Abstract
Insulin resistance, hyperglycemia, hyperinsulinemia, hyperlipidemia and oxidative stress are risk factors related to cardiovascular diseases including congestive heart failure, myocardial infarction, ventricular hypertrophy, endothelial nitric oxide impairment in systemic blood vessels and the heart, atherosclerosis, and hypercoagulability of blood. The traditional focus on insulin sensitivity and blood levels of markers of risk determined in the fasted state is inconsistent with the large volume of recent data that indicates that the metabolic defect in the pre-diabetic and diabetic condition relates more strongly to postprandial deficiency than to the fasting state. Risk factors for adverse cardiovascular events can be detected in the pre-diabetic insulin-resistant subject based upon the metabolic response to a test meal even in the absence of altered fasting parameters. The normal response to a mixed meal includes a doubling of insulin action secondary to insulin-induced release of a putative hepatic insulin sensitizing substance (HISS) that acts selectively on skeletal muscle. HISS is released only in the fed state and accounts for meal-induced insulin sensitization. Blockade of HISS release leads to a condition referred to as HISS-dependent insulin resistance, which is suggested as the primary postprandial metabolic defect, accounting for postprandial hyperglycemia, hyperinsulinemia, hyperlipidemia, and increased oxidative stress in the pre-diabetic and diabetic condition. HISS-dependent insulin resistance represents a novel hypothesis and suggests a new diagnostic and therapeutic target.
Early diagnosis of diabetes was done by the diagnostician tasting the copious volumes of urine produced by their patients. This diagnostic approach led to a severe underestimation of the incidence of diabetes. Modern diagnosticians depend almost entirely upon determinations of fasting plasma levels of glucose and, less frequently, insulin. This approach also leads to a severe underestimation of the metabolic dysfunction that is typical of the type 2 diabetic. A state of insulin resistance is recognized to occur well prior to the development of diabetes. The pre-diabetic state of insulin resistance can be diagnosed by determining the response to a test meal. The theme of this brief review is that the metabolic dysfunction in the pre-diabetic state is quantifiable and represents a major risk factor for the development of cardiovascular disease. Postprandial hyperglycemia, hyperinsulinemia, hyperlipidemia, and oxidative stress are individually and collectively recognizable risk factors. An abnormal meal-induced insulin sensitization (AMIS) is proposed as a novel hypothesis to account for the pre-diabetic state of insulin resistance which, if uncorrected, progresses to diabetes when the pancreatic insulin release is no longer able to compensate for AMIS. In this review, I suggest that the “HISS story” may explain the mechanism of AMIS and affords new approaches to diagnosis and treatment of pre-diabetic and diabetic insulin resistance.
Postprandial hyperglycemia
In 1997 the American Diabetes Association (ADA) introduced the term “impaired fasting glucose” to describe individuals whose fasting plasma glucose concentration was between 110 to 125 mg/dl (CitationADA 1997). Since this diagnostic category was proposed, questions have been raised as to its clinical utility and it has been suggested that impaired glucose tolerance is a better predictor of both type 2 diabetes and cardiovascular disease (CitationDECODE Study Group 2001, Citation2003). In an effort to respond to these concerns, the ADA has recently proposed that the glucose level used to identify individuals with impaired fasting glucose be lowered from 110 to 100 mg/dl (CitationADA 2003). Recent studies to evaluate the modified standard have indicated a 4-fold increase in individuals considered to have impaired fasting glucose following the new criteria. Serious questions related to the clinical and public health implications of this new impaired fasting glucose definition have been raised (CitationFord et al 2005).
The current approach of screening for type 2 diabetes using the fasted metabolic status, while convenient, is not effective. In a recent review evaluating the status of screening for type 2 diabetes, CitationEngelgau et al (2000) stated that one of the criteria for appropriate screening is that the tests should detect the preclinical stage of disease and that the tests be shown to be acceptable and reliable. The conclusion that current screening recommendations are not consistent with available evidence was briefly reviewed. Evidence is accumulating that most people with a 54–67% range of impaired glucose tolerance have fasting glucose in the normal range. Meta-analysis of 20 different European studies showed as many as 31% of those who were diabetic according to post-challenge plasma glucose had normal fasting values and therefore would not have been detected by a screening procedure based upon fasting glucose measurements alone.
The majority of studies and diagnosis continue to focus on the fasted state. However, the importance of postprandial rather than fasting metabolic defects, as related to cardiovascular disease, is becoming increasingly recognized. The relationship between HbA1c and plasma glucose in patients with type 2 diabetes was determined at four time points during the day and HbA1c levels were found to be significantly predicted by plasma glucose levels measured only at post-lunch and extended post-lunch (5 hours) time points (CitationAvignon et al 1997). The strongest age- and sex-adjusted relative risk for all-cause and cardiovascular mortality were associated with 2 hour post-load plasma glucose levels (Citationde Vegt et al 1999). Increased mortality risk has been associated with 2 hour post-load plasma glucose levels to a much greater extent than with fasting plasma glucose (CitationHanefeld et al 1996; CitationDECODE Study Group 1999). Isolated post-load hyperglycemia is a strong predictor of mortality (CitationSimon et al 1987; CitationDECODE Study Group 1999; CitationShaw et al 1999; CitationVaccaro et al 1999; CitationEngelgau et al 2000; CitationSimon and Brandenberger 2002).
It has been suggested that hyperglycemia-induced overproduction of superoxide by the mitochondrial electron transport chain accounts for the four main molecular mechanisms implicated in glucose-mediated vascular damage associated with blindness, renal failure, nerve damage, atherosclerosis, stroke, and hindlimb amputation (CitationBrownlee 2001). Postprandial plasma glucose is an important determinant of both onset and development of nephropathy in type 2 diabetic patients (CitationSchchiri et al 2000). Low density lipoprotein oxidation increases after meals (CitationDiwadkar et al 1999) and directly relates to the degree of hyperglycemia (CitationCeriello et al 1999). Acute hyperglycemia is associated with an acute increase in clotting factor VII (CitationCeriello et al 1988) and enhanced thrombin activity that was proportional to the level of hyperglycemia (CitationCeriello et al 1996). The synthesis of fibrinogen, which is a strong risk factor for cardiovascular disease in both diabetic and non-diabetic subjects, increases during food intake in diabetic patients (CitationCeriello 1997; CitationBruttomesso et al 2001).
