating element and without heating element, the median VAS scores with heating and without heating element were 17 and 22, respectively (Endo Pharmaceuticals Inc. Packet insert for Synera™).
The local effects reported were transient mild erythema, edema (CitationSethna et al 2005), blanching (Endo Pharmaceuticals Inc. Packet insert for Synera™), and burning sensation (CitationBerman et al 2005) resolving spontaneously soon after treatment. Contact with the eyes should be avoided as it may result in severe eye irritation based on animal studies (Endo Pharmaceuticals Inc. Packet insert for Synera™). There have been no reported systemic effects so far. In several studies conducted in both adults and children, either with a single or multiple Synera patches, the plasma levels of lidocaine and tetracaine were well below the toxic levels. Central nervous system toxicity may usually be seen at levels around 5000 ng/ml, though few patients may show signs of toxicity like excitation and or depression at plasma lidocaine levels of approximately 1000 ng/ml. In a study involving adults, the peak plasma levels of lidocaine were found to be less than 5 ng/ml, while levels of tetracaine were less than 0.9 ng/ml in all patients on application of one Synera patch for 30 minutes. When the duration of application was doubled to 60 minutes, there was no significant increase in plasma levels of both the agents. In children aged 4 months to 12 years, on application of one Synera patch for 30 min, the plasma levels of lidocaine and tetracaine were found to be 63 ng/ml and 65 ng/ml, respectively. Studies were also done to determine the plasma levels of lidocaine and tetracaine on simultaneous and sequential usage of multiple Synera patches in adults and children. Although these studies did not show the levels of either lidocaine or tetracaine to reach toxic levels, application of multiple Synera patches is not recommended. In a clinical pharmacology study, when two or four Synera patches were applied simultaneously for 60 minutes, the peak plasma concentration of lidocaine were less than 9 ng/ml, while that of tetracaine were undetectable. On sequential 30 minute application of four Synera patches at 60 minute intervals, the peak plasma concentrations of lidocaine were less than 12 ng/ml and that of tetracaine were less than the quantitation limit. When two Synera patches were applied for up to 30 minutes in children of ages 4 months and 12 years, the peak levels of lidocaine and tetracaine were 331 ng/ml and less than 5 ng/ml, respectively (Endo Pharmaceuticals Inc. Packet insert for Synera™). Based on the results of the above mentioned studies, the usage of Synera patch seems to be safe and without major side effects. The usage of this patch is not recommended during magnetic resonance imaging as the heating element contains iron powder (Endo Pharmaceuticals Inc. Packet insert for Synera™). The advantages of using Synera over other topical products are ease of application, heat induced enhancement of solubility of drugs and their permeation, no reactions with the vehicle components, and no necessity for occlusive dressings. (see URL: http://www.zars.com/scainepatch.html). Most of all, from the data in the above mentioned studies, Synera patch, when used as recommended by the manufacturer, seems to be very safe and efficacious in delivering dermal anesthesia. The technique of using thermal energy for enhancement of drug penetration may be applied for producing local anesthesia with other agents as well.
Dentipatch
Dentipatch is an oral transmucosal delivery system containing lidocaine. This was the first bioadhesive patch developed for delivering local anesthesia to oral mucosa. It was introduced in the US in 1996 and is FDA-approved for providing mild topical anesthesia of accessible mucous membranes of the mouth prior to superficial dental procedures (CitationMantele et al 2005). This patch can also find its use in dermatology prior to procedures involving oral mucosa.
The dentipatch contains a viscous mixture of lidocaine, lecithin, propylene glycol, dipropylene glycol, glycerin, karaya gum, aspartame, and spearmint flavor. This mixture is coated onto a backing containing a polyster/ethylene vinyl acetate (EVA) film laminated to a polyester/rayon nonwoven fabric at a predetermined thickness. This is then dried in ovens to accelerate gelling process. Once the gelling is completed, this is again laminated to the release liner. The current available product contains 46.1 mg of lidocaine which is 20 weight percent concentration in a bioadhesive matrix. It provides site-specific anesthetic effect where needed, when directly applied to the mucosa (CitationMantele et al 2005).
On application of the dentipatch for 15 minutes, anesthetic effect was found to be produced in 2.5 minutes, and the action lasted for 40 minutes after the removal of the patch. Two studies done to evaluate the efficacy of 10 and 20 weight percent lidocaine patches against placebo showed to provide effective anesthetic effect when tested with 25 gauge needle inserted unto bone. The plasma levels of lidocaine with 20 weight percent active patch at intervals of 15 and 45 minutes were found to be 9 times lesser than those achieved with injection of 2% lidocaine. Plasma levels of lidocaine with application of 5% lidocaine ointment were found to be at least double than those achieved with application of 20 weight percent of dentipatch for the same time period of 15 minutes. The most common local effect found was unpleasant taste. The other was minimal irritation (CitationHersh et al 1996; CitationMantele et al 2005).
