Abstract
Despite progress in pain management, chronic non-cancer pain (CNCP) represents still a clinical challenge. The efficacy and safety profile of tramadol make it suitable as a long-term treatment in a variety of CNCP conditions. New once-daily (OD) formulations of tramadol have been marketed in various countries, in order to offer the advantage of a reduced dosing regimen and to improve patients’ compliance. This review focuses on the technology, pharmacology, clinical efficacy, and safety of different once-daily tramadol formulations. Hydrophilic vs hydrophobic matrix systems and newer technologies used in once-daily formulations to control drug delivery are discussed. Three randomized controlled trials (RCTs) established OD tramadol analgesic efficacy to be superior to that of placebo for pain management and functional improvement in patients with osteoarthritis. Three RCTs demonstrated similar rates of efficacy between OD tramadol and immediate-release (IR) or sustained-release (SR) formulations, with a better adverse events profile. An open trial on long term tolerability showed that OD tramadol is generally safe in rheumatological pain treatment.
Introduction
Despite progress in pain management, chronic pain remains a major problem in most of countries. Chronic pain was once defined as pain that extends 3 or 6 months beyond onset or beyond the expected period of healign. “Chronic nonmalignant pain” is a subtype of chronic pain, which refers to persistent pain not associated with cancer. As such pain may last for many years, some consider use of term “nonmalignant” inappropriate, and prefer to speak about “chronic noncancer pain” (CNCP). CNCP is a problem of epidemic proportions. About 50 million of the estimated 75 million Americans who live with “serious pain” suffer from chronic pain, substantially reducing their quality of life. Many have been living with their pain for more than 5 years and experience pain almost 6 days a week. According to the Nuprin Pain Report, 20.8 millions of Americans experienced pain at least 101 days in the year preceding the survey. (CitationTaylor 1985) CNCP can affect virtually any body system or region, and pain severity ranges from mild to excruciating. It includes chronic pain of a nociceptive or neuropathic nature with variable influence by psychological and socioenvironmental factors.
Musculoskeletal conditions such as low back pain and osteoarthritis (OA) represent a leading cause of disability among individuals of working age. According to a recent report from the centers for disease control (CDC), the estimated prevalence of arthritis and chronic joint symptoms among adults in the United States was 33%, representing approximately 69.9 million adults in 2001. The socioeconomic burden also is significant, with chronic pain estimated to cost about 50 billion dollars annually in medical expenses. However, when considering the reduced work productivity, due to 36 million lost work days annually, the total cost rose to about 90 billion dollars (CDC 2006).
Despite progress in our knowledge of the pathophysiology of pain and OA, the management of chronic non-cancer pain continues to challenge physicians. Contemporary standard pharmacological care for the treatment of CNCP includes the use of opioid medications. The aim of opioid treatment should be to relieve pain and improve functional capacity and quality of life. Evidence from multiple randomized controlled trials indicates that opioids can relieve pain in a variety of chronic pain syndromes (CitationKalso et al 2003).
Tramadol is a synthetic, centrally acting analgesic that has been widely used for chronic pain management. Its analgesic effect results from two different pharmacologic actions. Tramadol displays a weak agonistic effect at the μ- and δ-opioid receptors and a weaker affinity for κ-opioid receptors (CitationGrond et al 2004). However, tramadol-induced analgesia is only partly antagonised by the opioid antagonist naloxone, whereas both the α2-adrenoreceptor antagonist, yohimbine (CitationDesmeules et al 1996), and the selective 5-HT3 receptor antagonist, ondansetron (CitationDe Witte et al 2001), reduced its analgesic effect. In fact, tramadol acts also on the descending inhibitory pathways by inhibiting monoamine (noradrenaline and serotonin) re-uptake.
Tramadol is formulated as a racemic mixture consisting of two enantiomers. The main activity of enantiomer(−) is the inhibition of the neuronal re-uptake of noradrenaline, whereas enantiomer(+) both interacts with μ-opioid receptors and increases serotonin synaptic concentrations by blocking serotonin re-uptake (CitationGrond et al 2004).
The efficacy and safety profile of tramadol make it suitable as a long-term treatment in a variety of CNCP conditions. In osteoarthritis patients (double-blind study), pain relief was superior with oral tramadol 300 mg than with oral dextropropoxyphene 300 mg (CitationJensen et al 1994). Similarly, in a double-blind crossover trial, tramadol 200 mg was shown to be more effective than pentazocine 150 mg (CitationBird et al 1995. No significant differences were observed in pain relief between tramadol and diclofenac (CitationPavelka et al 1998) and paracetamol/codeine combination (CitationRauck et al 1994). In the treatment of severe pain from osteoarthritis, similar pain relief was achieved with both long-acting tramadol and dihydrocodeine with NSAID’s, but tramadol interfered less with intestinal function (CitationWilder-Smith et al 2001).