Acute hyperglycemia also stimulates increased expression of proadhesive proteins including ICAM-1 (CitationCeriello 2003). CitationDunn and Grant (2005) reviewed the relationship between the hypercoagulable prothrombic state that occurs in type 2 diabetes and cardiovascular disease risk. Hypertriglyceridemia and hyperglycemia have been shown to have an independent and cumulative effect on postprandial production of nitrotyrosine and adhesion molecules (CitationCeriello et al 2004).
In a review of the importance of postprandial hyperglycemia on the development of cardiovascular disease, CitationHaffner (1998) suggested that atherosclerotic changes start to develop in the pre-diabetic state when postprandial blood glucose levels are only moderately elevated above normal levels. He suggested, however, that increased insulin resistance and hyperinsulinemia may be responsible for the atherosclerotic changes and that hyperglycemia may be a marker but not a cause of these changes.
Postprandial lipidemia
The hypothesis that atherogenesis is a postprandial phenomenon (CitationZilversmit 1979) was largely ignored until fairly recently when re-emphasis on the acute response to test meals demonstrated a clear superiority in predicting cardiovascular risk factors. An oral glucose tolerance test resulted in hyperglycemia and similar cardiovascular responses in both healthy and diabetic subjects. However, the use of the more physiological mixed meal test revealed myocardial endothelial dysfunction in the diabetic subjects. Myocardial blood flow, which was similar in fasted diabetic and healthy subjects, increased significantly in response to a standardized mixed meal in the control subjects but decreased significantly in the diabetic patients (CitationScognamiglio et al 2005). The superiority of a mixed meal versus the oral glucose tolerance test, related to cardiac dysfunction, was proposed to relate to the postprandial hypertriglyceridemia which only occurred using the test meal (CitationScognamiglio et al 2005). A negative influence of postprandial hypertriglyceridemia on endothelial function has been reported in diabetic subjects (CitationBae et al 2001; CitationAnderson et al 2001). Postprandial hypertriglyceridemia is a recognized independent predictor of cardiovascular pathology (CitationAnderson et al 2001).
Postprandial dyslipidemia is prevalent in diabetic patients even with normal fasting triglyceride concentrations (CitationMero et al 1998). Insulin resistance causes increased flux of free fatty acids and thus enhanced VLDL synthesis in the liver. Postprandial hypertriglyceridemia contributes to the metabolic disturbances transforming lipoprotein subclasses into more atherogenic forms.
Healthy, male, first-degree relatives of patients with type 2 diabetes have insulin resistance and postprandial hypertriglyceridemia despite having normal fasting triglyceride levels (CitationAxelsen et al 1999). Newly diagnosed hypertensive patients with hypertriglyceridemia were more insulin resistant and showed greater postprandial hypertriglyceridemia than hypertensive patients not showing elevated fasting levels of triglycerides (CitationHwu et al 2002). Atherosclerosis is an inflammatory disorder involving leukocytes. The postprandial triglyceride increment after a fat meal was paralleled by a leukocyte increment due to an increase in neutrophils in the first two postprandial hours (Citationvan Oostrom et al 2003). It has even been suggested that the cardiovascular risk recognized to occur with chronic smokers is related to insulin resistance and postprandial dyslipidemia that is not mirrored by fasting hypertriglyceridemia (CitationEliasson et al 1997). The recognized impact of various nutritional supplements or beverages, including tea, in lowering the incidence of cardiovascular disease may be related to the demonstration of attenuation of the postprandial increase in plasma triglyceride levels following a fat load (CitationUnno et al 2005).
Postprandial hyperinsulinemia
Impaired glucose metabolism was demonstrated to be a predictor of development of congestive heart failure in a large community-based sample of elderly men (CitationIngelsson et al 2005). Surprisingly, when insulin sensitivity and the impaired glucose tolerance were analyzed as co-variates, obesity was no longer a significant predictor of the subsequent development of congestive heart failure. This suggests that obesity may be a coincidental predictor of congestive heart failure and may simply be a marker of insulin resistance, which is compensated for by hyperinsulinemia.
CitationIngelsson et al (2005) suggest that the hyperinsulinemia associated with impaired glucose metabolism represents a risk factor through several possible mechanisms. Insulin acts as a growth factor in the myocardium as shown by increased myocardial mass and decreased cardiac output in rats exposed to sustained hyperinsulinemia (Holmang et al 1996). Hyperinsulinemia leads to sodium retention (CitationDeFronzo et al 1975) which may exacerbate subclinical myocardial dysfunction due to blood volume expansion. Hyperinsulinemia leads to sympathetic nervous system activation (CitationAnderson et al 1991) which is a presumed causal factor for congestive heart failure (CitationKannel and Belanger 1991; CitationBell 2003). Insulin resistance is related to increased effectiveness of angiotensin II on blood pressure (CitationGaboury et al 1994) and cellular hypertrophy and collagen production (CitationSartori et al 2004) in individuals with hypertension, leading to myocardial hypertrophy and fibrosis (CitationBell 2003) and likely subsequent congestive heart failure.
The relationship between elevated insulin levels and heart disease remains controversial mainly because it is often not clear exactly what is being measured by insulin assays. Using an assay specific for insulin and proinsulin, CitationZethelius et al (2005) suggested that proinsulin levels rather than insulin levels were a better predictor of development of coronary heart disease in a study of older Swedish males. The literature supporting proinsulin levels as a better marker than insulin suggests a unique biological role for proinsulin and could also be interpreted to indicate that the fasting levels of proinsulin are not representative of postprandial responses, rather that the slow metabolic degradation of proinsulin may lead to greater fasting levels of proinsulin and thus reflect postprandial hyperinsulinemia.
CitationSomogyi et al (2005) studied hyperglycemia-induced oxidative stress using the rat streptozotocin model. The diabetic rats not treated with insulin showed enhanced activity of antioxidant enzymes. Diabetic rats treated with insulin showed decreased total oxidant scavenger capacity and development of left ventricular hypertrophy. They suggested that increased activity of the antioxidant enzymes inhibits subcellular remodeling processes thereby inhibiting cardiac hypertrophy, whereas insulin decreases the activity of the antioxidant system and can enhance the function of other localized tissue-specific growth factors. Chronic hyperinsulinemia may contribute to pathologies related to unregulated growth stimulation.