Other patches
Other patches are also used for their systemic effects in the management of chronic pain states. One such patch is duragesic patch containing the opioid, fentanyl. This provides sustained analgesia around the clock. It finds application in the treatment of cancer and noncancer pain states. The lidoderm patch containing lidocaine 5% has been found to be useful in chronic pain states. It has been extensively studied and used for pain control in post-herpetic neuralgia. It has also been studied for pain control in osteoarthritis, myofascial pain, peripheral pain syndromes, chronic leg ulcers, allodynia, and erythromelalgia (CitationKatz et al 2002; CitationDavis 2003; CitationMeier et al 2003; CitationGammaitoni et al 2003, Citation2004; CitationDalpiaz et al 2004).
S-Caine peel
This is a novel and innovative method of delivering topical anesthesia, mostly is being tested in the field of cosmetic dermatology. This is a cream-based preparation, made up of eutectic mixture of lidocaine 7% and tetracaine 7%. The inactive ingredients in the formulation are polyvinyl alcohol, lecithin, corn starch, and water (CitationChen et al 2003). When applied to the skin, it dries on exposure to air, forming a flexible membrane that can be easily peeled off. The advantage is that anesthesia is easily delivered to contours of the body without needing any occlusion (see URL: http://www.zars.com/scainepatch.html). Its efficacy had been mostly tested for anesthesia that is necessary for laser procedures used in dermatology. A picture of S-Caine peel is provided by ZARS on their website at http://www.zars.com/scainepatch.html.
In comparative clinical studies with placebo, it has shown to provide effective anesthesia, and the time of onset was between 30 to 60 minutes. The level of anesthetic action needed depended on the specific type of lasers, such as pulsed dye laser, nonablative laser, and long-pulsed Nd: YAG laser, used for specific procedures (CitationBryan and Alster 2002; CitationDoshi et al 2003; CitationJih et al 2004). The more the numbing effect is needed, the more time the peel should be left behind.
In a randomized, double-blind, placebo-controlled study involving 60 patients in three centers, S-Caine peel was found to provide safe and effective anesthesia in 20 to 30 minutes of applicaton prior to treatment of portwine stains and facial telengectiasis using pulsed dye laser. Fifty-two percent of patients had VAS scores for pain as 10 mm and 72.2% of patients had VAS scores as 20 mm being on the active drug. The investigators and independent observer rated no pain in 75% and 72% of patients on the active drug, respectively. The high level of efficacy found in this study should be confirmed by further clinical evaluation (CitationBryan and Alster 2002). For treatment of leg veins using long-pulsed Nd: YAG laser treatment, S-Caine peel provided safe and highly effective anesthesia when applied for 60 minutes (CitationJih et al 2004). This was evaluated in a study involving 60 patients which was a randomized, double-blind, placebo-controlled study conducted at 2 centers (p < 0.001). In a multicentered, randomized, double-blind, placebo-controlled study conducted in 30 adult patients, who underwent laser-assisted tattoo removal, 70% of patients, S-Caine peel was found to have pain reduction when applied for 60 minutes (CitationChen et al 2005).
Local side effects thus far reported included transient mild erythema (CitationBryan and Alster 2002; CitationDoshi et al 2003; CitationChen et al 2005). This interesting new invention seems to have advantages over classical topical anesthetics, in that it can be easily applied and removed, and the anesthetic effect generated depends on the duration of the peel left behind. More information pertaining to plasma levels of the active agents attained and potential side effects, if any, would be expected to be available once S-Caine peel is approved by the FDA.
Summary
summarizes the various modes of penetration enhancements of the drugs discussed in this review.
Table 1 Modes of penetration enhancement
Conclusion
Among the current available products, EMLA and LMX have been widely tested and are popular in clinical practice. With the invention of smaller and portable instruments, iontophoresis has considerable potential to regain its popularity. Synera patch, which was recently FDA-approved, would likely find more application because of its ease of usage, especially in the pediatric population. In the immediate future, S-Caine peel has potential to become popular in cosmetic dermatology procedures.
There has been significant research over the past decade in understanding the skin permeation mechanisms. The outcome of research in this area so far is reflected on the advances we are now seeing in the development of formulations and devices that optimize drug delivery, either by passive or active means, necessary for local and or systemic effects. More products in the form of patches with novel polymers for constructing the backing membranes and adhesives, peels, and vesicles as drug carriers are likely to be the mode of drug delivery through the skin in future.