Tramadol is classified as a “step II” opioid analgesic in the World Health Organization (WHO) pain treatment ladder. The American Pain Society guidelines recommend tramadol in any phase of osteoarthritis as single therapy or in combination with acetaminophen or non-steroidal anti-inflammatory drugs (NSAIDs). (CitationAPS 2002) Similarly, the American College of Rheumatology (ACR) guidelines on the management of osteoarthritis recommend tramadol in patients for whom acetaminophen, NSAIDs, and cyclo-oxygenase (COX)-2 inhibitors are no longer effective (CitationACR 2000).
The use of stronger opioid analgesics for long term management of chronic non-cancer pain is now an accepted, although still a controversial medical practice. According to recent recommendations on the use of opioids in osteoarthritis, patients for whom NSAIDs are contraindicated, or for whom combined acetaminophen, tramadol, and NSAID therapy is ineffective, may be started on low-dose opioids and titrated as needed and tolerated (CitationGoodwin et al 2005). In particular oxycodone and morphine seem to be effective in both neuropathic and musculoskeletal pain conditions (CitationKalso et al 2004). Strong opioids have a role in the treatment of low back pain when other treatments have failed. They should be prescribed as part of a multimodal treatment plan, with the aim of relieve pain and facilitate rehabilitation (CitationKalso et al. 2005).
Tramadol has been available for pain treatment in Germany since 1977. The immediate release (IR) formulations were introduced in the UK (1994), in the US (1995) and then in many other countries. The short half-life of IR tramadol requires dosing every 6 hours in order to maintain optimal analgesia. Sustained release formulations are recommended in chronic pain treatment to avoid the “peak and valley” phenomena in drug serum concentration and to maintain a stable level of analgesia. The introduction of twice-daily sustained-release (SR) formulations, which provide stable plasma concentrations when administrated at 12-hour intervals, represented the first goal of pharmaceutical research. There is an inverse relationship between number of daily doses and rate of compliance to treatment (CitationClaxon et al 2001). High-frequency dosing regimens can result in a lack of compliance, and subsequent inappropriate plasma drug concentrations and analgesia, thus they are not suitable for patients in chronic treatment. Extended-release formulations have been shown to provide the patient with better symptom control (CitationRichter et al 2003).
Several studies have demonstrated the effectiveness of SR tramadol in the treatment of chronic pain of nonmalignant origin, with fewer adverse effect than the standard formulation and better patient compliance during treatment (CitationSorge et al 1997; CitationFrank et al 1999).
Once-daily (OD), sustained-release formulations of tramadol, have been recently marketed in various countries, with the aim of providing continuous drug delivery and corresponding analgesic efficacy over 24 hours. The expected advantages are the reduction of plasma drugs peaks responsible of adverse events and the improvement of patient compliance with a once-daily dosing regimen (CitationKlotz et al 2003; CitationMalonne et al 2003).
This review focuses on the technology, pharmacology, clinical efficacy, and safety of different once-daily tramadol formulations.
Once-daily tramadol: different formulations
Tramadol is available in various pharmaceutical forms. Immediate-release (IR) formulations are capsules, soluble tablets, drops and suppositories. IR formulations normally require four to six times daily administrations, because tramadol is a freely water-soluble drug and its half-life is about 5.5 hours (CitationScott et al 2000).
Several sustained-release (SR) formulations of tramadol have been developed for twice daily administration (capsules and tablets). SR capsules contain multiple pellets of 1mm diameter (from 90 to 370, depending on dosage) consisting of a neutral core layered with tramadol and a membrane that controls the release (CitationGrond et al 2004). SR tablets instead are based on a matrix system in which tramadol is distributed, which on contact with the gastrointestinal fluid is gradually swelled and forms a retarding gel layer. Tramadol SR capsules had identical bioavailability to tramadol immediate-release capsules with lower peak concentrations and less fluctuation in plasma concentrations (CitationKeating 2006).
In order to reduce the frequency of administration and to improve patient compliance, once-daily formulations have been developed. The most commonly used method of modulating the drug release is to include it in a matrix system. A wide array of polymers has been employed as drug retarding agents.