Postprandial oxidative stress
CitationCeriello (2000) has suggested that increased postprandial oxidative stress may be the common pathway through which the majority of diabetic complications occur. As previously discussed, both hyperglycemia and hyperlipidemia lead to increased oxidative stress. Meal consumption in healthy subjects has been shown to acutely reduce antioxidant defenses (CitationCeriello et al 1998) and produces an oxidative stress (CitationCeriello et al 1998; CitationUrsini et al 1998). Oxidative stress is linked to the pathogenesis of cardiovascular disease (CitationGriendling and Alexander 1997) and hypertension (CitationNakazono et al 1991). Antioxidants produce vasodilation in patients with hypertension and coronary artery disease (CitationCeriello et al 1991; CitationLevine et al 1996; CitationSolzbach et al 1997). This is consistent with evidence that free radical production accompanies endothelial dysfunction (CitationGriendling and Alexander 1997) and that antioxidants improve endothelial dysfunction (CitationAnderson et al 1995). Ceriello, recognizing the strong relationship between processing a meal and the production of oxidative stress, concluded that “…paradoxically, the vast majority of the studies on cardiovascular disease risk factors have been conducted by measuring them in strictly fasting conditions. This simply means that most of the data available to date may not reflect the real situation” (CitationCeriello 2000, p128).
It has been suggested that nitric oxide is inactivated by excess superoxide production in the postprandial state in both healthy and diabetic subjects and that the subsequent impaired vascular reactivity can be predicted based upon the circulating level of nitrotyrosine (CitationCeriello 2002). Vitamin E and other antioxidants administered to diabetics increase tissue antioxidant levels, improve the action of insulin, promote endothelial function, prevent oxidation of serum lipids, suppress protein glycation and reduce the oxidative load (CitationRosen et al 1995). Drugs that have significant antioxidant activity may improve the risk factors for cardiovascular disease through the sequestration of superoxide, thereby reducing the nitric oxide-dependent cardiovascular and metabolic dysfunctions.
CitationWhiteside (2005) reviewed the literature on vascular complications of diabetes and reactive oxygen species, concluding that attention must be directed to more effective antioxidants as few clinical trials indicate a major therapeutic benefit from current monotherapy approaches. A recent study of ours strongly supports this conclusion. Insulin resistance produced in response to the chemical hepatotoxin, thioacetamide, can be prevented from developing by the use of an antioxidant cocktail consisting of vitamin E, vitamin C, and S-adenosylmethionine, but not the individual components of the cocktail (CitationMing et al 2006). The insulin resistance produced by thioacetamide was shown to be represented by HISS-dependent insulin resistance with direct (HISS-independent) insulin action remaining unaltered (HISS and HISS-dependent insulin resistance are discussed later). The use of an antioxidant cocktail designed to protect multiple sites may offer a more rational approach to antioxidant therapy.
Cardiovascular disease
Insulin resistance in type 2 diabetics is associated with increased prevalence of coronary heart disease, blood coagulability, and dislipidemia leading to the suggestion that reducing insulin resistance in diabetics may reduce their tendency to develop thrombosis and hence coronary heart disease risk (CitationWannamethee et al 2004). In post-myocardial infarction patients, the metabolic syndrome and diabetes were prevalent and associated with increased risk of cardiovascular events and death (CitationLevantesi et al 2005). Impaired glucose regulation has been related to left ventricular systolic (CitationArnlov et al 2001) and diastolic (CitationArnlov et al 2005) dysfunction and left ventricular remodeling (CitationDevereux et al 2000; CitationSundstrom et al 2000; CitationRutter et al 2003). The exaggerated cardiac damage in response to acute ischemia/reperfusion injury induced by repetitive hyperglycemia was prevented by co-administration of acarbose (CitationFrantz et al 2005).
Chronic inflammatory diseases such as rheumatoid arthritis (CitationDessein et al 2005), polycystic ovarian syndrome (CitationDokras et al 2005; CitationKravariti et al 2005), and obesity (CitationKarelis et al 2005) represent a high risk factor for development of insulin resistance. Primary renal disease is associated with postprandial hypertriglyceridemia (CitationCharlesworth et al 2005). C reactive protein has recently been demonstrated to be associated with high incidence of insulin resistance (CitationFesta et al 2000; CitationLee et al 2004; CitationRutter et al 2004) and cardiovascular disease (CitationKoenig et al 2004; CitationPai et al 2004) and is also elevated in the above chronic inflammatory disease conditions. Low grade systemic inflammation, identified by elevated C reactive protein, is present in normal weight subjects who show insulin resistance but no other metabolic abnormalities (CitationBo et al 2005). Testing for high sensitivity C reactive protein has recently (CitationPearson et al 2003) been recommended by the American Heart Association for the assessment of the risk for developing cardiovascular disease (CitationRifai 2005). Although one study suggests that the association between C reactive protein and the metabolic syndrome disappears after adjustment for fitness level (CitationLamonte et al 2005).
Postprandial nutrient processing and the HISS hypothesis
We have recently demonstrated (CitationLautt et al 2001) that the glucose disposal effect of a bolus of insulin is approximately doubled in the early postprandial state and this meal-induced insulin sensitization (MIS) progressively decreases to a baseline level of insulin sensitivity after 24 hours of fasting. As a brief overview, the MIS process is proposed to occur as a result of insulin acting on the liver to release a hepatic insulin sensitizing substance (HISS) that acts selectively on skeletal muscle to stimulate glucose uptake. HISS action thus accounts for the large postprandial glucose sequestration in skeletal muscle (CitationXie and Lautt 1996a, Citation1996b; CitationMoore et al 2002). The HISS hypothesis further proposes that blockade of HISS release results in postprandial hyperglycemia, which leads to postprandial compensatory hyperinsulinemia, with the increased insulin acting primarily on the liver and adipose tissue and resulting in increased formation of triglycerides and VLDL as well as increased free radical production (i.e. the metabolic syndrome). The sequence of discoveries leading to the current status of the HISS hypothesis is reviewed (CitationLautt 2004) as are methods to evaluate HISS-dependent and HISS-independent insulin action (CitationLautt 2003).