References
- AlkanMGefenZGolcmanLWound infection after simple suture at the emergency wardInfection Control1984556246569855
- AltieriMBogemaSSchwartzRHTAC topical anesthesia produces positive urine tests for cocaineAnn Emerg Med19901957792184707
- AltmanDAGildenbergSRHigh-energy pulsed light source hair removal device used to evaluate the onset of action of a new topical anestheticDermatol Surg1999258161810594586
- AndersonABColecchiCBaronoskiRLocal anesthesia in pediatric patients: topical TAC versus lidocaineAnn Emerg Med199019519222184706
- Arendt-NeilsenLBjerringPNielsenJRegional variations in analgesic efficacy of EMLA cream. Quantitatively evaluated by argon laser stimulationActa Derm Venereol199070314181977256
- Arendt-NielsenLBjerringPLaser-induced pain for evaluation of local analgesiaAnesth Analg198867115233341564
- ArevaloMIEscribanoECalpenaARapid skin anesthesia using a new topical amethocaine formulation: a preclinical studyAnesth Analg20049814071215105222
- AshburnMAGauthierMLoveGIontophoretic administration of 2% lidocaine HCl and 1:100,000 epinephrine in humansClin J Pain1997132269084949
- AshinoffRGeronemusRGEffect of the topical anesthetic EMLA on the efficacy of pulsed dye laser treatment of port-wine stainsJ Dermatol Surg Oncol1990161008112246405
- AstraZeneca Pharmaceuticals, USARev 05/05. EMLA full prescription information [online]2004 Accessed on 20 Aug 2005. URL: http://www.astrazeneca-us.com/pi/EMLA.pdf
- BarkerWRodeheaverGTEdgertonMTDamage to tissue defenses by a topical anesthetic agentAnn Emerg Med198211307107081792
- BarryBWJohnsonPLloyd-JonesJGTransdermal drug delivery systems fundamentals and techniques1987Chichester, UKEllis Horwood Publishers200223
- BergerLFreud: Darkness in the Midst of Vision2000New York, NYJohn Wiley &Sons, Inc.639
- BermanBFloresJPariserDSelf-warming lidocaine/tetracaine patch effectively and safely induces local anesthesia during minor dermatologic proceduresDermatol Surg200531135815762203
- BernardiMSeccoFBenechAAnesthetic efficacy of an eutectic mixture of lidocaine and prilocaine (EMLA) on the oral mucosa: prospective double-blind study with a placeboMinerva Stomatol199948394310356950
- BjerringPAndersenPHArendt-NielsenLVascular response of human skin after analgesia with EMLA creamBr J Anaesth198963655602532919
- BjerringPArendt-NielsenLDepth and duration of skin analgesia to needle insertion after topical application of EMLA creamBr J Anaesth19906417372317421
- BlackburnPAButlerKHHughesMJComparison of tetracaine-adrenaline-cocaine (TAC) with topical lidocaineepinephrine (TLE): efficacy and costAm J Emerg Med199513315177755827
- BlankeWHallernBVSharp wound debridement in local anaesthesia using EMLA cream: 6 years’ experience in 1084 patientsEur J Emerg Med2003102293112972901
- BonadioWAWagnerVEfficacy of TAC topical anesthetic for repair of pediatric lacerationsAm J Dis Child1988a14220353277392
- BonadioWAWagnerVHalf-strength TAC topical anesthetic. For selected dermal lacerationsClin Pediatr (Phila)1988b2749583168386
- BonadioWAWagnerVWhen TAC drips into the eyeAm J Emerg Med199083712363764
- BrahmaAKInksterCAlkaline chemical ocular injury from EMLA creamEye1995965898543097
- BrismanMLjungBMOtterbomIMethaemoglobin formation after the use of EMLA cream in term neonatesActa Paediatr199887119149846923
- BronaughRLMiabachHIPercutaneous absorption1985New York, NYMarcel Dekker
- BryanHAAlsterTSThe S-Caine peel: a novel topical anesthetic for cutaneous laser surgeryDermatol Surg200228999100312460292
- BucaloBDMirikitaniEJMoyRLComparison of skin anesthetic effect of liposomal lidocaine, nonliposomal lidocaine, and EMLA using 30-minute application timeDermatol Surg199824537419598008
- Bucks DanielAWMaibachHIBronaughRLMaibachHIOcclusion does not uniformly enhance penetration in vivoTopical absorption of dermatological products2002New York, NYDekker932
- CannonCRChouteauSHutchinsonKTopically applied tetracaine, adrenalin, and cocaine in the repair of traumatic wounds of the head and neckOtolaryngol Head Neck Surg19891007892493622
- ChenJZAlexiades-ArmenakasMRBernsteinLJTwo randomized, double-blind, placebo-controlled studies evaluating the S-Caine Peel for the induction of local aneshesia before long-pulsed Nd: YAG laser therapy for leg veinsDermatol Surg20032910121812974697
- ChenJZJacobsonLGBakusADEvaluation of the S-Caine Peel for induction of local anesthesia for laser-assisted tattoo removal: randomized, double-blind, placebo-controlled, multicenter studyDermatol Surg200531281615841627
- ChienYWNovel drug systems1982New York, NYDekker149
- ClearyGWLangerRSWiseDLTransdermal controlled-release systemsMedical applications of controlled release1984Boca RatonCRC Press, Inc.203251
- CovinoBGPharmacology of local anaesthetic agentsBr J Anaesth198658701162425835
- DaileyRHFatality secondary to misuse of TAC solutionAnn Emerg Med198821591603337432
- DalpiazASLordonSPLipmanAGTopical lidocaine patch therapy for myofascial painJ Pain Palliat Care Pharmacother200418153415364629
- DavisMDLidocaine patch helpful in managing the chronic pain of leg ulcerationJ Am Acad Dermatol20034996414576697
- DoshiSNFriedmanPMMarquezDKThirty-minute application of the S-Caine peel prior to nonablative laser treatmentDermatol Surg20032910081112974696
- DykeVCByckRCocaineSci Am1982246128417043731
- EaglsteinFNChemical injury to the eye from EMLA cream during erbium laser resurfacingDermatol Surg199925590110469121
- EichenfieldLFFunkAFallon-FriedlanderSA clinical study to evaluate the efficacy of ELA-Max (4% liposomal lidocaine) as compared with eutectic mixture of local anesthetics cream for pain reduction of venipuncture in childrenPediatrics20021091093912042548
- EngbergGDanielsonKHennebergSPlasma concentrations of prilocaine and lidocaine and methaemoglobin formation in infants after epicutaneous application of a 5% lidocaine-prilocaine (EMLA)Acta Anaesthesiol Scand19873162483687359
- EremiaSNewmanNTopical anesthesia for laser hair removal: comparison of spot sizes and 755 nm versus 800 nm wavelengthsDermatol Surg200026667910886276
- ErnstAAMarvezENickTGLidocaine adrenaline tetracaine gel versus tetracaine adrenaline cocaine gel for topical anesthesia in linear scalp and facial lacerations in children aged 5 to 17 yearsPediatrics1995a9525587838644
- ErnstAAMarvezENickTGLidocaine adrenaline tetracaine gel versus tetracaine adrenaline cocaine gel for topical anesthesia in linear scalp and facial lacerations in children aged 5 to 17 yearsAm J Emerg Med1995b1315147893297
- [ESBA] ESBA LaboratoriesInformation on Topicaine gel [online]2005Jupiter, FL, USAESBA Laboratories Accessed on 15 Aug 2005 URL: http://www.topicaine.com/
- EversHVon DardelOJuhlinLDermal effects of compositions based on the eutectic mixture of lignocaine and prilocaine (EMLA)Br J Anaesth19855799710054041328
- FaulconorAJrKeysTEFoundations of anesthesiology1965Springfield, ILCC Thomas771
- FinkBRLeaves and needles: the introduction of surgical local anesthesiaAnesthesiology19856377833893227
- FinkelJCYangCIYarvitzJLNeuroselective sensory electrodiagnostic evaluation of 4% liposomal topical lidocaineAnesth Analg20029412596211973201
- FlynnGLBankerGSRhodesCTTopical drug absorption and topical pharmaceutical systemsModern pharmaceutics1979New York, NYDekker263
- FriedmanPMMafongEAFriedmanESTopical Anesthetics Update: EMLA and BeyondDermatologic Surgery2001a2710192611849263
- FriedmanPMFogelmanJLevineVComparative study of three topical anesthetics after 30 minutes application timeCosmetic Surgery Times2001
- FriedmanPMFogelmanJPNouriKComparative study of the efficacy of four topical anestheticsDermatol Surg199925950410594629
- FriedmanPMMafongEAFriedmanESTopical anesthetics update: EMLA and beyondDermatol Surg2001b2710192611849263
- GalinkinJLRoseJBHarrisKLidocaine iontophoresis versus eutectic mixture of local anesthetics (EMLA) for IV placement in childrenAnesth Analg2002941484812032012
- GalvinJRDe SimoneDInfection rate of simple suturingJ Am Coil Emerg Physicians19765332333
- GammaitoniARAlvarezNAGalerBSSafety and tolerability of the lidocaine patch 5%, a targeted peripheral analgesic: a review of the literatureJ Clin Pharmacol2003431111712616661
- GammaitoniARGalerBSOnawolaRLidocaine patch 5% and its positive impact on pain qualities in osteoarthritis: results of a pilot 2-week, open-label study using the Neuropathic Pain ScaleCurr Med Res Opin200420Suppl 2S131915563742
- GangarosaLP SrOzawaAOhkidoMIontophoresis for enhancing penetration of dermatologic and antiviral drugsJ Dermatol199522865758557860
- GoodacreTESandersRWattsDASplit skin grafting using topical local anaesthesia (EMLA): a comparison with infiltrated anaesthesiaBr J Plast Surg19884153383052675
- GosnoldJKInfection rate of sutured woundsPractitioner19772185845859805
- GrantSAHoffmanRSUse of tetracaine, epinephrine, and cocaine as a topical anesthetic in the emergency departmentAnn Emerg Med199221987971497171