Methods used to quantitate the MIS process rely on an index of insulin sensitivity determined before and after administration of a mixed test meal. Although the original discovery of the dependence of whole body insulin action on hepatic nerves was made in cats using a standard insulin tolerance test (CitationXie et al 1993), the problems associated with the hypoglycemia that ensues following a bolus of insulin led us to develop the rapid insulin sensitivity test (RIST). The RIST is simply a rapidly sampled transient euglycemic clamp (CitationLautt et al 1998) and has been used in cats, mice, rats, pigs, and humans and with a wide range of physiological and pathophysiological models (for review see CitationLautt 2003). The RIST and the insulin tolerance test are equally able to detect HISS action and different insulin effectiveness in the fed versus fasted state (CitationReid et al 2002). The RIST is highly reproducible and can be repeated several times consecutively in the same animal.
Abnormal insulin delivery, such as produced by a single large bolus of 300 mU/kg, results in an inability of subsequent normal doses of insulin to cause HISS release. This would appear to be protective in nature. Further, when insulin is administered as pulses, subsequent insulin action is demonstrated to be unaffected whereas administration of the same dose of insulin by constant infusion results in an impairment of HISS release in subsequent tests with the degree of impairment related to the duration of the constant infusion (CitationReid and Lautt 2004). Similar endocrine dependence on pulsatile stimulation is seen with the gonadotropins, which, when delivered in pulses results in testosterone secretion but when delivered in the same dose but at a constant rate results in chemical castration (CitationBelchetz et al 1978). In our hands, the 3-hour hyperinsulinemic euglycemic clamp utilizing continuous insulin infusion was not capable of determining differences in insulin sensitivity before and after a meal except for an increased response in the fed state within the first 30 minutes of infusion (CitationReid et al 2002). Others (CitationZsuga et al 2004) however have studied aspects related to HISS and have found similar results using a prolonged clamp or the RIST. Studies in the conscious dog (CitationMoore et al 2002) were able to detect significant HISS-like responses using a prolonged clamp. HISS release is dependent on hepatic parasympathetic tone. Cardiovascular parasympathetic dysfunction is associated with diabetes and is detectable at the pre-diabetic stage of insulin resistance (CitationLautt 1999). A 90 minute hyperinsulinemic euglycemic clamp resulted in a decrease in cardiac parasympathetic tone and an increase in sympathetic nerve activity in skeletal muscle (CitationVan de Borne et al 1999) suggesting that the prolonged, constant-infusion euglycemic clamp may not be the most appropriate index of insulin sensitivity under conditions, such as diabetes and obesity, where normal parasympathetic tone is important. Use of the euglycemic clamp also resulted in elevated levels of cytokines, beta amyloid and norepinephrine in cerebrospinal fluid (CitationFishel et al 2005). It is crucial that any methods used to study MIS, and the postprandial defect we refer to as HISS-dependent insulin resistance (HDIR), must be able to quantify insulin effect in the fed and fasted state.
HISS release can be acutely blocked by surgical parasympathetic denervation of the liver which results in decreased postprandial insulin sensitivity that is indistinguishable from that measured in the fasted state. Further, after hepatic denervation, mimicking the hepatic parasympathetic permissive signal through intraportal venous infusion of acetylcholine does not result in a direct impact on glycemia but the restored parasympathetic signal allows insulin to cause HISS release. Both the defect in insulin response subsequent to hepatic denervation and its restoration subsequent to intraportal but not intravenous acetylcholine has been demonstrated to occur in skeletal muscle (CitationXie and Lautt 1996a, Citation1996b; CitationMoore et al 2002).
The ability of surgical denervation of the liver to result in a selective inhibition of skeletal muscle response to glucose could suggest either a neural or hormonal link between the liver and skeletal muscle. However, the observation that restoration of the parasympathetic permissive signal can be achieved by intraportal but not intravenous continuous administration of acetylcholine proves the hormonal nature of the regulatory process. It is important to indicate that the parasympathetic signal in the liver is “permissive” in nature as demonstrated by the observation that the intraportal acetylcholine infusion does not result in an alteration of baseline glycemia but does allow insulin to have a restored effect in skeletal muscle. Similar studies have been done related to the hepatic parasympathetic requirement for sequential activation of hepatic muscarinic receptors and nitric oxide production. CitationSadri and Lautt (1999) reported that nitric oxide synthase antagonists were much more effective at blocking HISS release than were intravenous doses. Similarly, in the presence of blockade of hepatic nitric oxide synthase, the permissive parasympathetic signal could be restored by intraportal but not intravenous administration of nitric oxide donors. CitationGuarino et al (2004) demonstrated that the sequence of parasympathetic nerve activation involves sequential muscarinic and secondary nitric oxide synthase activation as demonstrated by the ability of a nitric oxide donor to reverse atropine-induced HISS-dependent insulin resistance and the inability of intraportal acetylcholine to reverse HISS-dependent insulin resistance produced by prior blockade of hepatic nitric oxide synthase.
Cats (CitationXie and Lautt 1995), rats (CitationLautt et al 2001), and dogs (CitationMoore et al 2002) that have been fasted for 16 hours continue to show a small HISS-dependent component of insulin action of approximately 25%–35%. The HISS-independent component (direct insulin action) is not altered by feeding or fasting nor is it altered by administration of atropine or hepatic denervation or blockade of hepatic nitric oxide (CitationLautt et al 2001). The HISS-dependent component of insulin action represents approximately 55% of the glucose disposal action of boluses of insulin over a wide range of insulin doses, from a barely detectable stimulation of glucose uptake induced by 5 mU/kg up to 100 mU/kg.
HISS-dependent insulin resistance (HDIR) accounts for the insulin resistance seen in a wide range of animal models including the spontaneously hypertensive rat, sucrose-fed rats, animals with liver disease induced by chronic bile duct ligation or chemical toxins, adult offspring of fetal alcohol exposure, acute stress and ageing, physical interruption of hepatic parasympathetic nerves, and pharmacological blockade of hepatic muscarinic cholinergic receptors, nitric oxide production or cyclooxygenase (reviewed CitationLautt 2003).