- GreenbaumSSBernsteinEFComparison of iontophoresis of lidocaine with a eutectic mixture of lidocaine and prilocaine (EMLA) for topically administered local anesthesiaJ Dermatol Surg Oncol199420579838089357
- GuardianoRANorwoodCWDirect comparison of EMLA versus lidocaine for pain control in Nd:YAG 1,064 nm laser hair removalDermatol Surg200531396815871313
- GuptaAKSibbaldRGEutectic lidocaine/prilocaine 5% cream and patch may provide satisfactory analgesia for excisional biopsy or curettage with electrosurgery of cutaneous lesions. A randomized, controlled, parallel group studyJ Am Acad Dermatol199635419238784280
- GuyRHHadgraftJPharmacokinetics of percutaneous absorption and concurrent metabolismInt J Pharm19842043
- HallenBOlssonGLUppfeldtAPain-free venepuncture. Effect of timing of application of local anaesthetic creamAnaesthesia198439969726496911
- HegenbarthMAAltieriMFHawkWHComparison of topical tetracaine, adrenaline, and cocaine anesthesia with lidocaine infiltration for repair of lacerations in childrenAnn Emerg Med1990196372297157
- HershEVHouptMICooperSAFeldmanRSAnalgesic efficacy and safety of an intraoral lidocaine patchJ Am Dent Assoc19961271626348952239
- HiguchiTRocheBPro-drug, molecular structure and percutaneous deliveryDesign of biopharmaceutical properties through pro-drugs and analogs1977Washington, DCAPA409121
- HjorthNHarringMHahnAEpilation of upper lip hirsutism with a eutectic mixture of lidocaine and prilocaine used as a topical anestheticJ Am Acad Dermatol199125809111802904
- HolmJAndrenBGraffordKPain control in the surgical debridement of leg ulcers by the use of a topical lidocaine—prilocaine cream, EMLAActa Derm Venereol19907013261969197
- HolmesHSChoosing a local anestheticDermatol Clin19941281727805311
- HolmesMVDaweRSFergusonJA randomized, double-blind, placebo-controlled study of the efficacy of tetracaine gel (Ametop) for pain relief during topical photodynamic therapyBr J Dermatol20041503374014996106
- HolstRGKristoffersonALidocaine-prilocaine cream (EMLA Cream) as a topical anaesthetic for the cleansing of leg ulcers. The effect of length of application timeEur J Dermatol1998824579649697
- HuangWVidimosATopical anesthetics in dermatologyJ Am Acad Dermatol2000432869810906653
- IdsonBRabinowitz MyersonRMPercutaneous absorption in topics in medicinal chemistryAbsorption phenomena19764New York, NYWiley-Interscience181
- IsmailFGoldsmithPCEmla cream-induced allergic contact dermatitis in a child with thalassaemia majorContact Dermatitis20055211115725295
- JacobsenSErrors in emergency practiceEmerg Med198719109
- JainARutterNRatnayakaMTopical amethocaine gel for pain relief of heel prick blood sampling: a randomised double-blind controlled trialArch Dis Child Fetal Neonatal Ed200184F56911124928
- JainARutterNDoes topical amethocaine gel reduce the pain of venepuncture in newborn infants? A randomised double-blind controlled trialArch Dis Child Fetal Neonatal Ed200083F2071011040170
- JihMHFriedmanPMSadickN60-minute application of S-Caine Peel prior to 1,064 nm long-pulsed Nd:YAG laser treatment of leg veinsLasers Surg Med2004344465015216539
- JuhlinLEversHEMLA: A New Topical AnestheticAdv Dermatol1990575912204380
- JuhlinLEversHBrobergFAlidocaine-prilocaine cream for superficial skin surgery and painful lesionsActa Derm Venereo1980605446
- JuhlinLHagglundGEversHAbsorption of lidocaine and prilocaine after application of a eutectic mixture of local anesthetics (EMLA) on normal and diseased skinActa Derm Venereol19896918222563603
- JuhlinLRollmanOVascular effects of a local anesthetic mixture in atopic dermatitisActa Derm Venereol198464439406208728
- KapelushnikJKorenGSolhHEvaluating the efficacy of EMLA in alleviating pain associated with lumbar puncture; comparison of open and double-blinded protocols in childrenPain1990423142234995
- KatzMAriensEJDesign of topical drug product: pharmaceuticsDrug design19734New York, NYAcad Pr.93148
- KatzMPoulsenBJBrodieBBGilletteJAbsorption of drugs through the skinHandbook of experimental pharmacology1971New York, NYSpringer-Verlag28 103
- KatzNPGammaitoniARDavisMWLidoderm Patch Study Group. Lidocaine patch 5% reduces pain intensity and interference with quality of life in patients with postherpetic neuralgia: an effectiveness trialPain Med200233243215099237
- KatzNPShapiroDEHerrmannTERapid onset of cutaneous anesthesia with EML A cream after pretreatment with a new ultrasound–emitting deviceAnesth Analg200498371614742372
- KearnsGLHeacookJDalySJPercutaneous lidocaine administration via a new iontophoresis system in children: tolerability and absence of systemic bioavailabilityPediatrics20031125788212949287
- KleiberCSorensonMWhitesideKTopical anesthetics for intravenous insertion in children: a randomized equivalency studyPediatrics20021107586112359791
- KohJLHarrisonDMyersRA randomized, double-blind comparison study of EMLA and ELA-Max for topical anesthesia in children undergoing intravenous insertionPaediatr Anaesth2004149778215601345
- KopeckyEAJacobsonSBchMBSafety and pharmacokinetics of EMLA in the treatment of postburn pruritus in pediatric patients: a pilot studyJ Burn Care Rehabil2001222354211403247
- KoppelRAColemanKMColemanWPThe efficacy of EMLA versus ELA–Max for pain relief in medium–depth chemical peeling: a clinical and histopathologic evaluationDermatol Surg20002661410632688
- KunduSAcharSPrinciples of office anesthesia: part II. Topical anesthesiaAm Fam Physician2002669910212126037
- KurienLKollbergHUppfeldtAVenepuncture pain can be reducedJ Trop Med Hyg19858839793837123
- LahteenmakiTLillieborgSOhlsenLTopical analgesia for the cutting of split-skin grafts: a multicenter comparison of two doses of a lidocaine/prilocaine creamPlast Reconstr Surg198882458623043487
- LarssonBANormanMBjerringPRegional variations in skin perfusion and skin thickness may contribute to varying efficacy of topical, local anaesthetics in neonatesPaediatr Anaesth19966107108846274
- LawsonRASmartNGGudgeonACEvaluation of an amethocaine gel preparation for percutaneous analgesia before venous cannulation in childrenBr J Anaesth19957528257547043
- LenerEVBucaloBDKistDATopical anesthetic agents in dermatologic surgeryDermatol Surg199723673839256914
- LiuDRKirchnerHLPetrackEMDoes using heat with eutectic mixture of local anesthetic cream shorten analgesic onset time? A randomized, placebo-controlled trialAnn Emerg Med200342273312827120
- LokCPaulCAmblardPEMLA cream as a topical anesthetic for the repeated mechanical debridement of venous leg ulcers: a double-blind, placebo-controlled studyJ Am Acad Dermatol1999402081310025747
- LongCPMcCaffertyDFSittlingtonNMRandomized trial of novel tetracaine patch to provide local anaesthesia in neonates undergoing venepunctureBr J Anaesth200492450114970141
- LuhmannJHurtSShootmanMA comparison of buffered lidocaine versus ELA-Max before peripheral intravenous catheter insertions in childrenPediatrics2004113e2172014993579
- LyckaBAMedical indications for using a topical anestheticPerspect Pain Manage19911912
- LyckaBAEMLA. A new and effective topical anestheticJ Dermatol Surg Oncol199218859621430539
- MaloneyJMBezzantJLStephenRLIontophoretic administration of lidocaine anesthesia in office practice: An appraisalJ Dermatol Surg Oncol199218937401430549
- ManteleJALuckingDKaniosDPGoshTKPfisterWROral transmucosal systems for Local anesthetics: dental and oral surgical premedicationDrug delivery to the oral cavity molecules to market2005Boca Raton, FLCRC Pr.233259
- MartyJPGuyRHMaibachHIBronaughRLMaibachHIPercutaneous penetration as a method of delivery to muscle and other tissuesPercutaneous absorption1985New York, NYMarcel Dekker
- MazumdarBTomlinsonAAFaulderGCPreliminary study to assay plasma amethocaine concentrations after topical application of a new local anaesthetic cream containing amethocaineBr J Anaesth19916743261931400
- McCaffertyDFWoolfsonADNew patch delivery system for percutaneous local anesthesiaBr J Anaesth19937137048398517
- McCaffertyDFWoolfsonADBostonVIn vivo assessment of percutaneous local anaesthetic preparationsBr J Anaesth19896217212644962
- McCaffertyDFWoolfsonADHandleyJEffect of percutaneous local anaesthetics on pain reduction during pulse dye laser treatment of portwine stainsBr J Anaesth19977828699135307
- McKinlayJRHofmeisterERossEVEMLA cream-induced eye injuryArch Dermatol1999135855610411170
- MeierTWasnerGFaustMEfficacy of lidocaine patch 5% in the treatment of focal peripheral neuropathic pain syndromes: a randomized, double-blind, placebo-controlled studyPain2003106151814581122
- MillerKABalakrishnanGEichbauerG1% lidocaine injection, EMLA cream, or “numby stuff” for topical analgesia associated with peripheral intravenous cannulationAANA J200169185711759560
- MollerCA lignocaine-prilocaine cream reduces venipuncture painUps J Med Sci19859029383913095