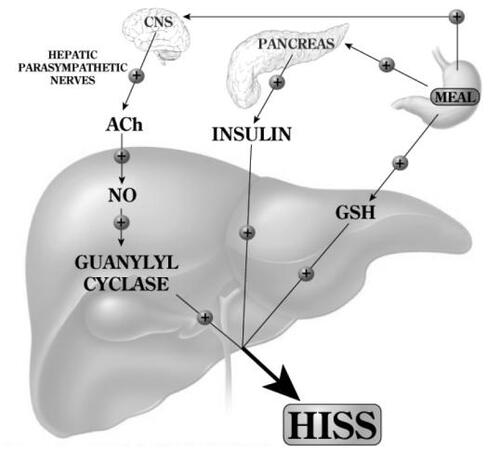
The permissive feeding signal (), delivered to the liver through the parasympathetic nerves acts via muscarinic receptor activation and generation of hepatic nitric oxide which then results in the insulin dose-related release of HISS (CitationSadri and Lautt 1999; CitationGuarino et al 2003). The nitric oxide acts through hepatic guanylyl cyclase (CitationCorreia et al 2002; CitationGuarino et al 2004). Hepatic glutathione level, which decreases significantly with fasting and rapidly increases following re-feeding is also an essential component of the feeding response in rats (CitationGuarino et al 2003; CitationLautt et al 2005; CitationSadri et al 2006). The mechanism of regulation of hepatic glutathione in response to feeding is unknown.
Figure 1 Feeding results in an increase of hepatic glutathione (GSH) and a parasympathetic signal to the liver that acts, via acetylcholine, on muscarinic receptors to activate NO release which, in turn, activates adenylyl cyclase. Both of these signals are permissive and both are needed in order that insulin can cause the release of hepatic insulin sensitizing substance (HISS). HISS acts selectively on skeletal muscle. Blockade of any portion of these pathways leads to blockade of HISS release and a state of HISS-dependent insulin resistance which is physiologically regulated to occur in the fasted state but, when not activated by feeding, is suggested to account for postprandial hyperglycemia, hyperinsulinemia, hyperlipidemia, and increased oxidative stress.
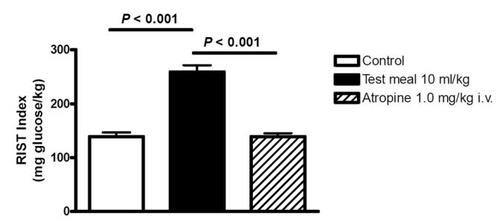
In a recent study we utilized a liquid test meal administered through a gastric catheter to quantitate MIS in both conscious and anesthetized rats by determining insulin sensitivity before and after the meal (CitationSadri et al 2006). A mixed liquid test meal, but not sucrose or glucose, resulted in MIS that could be completely reversed by atropine administration (). The insulin sensitivity index increased in response to feeding and was reversed completely back to fasting levels of sensitivity by atropine. Similarly, prior denervation of the liver completely prevented the MIS process from occurring, thereby confirming the central role of hepatic parasympathetic nerves in the feeding signal. MIS has also recently been shown to occur in healthy male volunteers and blockade of MIS has been confirmed to occur in humans subsequent to atropine administration (CitationPatarrao et al 2005).
Figure 2 The RIST index (mg glucose/kg body weight required to maintain euglycemia after a bolus of 50 mU/kg of insulin) increased 90 minutes after administration of a mixed liquid test meal via an indwelling gastric catheter in conscious unrestrained rats. Atropine (1 mg/kg), which blocks release of hepatic insulin sensitizing substance (HISS), completely eliminated the meal-induced insulin sensitization (MIS). The same report showed that sucrose or glucose were ineffective in activating MIS. Prior surgical denervation of the liver blocked MIS from developing (CitationSadri et al 2006).
Therapeutic potential
The HISS hypothesis is suggested to account for meal-induced insulin sensitization. Absence of HISS action, or HISS-dependent insulin resistance (HDIR), is suggested to account for the major postprandial metabolic dysfunctions seen in the pre-diabetic insulin resistant state. The conclusions reached in many of the studies referred to previously suggest that therapeutic intervention should be focused on correction of the postprandial insulin resistance. In a recent review evaluating new drug targets for type 2 diabetes and the metabolic syndrome, CitationMoller (2001 p821) emphasized that current therapies for type 2 diabetes were developed in the absence of defined molecular targets or an understanding of disease pathogenesis: “These therapies have limited efficacy, limited tolerability, and significant mechanism-based side effects. Of particular concern is the tendency for most treatments to enhance weigh gain. Several current approaches are also associated with episodes of hypoglycemia, and few of the available therapies adequately address underlying defects such as obesity and/or insulin resistance.” He further concluded that “Thus, newer approaches are desperately needed. Particular emphasis should be placed on finding and using mechanisms that are dependent on physiological responses and that result in weight loss.” With the recent understanding of the physiology and pathology related to HISS, targeting of this mechanism offers a novel approach to restoring normal postprandial physiological insulin sensitivity in skeletal muscle, the major site where the insulin resistance is generally acknowledged to occur in many insulin resistant states.
Conclusion
Postprandial hyperglycemia, hyperinsulinemia, hyperlipidemia and increased oxidative stress are strongly related to cardiovascular disease. Meal-induced insulin sensitization (MIS) normally occurs in response to a mixed meal, and absence of MIS is based on inability of the liver to secrete HISS in response to insulin. The argument has been made that HDIR could account for the primary endocrine defect in the pre-diabetic and diabetic state. Absence of MIS results in altered postprandial nutrient processing away from skeletal muscle and toward lipid production by liver and fat cells. These are all hypotheses that should be tested in the clinical setting.
The absence of MIS in response to glucose or sucrose “meals” in rats has major implications for interpretation of a large body of research, based on the oral glucose tolerance test, if confirmed in humans.
Although we advocate the use of the rapid insulin sensitivity test, any method used to evaluate the mechanisms and consequence of abnormal meal-induced insulin sensitization must clearly demonstrate a difference in insulin effect in the fed and fasted state.
HDIR is suggested to occur in association with a wide range of chronic inflammatory states and to contribute negatively as a strong risk factor for development of diabetes, obesity, cardiac and vascular disease, and asthma. If the “HISS story” is fundamentally correct, it represents a new paradigm impacting diagnosis and therapy of a broad spectrum of metabolic disorders.
Acknowledgements
The HISS-related work of the author cited here has been supported by operating grants from the Canadian Institutes of Health Research and the Canadian Diabetes Association. The HISS-related studies were carried out mainly by graduate students, technologists and trainees in the laboratories of Lautt (Winnipeg, Canada) and Macedo (Lisbon, Portugal). Manuscript preparation was by Karen Sanders. The author discloses that intellectual property related to diagnosis, prevention, and therapy of HISS-dependent insulin resistance has been licensed by the University of Manitoba to DiaMedica Inc.
References
- [ADA] ADA Expert Committee on the Diagnosis and Classification of Diabetes MellitusReport of the Expert Committee on the diagnosis and classification of diabetes mellitusDiabetes Care1997201183979203460
- [ADA] ADA Expert Committee on the Diagnosis and Classification of Diabetes MellitusReport of the Expert Committee on the diagnosis and classification of diabetes mellitusDiabetes Care200326S52012502614
- AndersonRAEvansMLEllisGRThe relationship between post-prandial lipeemia, endothelial function and oxidative stress in healthy individuals and patients with type 2 diabetesAtherosclerosis20011544758311166782
- AndersonEAHoffmanRPBalonTWHyperinsulinemia produces both sympathetic neural activation and vasodilation in normal humansJ Clin Invest1991872246522040704
- AndersonTJMeredithITYeungACThe effect of cholesterol-lowering and antioxidant therapy on endothelial-dependent coronary vasomotionN Engl J Med1995332488937830729
- ArnlovJLindLZetheliusBSeveral factors associated with the insulin resistance syndrome are predictors of left ventricular systolic dysfunction in a male population after 20 years of follow-upAm Heart J2001142720411579365
- ArnlovJLindLSundstromJInsulin resistance, dietary fat intake and blood pressure predict left ventricular diastolic dysfunction 20 years laterNutr Metab Cardiovasc Dis200515242916054547
- AvignonARadauccanuAMonnierLNonfasting plasma glucose is a better marker of diabetic control than fasting plasma glucose in type 2 diabetesDiabetes Care199720182269405900
- AxelsenMSmithUErikssonJWPostprandial hypertriglyceridemia and insulin resistance in normoglycemic first-degree relatives of patients with type 2 diabetesAnn Intern Med1999131273110391812
- BaeJHBassengeEKimKBPostprandial hypertriglyceridemia impairs endothelial function by enhanced oxidant stressAtherosclerosis20011555172311254924
- BelchetzPEPlantTMNakaiYHypophysial responses to continuous and intermittent delivery of hypothalamic gonadotropin-releasing hormoneScience19782026313100883
- BellDSHeart failure: the frequent, forgotten, and often fatal complication of diabetesDiabetes Care20032624334112882875
- BoSGambinoRUbertiBDoes C-reactive protein identify a subclinical metabolic disease in healthy subjects?Eur J Clin Invest2005352657015816996
- BrownleeMBiochemistry and molecular cell biology of diabetic complicationsNature20014148131911742414
- BruttomessoDIoriEKiwanukaEInsulin infusion normalizes fasting and post-prandial albumin and fibrinogen synthesis in type 1 diabetes mellitusDiabet Med2001189152011703437
- CerielloAFibrinogen and diabetes mellitus. Is it time for intervention trials?Diabetologia19974073149222655
- CerielloAThe post-prandial state and cardiovascular disease: relevance to diabetes mellitusDiabetes Metab Res Rev2000161253210751752
- CerielloANitrotyrosine: new findings as a marker of postprandial oxidative stressInt J Clin Pract Suppl200212951812166608
- CerielloAThe possible role of postprandial hyperglycaemia in the pathogenesis of diabetic complicationsDiabetologia200346M91612652353
- CerielloABortolottiNMotzEMeal-induced oxidative stress and low-density lipoprotein (LDL) oxidation in diabetes: the possible role of hyperglycemiaMetabolism1999481503810599980
- CerielloABortolottiNMotzEMeal-generated oxidative stress in type 2 diabetic patientsDiabetes Care1998211529339727904
- CerielloAGiuglianoDQuatraroAAnti-oxidants show an anti-hypertensive effect in diabetic and hypertensive subjectsClin Sci (Colch)199181739421662579
- CerielloAGiuglianoDQuatraroABlood glucose may condition factor VII levels in diabetic and normal subjectsDiabetologia198831889913240844
- CerielloATabogaCTonuttiLPost-meal coagulation activation in diabetes mellitus: the effect of AcarboseDiabetologia199639469738777997
- CerielloAQuagliaroLPiconiLEffect of postprandial hypertriglyceridemia and hyperglycemia on circulating adhesion molecules and oxidative stress generation and the possible role of simvastatin treatmentDiabetes2004537011014988255
- CharlesworthJAKriketosADJonesJEInsulin resistance and postprandial triglyceride levels in primary renal diseaseMetab Clin Exp200554821815931621
- CorreiaNCGuarinoMPPaposoJHepatic guanylyl cyclase inhibition induces HISS-dependent insulin resistanceProc West Pharmacol Soc20024557812434528
- DECODE Study Group on behalf of the European Diabetes Epidemiology GroupGlucose tolerance and mortality comparison of WHO and American Diabetes Association diagnostic criteriaLancet19993546172110466661
- DECODE Study Group the European Diabetes Epidemiology GroupGlucose tolerance and cardiovascular mortality: comparison of fasting and 2-hour diagnostic criteriaArch Intern Med200116139740411176766
- DECODE Study Group the European Diabetes Epidemiology GroupIs the current definition for diabetes relevant to mortality risk form all causes and cardiovascular and noncardiovascular disease?Diabetes Care2003266889612610023
- DeFronzoRACookeCRAndresRThe effect of insulin on renal handling of sodium, potassium, calcium, and phosphate in manJ Clin Invest197555845551120786
- DesseinPHJoffeBIStanwixAEEditorial: Should we evaluate insulin sensitivity in rheumatoid arthritis?Sem Arth Rheum20053557