- MolodeckaJStenhouseCJonesJMComparison of percutaneous anaesthesia for venous cannulation after topical application of either amethocaine or EMLA creamBr J Anaesth19947217468110569
- MooreJNo more tears: a randomized controlled double-blind trial of Amethocaine gel vs. placebo in the management of procedural pain in neonatesJ Adv Nurs2001344758211380714
- MoppettIKSzypulaKYeomanPMComparison of EMLA and lidocaine iontophoresis for cannulation analgesiaEur J Anaesthesiol200421210315055894
- NicholsFCIIIMuchaPJrFarnellMBTAC topical anesthetic and minor skin lacerationsResident and Staff Physician1987335966
- NunezMMirallesESBoixedaPIontophoresis for anesthesia during pulsed dye laser treatment of port-wine stainsPediatr Dermatol1997143974009336816
- O’ConnorBTomlinsonAAEvaluation of the efficacy and safety of amethocaine gel applied topically before venous cannulation in adultsBr J Anaesth19957470687640129
- OldaySJWalpoleRWangJYRadial artery cannulation: topical amethocaine gel versus lidocaine infiltrationBr J Anaesth200288580212066736
- OrdogGJOrdogCThe efficacy of TAC (tetracaine, adrenaline, and cocaine) with various wound-application durationsAcad Emerg Med1994136037614282
- OshimaTKashikiKToyookaHCutaneous iontophoretic application of condensed lidocaineCan J Anaesth19944167797923514
- PoulsenBJAriensEJDesign of topical drug products: biopharmaceuticsDrug design19734New York, NYAcad Pr.149192
- PryorGJKilpatrickWROppDRLocal anesthesia in minor lacerations: topical TAC vs lidocaine infiltrationAnn Emerg Med19809568717436066
- Ramos-ZabalaAPerez-MenciaMTFernandez-GarciaRAnesthesia technique for outpatient facial laser resurfacingLasers Surg Med2004342697215022256
- RanadeVVHollinger MannfredATransdermal drug deliveryDrug delivery systems20032Boca Raton, FLCRC Pr.20740
- RinconEBakerRLIglesiasAJCNS toxicity after topical application of EMLA cream on a toddler with molluscum contagiosumPediatr Emerg Care200016252410966344
- RitchieJMGreeneNMGoodmanAGRallTWNiesASLocal anestheticsThe pharmacologic basis of therapeutics19808New York, NYPergamon Pr.31129
- RosdahlIEdmarBGisslenHCurettage of molluscum contagiosum in children: analgesia by topical application of a lidocaine/prilocaine cream (EMLA)Acta Derm Venereol198868149532453995
- RoseJBGalinkinJLJantzenECA study of lidocaine iontophoresis for pediatric venipunctureAnesth Analg2002948677111916787
- RosenthalDMurphyFGottschalkRUsing a topical anaesthetic cream to reduce pain during sharp debridement of chronic leg ulcersJ Wound Care200110503512964231
- RussellSCDoyleEA risk-benefit assessment of topical percutaneous local anaesthetics in childrenDrug Saf199716279879113495
- RutherfordWHSpenceRAJInfection in wounds sutured in the accident and emergency departmentAnn Emerg Med1980935026994527
- RylanderESjobergILillieborgSLocal anesthesia of the genital mucosa with a lidocaine/prilocaine cream (EMLA) for laser treatment of condylomata acuminata: a placebo-controlled studyObstet Gynecol19907530262405326
- SarifakiogluNTerziogluACigsarBEMLA and ear surgery: is it possible to achieve full-thickness anesthesia with EMLA?Dermatol Surg200430395815008868
- SchaeferHZeschAStuttgenGSkin permabilityHeidelberg: Springer-Verlag19826047
- SchafferDJClinical comparison of TAC anesthetic solutions with and without cocaineAnn Emerg Med1985141077804051273
- SchecterAKRandomized, double-blind, placebo-controlled study evaluating the lidocaine/tetracaine patch for induction of local anesthesia prior to minor dermatologic procedures in geriatric patientsDermatol Surg200531287915841628
- SchillingCGBankDEBorchertBATetracaine, epinephrine (adrenalin), and cocaine (TAC) versus lidocaine, epinephrine, and tetracaine (LET) for anesthesia of lacerations in childrenAnn Emerg Med19952520387832348
- SchultzAAStroutTDJordanPSafety, tolerability, and efficacy of iontophoresis with lidocaine for dermal anesthesia in ED pediatric patientsJ Emerg Nurs2002282899612122400
- SchupleinRJJarretAThe skin as a barrier, skin permeation, site variation in diffusion and permeabilityPhysiology and pathophysiology of the skin1978New York, NYAcad Pr.1693731
- SethnaNFVergheseSTHannallahRSA randomized controlled trial to evaluate S-Caine Patch for reducing pain associated with vascular access in childrenAnesthesiology2005102403815681958
- ShelleyWBThe razor blade in dermatologic practiceCutis1975168434
- SherwinJAwadITSadlerPJAnalgesia during radial artery cannulation: comparison of the effects of lidocaine applied by local injection or iontophoresisAnaesthesia200358474612751506
- SherwoodKAThe use of topical anesthesia in removal of port-wine stains in childrenJ Pediatr1993122S3640
- ShomakerTSZhangJLoveGEvaluating skin anesthesia after administration of a local anesthetic system consisting of an S-Caine Patch and a controlled heat-aided drug delivery (CHADD) patch in volunteersClin J Pain200016200411014392
- SmithDPGjellumMThe efficacy of LMX versus EMLA for pain relief in boys undergoing office meatotomyJ Urol20041721760115371808
- SmithGAStrausbaughSDHarbeck-WeberCComparison of topical anesthetics without cocaine to tetracaine-adrenaline-cocaine and lidocaine infiltration during repair of lacerations: bupivacainenorepinephrine is an effective new topical anesthetic agentPediatrics19969730178604261
- SmithGAStrausbaughSDHarbeck-WeberCNew non-cocaine-containing topical anesthetics compared with tetracaine-adrenaline-cocaine during repair of lacerationsPediatrics1997100825309346982
- SmithSMBarryRCA comparison of three formulations of TAC (tetracaine, adrenalin, cocaine) for anesthesia of minor lacerations in childrenPediatr Emerg Care19906266702290723
- SquireSJKirchhoffKTHissongKComparing two methods of topical anesthesia used before intravenous cannulation in pediatric patientsPediatr Health Care2000146872
- StroutTDSchultzAABaumannMRReducing pain in ED patients during lumbar puncture: the efficacy and feasibility of iontophoresis, collaborative approachJ Emerg Nurs2004304233015452520
- StymneBLillieborgSPlasma concentrations of lignocaine and prilocaine after a 24-h application of analgesic cream (EMLA) to leg ulcersBr J Dermatol2001145530411703277
- TanOTStaffordTJEMLA for laser treatment of portwine stains in childrenLaser Surg Med1992125438
- TerndrupTEWallsHCMarianiPJPlasma cocaine and tetracaine levels following application of topical anesthesia in childrenAnn Emerg Med19922116261739203
- TiptonGADe WittGWEisensteinSJTopical TAC (tetracaine, adrenaline, cocaine) solution for local anesthesia in children: prescribing inconsistency and acute toxicitySouth Med J198982134462814620
- TranNQPrettoJJWorsnopCJA randomized controlled trial of the effectiveness of topical amethocaine in reducing pain during arterial punctureChest200212213576012377864
- VinciRJFishSSEfficacy of topical anesthesia in childrenArch Pediatr Adolesc Med199615046698620226
- WahlgrenCFQuidingHDepth of cutaneous analgesia after application of a eutectic mixture of the local anesthetics lidocaine and prilocaine (EMLA cream)J Am Acad Dermatol200042584810727302
- WatonJBoulangerATrechotPHContact urticaria from Emla creamContact Dermatitis200451284715606654
- WatsonKAstra markets cream to remove pain of injectionsPharm J1986236262
- WehleBBjornstromMCedgardMRepeated application of EMLA cream 5% for the alleviation of cannulation pain in haemodialysisScand J Urol Nephrol1989232993022595326
- WehnerDHamiltonGCSeizures following topical application of local anesthetics to burn patientsAnn Emerg Med19841345686731962
- WhiteWBIsersonKVCrissETopical anesthesia for laceration repair: tetracaine versus TAC (tetracaine, adrenaline, and cocaine)Am J Emerg Med19864319223718621
- WoodfordRBarryBWPenetration enhancers and the percutaneous absorption of drugs: an updateJ Toxicol Cut Ocular Toxicol1986516777
- YunPLTachiharaRAndersonRREfficacy of erbium:yttrium-aluminum-garnet laser-assisted delivery of topical anestheticJ Am Acad Dermatol200247542712271298
- ZARSInformation on S-Caine Peel [online]2005 Accessed on 20 Jul 2005. URL: http://www.zars.com/scainepeel.htmlZARS, UT, USA.
- ZARSInformation on Synera [online]2005 Accessed on 20 Jul 2005 URL: http://www.zars.com/scainepatch.html ZARS, UT, USA
- ZempskyWTAnandKJSullivanKMLidocaine iontophoresis for topical anesthesia before intravenous line placement in childrenJ Pediatr1998132106139627608
- ZempskyWTParkinsonTMLidocaine iontophoresis for topical anesthesia before dermatologic procedures in children: a randomized controlled trialPediatr Dermatol2003a20364812869165
- ZempskyWTParkinsonTMLidocaine iontophoresis for local anesthesia before shave biopsyDermatol Surg2003b296273012786707
- ZempskyWTSullivanJPaulsonDMEvaluation of a low-dose lidocaine iontophoresis system for topical anesthesia in adults and children: a randomized, controlled trialClin Ther20042611101915336476
- ZimmerRAshburnMANoninvasive drug deliveryCompr Ther20012729330111765687