- De VegtFDekkerJMRuheHGHyperglycaemia is associated with all-cause and cardiovascular mortality in the Hoorn population: the Hoorn studyDiabetologia1999429263110491751
- DevereuxRBRomanMJParanicasMImpact of diabetes on cardiac structure and function: the strong heart studyCirculation20001012271610811594
- DiwadkarVAAndersonJWBridgesSRPostprandial low density lipoproteins in type 2 diabetes are oxidized more extensively than fasting diabetes and control samplesProc Soc Exp Biol Med19992221788410564543
- DokrasABochnerMHollinrakeEScreening women with polycystic ovary syndrome for metabolic syndromeObstet Gynecol2005106131715994628
- DunnEJGrantPJType 2 diabetes: an atherothrombotic syndromeCurr Molec Med200553233215892651
- EliassonBMeroNTaskinenM-RThe insulin resistance syndrome and postprandial lipid intolerance in smokersAtherosclerosis199712979889069521
- EngelgauMMNarayanKMVHermanWHScreening for type 2 diabetesDiabetes Care20002315638011023153
- FestaAD’AgostinoRJrHowardGChronic subclinical inflammation as part of the insulin resistance syndrome: the Insulin Resistance Atherosclerosis Study (IRAS)Circulation200010242710880413
- FishelMAWatsonSMontineTJHyperinsulinemia provokes synchronous increases in central inflammation and β-amyloid in normal adultsArch Neurol20056215394416216936
- FordESAbbasiFReavenGMPrevalence of insulin resistance and the metabolic syndrome with alternative definitions of impaired fasting glucoseAtherosclerosis2005181143815939066
- FrantzSCalvilloLTillmannsJRepetitive postprandial hyperglycemia increases cardiac ischemia/reperfusion injury: prevention by the α-glucosidase inhibitor acarboseFASEB J200519591315671153
- GabouryCLSimonsonDCSeelyEWRelation of pressor responsiveness to angiotensin II and insulin resistance in hypertensionJ Clin Invest19949422953007989585
- GriendlingKKAlexanderRWOxidative stress and cardiovascular diseaseCirculation199796326459396412
- GuarinoMPAfonsoRARaimundoNHepatic glutathione and nitric oxide are critical for hepatic insulin-sensitizing substance actionAm J Physiol Gastrointest Liver Physiol2003284G5889412466146
- GuarinoMPCorreiaNCLauttWWInsulin sensitivity is mediated by the activation of the Ach/NO/cGMP pathway in rat liverAm J Physiol Gastrointest Liver Physiol2004287G5273215331351
- HaffnerSMThe importance of hyperglycemia in the nonfasting state to the development of cardiovascular diseaseEndocrine Rev199819583929793758
- HanefeldMFischerSJuliusURisk factors for myocardial infarction and death in newly detected NIDDM: the Diabetes Intervention Study, 11-year follow-upDiabetologia1996391577838960845
- HolmanyAYoshidaNJennischeEThe effects of hyperinsulinaemia on myocardial mass, blood pressure regulation and central haemodynamics in ratsEur J Clin Invest19962697388957202
- HwuCNKwokCFKuoCSExacerbation of insulin resistance and postprandial triglyceride response in newly diagnosed hypertensive patients with hypertriglyceridaemiaJ Human Hypertens2002164879312080433
- IngelssonESundstromJArnlowJInsulin resistance and risk of congestive heart failureJAMA20052943344116030278
- KannelWBBelangerAJEpidemiology of heart failureAm Heart J199112195172000773
- KarelisADFarajMBastardJPThe metabolically healthy but obese individual presents a favorable inflammation profileJ Clin Endocrinol Metab20059041455015855252
- KoenigWLowelHBaumertJC-reactive protein modulates risk prediction based on the Framingham Score: implications for future risk assessment: results from a large cohort study in southern GermanyCirculation200410913495315023871
- KravaritiMNakaKKKalantaridouSNPredictors of endothelial dysfunction in young women with polycystic ovary syndromeJ Clin Endocrinol Metab20059050889515985492
- LamonteMJAinsworthBEDurstineJLInfluence of cardiorespiratory fitness on the association between C-reactive protein and metabolic syndrome prevalence in racially diverse womenJ Women’s Hlth2005142339
- LauttWWThe HISS story overview: A novel hepatic neurohumoral regulation of peripheral insulin sensitivity in health and diabetesCan J Physiol Pharmacol1999775536210543718
- LauttWWPractice and principles of pharmacodynamic determination of HISS-dependent and HISS-independent insulin action: methods to quantitate mechanisms of insulin resistanceMed Res Rev20032311412424750
- LauttWWA new paradigm for diabetes and obesity: the hepatic insulin sensitizing substance (HISS) hypothesisJ Pharmacol Sci20049591715153645
- LauttWWLegareDJReidMAGAlcohol suppresses meal-induced insulin sensitization (MIS)Metab Synd Rel Disord20053519
- LauttWWMacedoMPSadriPHepatic parasympathetic nerve-dependent control of peripheral insulin sensitivity is determined by feeding and fasting: dynamic control of HISS-dependent insulin actionAm J Physiol Gastrointest Liver Physiol2001281G293611408252
- LauttWWWangXSadriPRapid insulin sensitivity test (RIST)Can J Physiol Pharmacol1998761080610326829
- LeeWYParkJSNohWYC-reactive protein concentrations are related to insulin resistance and metabolic syndrome as defined by the ATP III reportInt J Cardiol200497101615336815
- LevantesiGMacchiaAMarfisiRMMetabolic syndrome and risk of cardiovascular events after myocardial infarctionJ Am Coll Cardiol2005462778316022955
- LevineGNFreiBKoulourisSNAscorbic acid reverses endothelial vasomotor dysfunction in patients with coronary artery diseaseCirculation1996931107138653830
- MeroNSyvanneMTaskinenM-RPostprandial lipid metabolism in diabetesAtherosclerosis1998141S5359888643
- MingZFanY-JYangXSynergistic protection by S-adenosylmethionine with vitamins C and E on liver injury induced by thioacetamide in ratsFree Rad Biol Med2006406172416458192
- MollerDENew drug targets for type 2 diabetes and the metabolic syndromeNature2001414821711742415
- MooreMCSatakeSBaranowskiBEffect of hepatic denervation on peripheral insulin sensitivity in conscious dogsAm J Physiol Endocrinol Metab2002282E2869611788359
- NakazonoKWatanabeNMatsunoKDoes superoxide underlie the pathogenesis of hypertension?Proc Natl Acad Sci USA1991881004581658794
- PaiJKPischonTMaJInflammatory markers and the risk of coronary heart disease in men and womenN Engl J Med2004351259961015602020
- PatarraoRSLauttWWGuarinoMPAtropine inhibits postprandial insulin sensitivity in a dose dependent mannerDiabetologia200548A211
- PearsonTAMensahGAAlexanderRWMarkers of inflammation and cardiovascular disease: application to clinical and public health practice: a statement for healthcare professionals from the Centers for Disease Control and Prevention and the American Heart AssociationCirculation200310749951112551878
- ReidMAGLatourMGLegareDJComparison of the rapid insulin sensitivity test (RIST), the insulin tolerance test (ITT), and the hyperinsulinemic euglycemic clamp (HIEC) to measure insulin action in ratsCan J Physiol Pharmacol2002808111812269792
- ReidMAGLauttWWPattern of insulin delivery affects HISS action and insulin resistanceCan J Physiol Pharmacol2004821068107415644948
- RifaiNHigh-sensitivity C-reactive protein: a useful marker for cardiovascular disease risk prediction and the metabolic syndromeClin Chem200551504515738514
- RosenPTBallhausenTBlochWEndothelial relaxation is disturbed by oxidative stress in the diabetic rat heart: influence of tocopherol as antioxidantDiabetologia1995381157688690167
- RutterMKMeigsJBSullivanLMC-reactive protein, the metabolic syndrome, and prediction of cardiovascular events in the Framingham Offspring StudyCirculation2004110380515262834
- RutterMKPariseHBenjaminEJImpact of glucose intolerance and insulin resistance on cardiac structure and function: sex-related differences in the Framingham Heart StudyCirculation20031074485412551870
- SadriPLauttWWBlockade of hepatic nitric oxide synthase causes insulin resistanceAm J Physiol1999277G101810409156
- SadriPReidMAGAfonsoRAMeal-induced insulin sensitization in conscious and anesthetized rat models comparing liquid mixed meal with glucose and sucroseBr J Nutr2006952889516469144
- SartoriMCeolottoGPapparellaIEffects of angiotensin II and insulin on ERK1/2 activation in fibroblasts from hypertensive patientsAm J Hypertens2004176041015233979
- SchchiriMKishikawaHOhkuboYLong-term results of the Kumamoto Study on optimal diabetes control in type 2 diabetic patientsDiabetes Care200023B21910860187
- ScognamiglioRNegutCVigili De KreutzenbergSPostprandial myocardial perfusion in healthy subjects and in type 2 diabetic patientsCirculation20051121798415998667
- ShawJEHodgeAMde CourtenMIsolated post-challenge hyperglycemia confirmed as a risk factor for mortalityDiabetologia1999421050410447514
- SimonCBrandenbergerGUltradian oscillations of insulin secretion in humansDiabetes200251S2586111815489
- SimonCFolleniusMBrandenbergerGPostprandial oscillations of plasma glucose insulin and C-peptide in manDiabetologia198730769733322902
- SolzbachUHornngBJeserichMVitamin C improves endothelial dysfunction of epicardial coronary arteries in hypertensive patientsCirculation1997961513199315540
- SomogyiARuzicskaEBlazovicsAInsulin treatment decreases the antioxidant defense mechanism in experimental diabetesMed Sci Monit200511BR2061115990681
- SundstromJLindLNystromNLeft ventricular concentric remodeling rather than left ventricular hypertrophy is related to the insulin resistance syndrome in elderly menCirculation2000101259560010840010
- TakayamaSLegareDJLauttWWDose-related atropine-induced insulin resistance: comparing intraportal versus intravenous administrationProc West Pharmacol Soc20004333411056951
- TseTFClutterWEShahSDNeuroendocrine responses to glucose ingestion in man: specificity, temporal relationships, and quantitative aspectsJ Clin Invest19837227076409929
- UnnoTTagoMSuzukiYEffect of tea catechins on postprandial plasma lipid responses in human subjectsBr J Nutr200593543715946418
- UrsiniFZamburliniACazzolatoGPostprandial plasma lipid hydroperoxides: a possible link between diet and atherosclerosisFree Rad Biol Med19982525029667503
- VaccaroORuffaGImperatoreGRisk of diabetes in the new diagnostic category of impaired fasting glucoseDiabetes Care1999221490310480514
- Van De BornePHausbergMHoffmanRPHyperinsulinemia produces cardiac vagal withdrawal and nonuniform sympathetic activation in normal subjectsAm J Physiol1999276R178839887192
- Van OostromAJHHMSijmonsmaTPRabelinkTJPostprandial leukocyte increase in healthy subjectsMetabolism20035219920212601632
- WannametheeSGLoweGDOShaperAGInsulin resistance, haemostatic and inflammatory markers and coronary heart disease risk factors in Type 2 diabetic men with and without coronary heart diseaseDiabetologia20044715576515365613
- WhitesideCICellular mechanisms and treatment of diabetes vascular complications converge on reactive oxygen speciesCurr Hypertens Rep200571485415748541
- XieHLauttWWInduction of insulin resistance by cholinergic blockade with atropine in the catJ Auton Pharmacol19951536198744976
- XieHLauttWWInsulin resistance of skeletal muscle produced by hepatic parasympathetic interruptionAm J Physiol1996a270E858638967475
- XieHLauttWWInsulin resistance caused by hepatic cholinergic interruption and reversed by acetylcholine administrationAm J Physiol1996b271E587928843755
- XieHTsybenkoVAJohnsonMVInsulin resistance of glucose response produced by hepatic denervationsCan J Physiol Pharmacol19937117588319140
- ZetheliusBLithellHHalesCNInsulin sensitivity, proinsulin and insulin as predictors of coronary heart disease. A population-based 10-year, follow-up study in 70-year-old men using the euglycaemic insulin clampDiabetologia200548862715803331
- ZilversmitDBAtherogenesis: a post-prandial phenomenonCirculation19796047385222498
- ZsugaJToryKJaszlitsLPre-clinical methods for the determination of insulin sensitivityJ Biochem Biophys Meth200461253815560942