In Europe, an hydrophilic OD tramadol formulation is produced by SMB and THERABEL GN Pharma. Hydrophilic polymer matrix systems are widely used in oral controlled drug delivery. Hydroxypropyl methylcellulose (HPMC) is commonly used in these systems (CitationHogan et al 1989). The hydration rate of HPMC increases with an increase in the hydroxypropyl content. As tramadol is a highly water-soluble drug, when a hydrophilic matrix is used, its efficacy is restricted due to rapid diffusion of the dissolved drug through the hydrophilic gel network. In an attempt to prolong the release of drug, the concentration of HPMC was increased. However the hydrophilic matrix system could not control the release of tramadol for more than 14 hours (CitationTiwari et al 2003).
For such drugs with high water solubility, hydrophobic polymers could represent more suitable matrixing agents for obtaining once-daily sustained-release dosage forms. An OD tramadol formulation based on a hydrophobic matrix is marketed by Napp Labs, Mundipharma, Zambon and MEDA. When a hydrophobic matrix system using hydrogenated castor oil (HCO) was investigated, the tramadol release rate was slower compared with the hydrophilic matrix system. Ethyl cellulose coating has been used, as a release retardant polymer, for hydrophobic matrix tablets. By comparison, combination of hydrophilic and hydrophobic polymers failed to prolong the drug release beyond 12 hours. In conclusion, the hydrophobic matrix seems to be a better system for once-daily formulations of a highly water-soluble drug like tramadol hydrochloride (CitationTiwari et al 2003).
Recently, a novel technology has been used by Labopharm Inc. (Canada) to obtain a new once-daily formulation, which permits controlled drug release over 24 hours (CitationMongin et al 2004). Contramid® is a patented, Labopharm’s proprietary advanced controlled-release drug delivery technology that uses cross-linked high-amylose starch (CLHAS) molecules as matrixing agents, for oral administration of solid dosage medications. (CitationIspas-Szabo et al 2000) Such CLHAS is prepared by (a) cross-linking and chemical modification of high amylose starch, (b) gelatinization, and (c) drying to obtain a powder capable of being used as a controlled release excipient. Following ingestion, gastric fluids transform the surface of the Contramid® into a semi-permeable membrane that stabilizes rapidly. This self-forming membrane, which does not begin to erode until it reaches the colon, regulates the release of the active drug. Contramid® technology can be applied successfully to a wide variety of active ingredients. The Tramadol Contramid® formulation is already distributed in Europe and is pending of FDA approval in USA. Labopharm”s New Drug Submission (NDS) for OD Tramadol Contramid® has been accepted for review by the Therapeutic Products Directorate of Health Canada (CitationLabopharm 2006).
Moreover, there is another tablet formulation manufactured by Biovail Corporation (once-daily Ultram® ER) that uses the innovative Smartcoat TM technology to gain a graduated release of the active drug. This is the only OD tramadol currently approved in USA (CitationBiovail 2006).
In September 2006, Cipher Pharmaceuticals Inc. (TSX: DND) announced that the Company’s New Drug Application (NDA) for CIP-TRAMADOL ER, a novel extended-release capsule formulation of tramadol with once-daily dosing, has been accepted for review by the US Food and Drug Administration (FDA) (CitationCipherpharma 2006).
Finally, a new once-daily abuse deterrent formulation of tramadol is being developed by TheraQuest Biosciences for the treatment of neuropathic pain. Comparing to CR Oxicodone, this TQ-1017 (TheraQuest’s Tramadol ER) demonstrates more robust in vitro abuse deterrent properties. It represents a secure-release formulation because it cannot be easily crushed. Intentional (to obtain rapid euphoria) or inadvertent crushing has the potential to deliver a massive dose all at once and produce neurological toxicity, including agitation, seizures, coma and respiratory failure. The active tramadol is also difficult to be extracted using common solvents, including alcohol. TQ-1017 has recently completed a Phase I study, and is going to be investigated for the management of post-herpetic neuralgia and for the treatment of painful HIV-associated neuropathy (CitationTheraQuest 2006).
Pharmacokinetics of once-daily tramadol
The pharmacokinetics of these new once-daily tramadol formulations have been investigated in three recent studies, by comparison with immediate-release and sustained release tramadol products.
In the first study, an hydrophobic once-daily tramadol formulation of in tablets 200 mg (Napp Pharmaceuticals, UK) was compared with the immediate-release (IR) tramadol solution 100 mg, in a single dose study. The systemic availability of OD tablets resulted comparable (94%) to that of IR solution. In the six days study, when comparing Once-Daily tramadol tablets 200 mg with immediate-release (IR) tramadol tablets 50 mg qid, the systemic availability of OD tramadol was found lower (74%) than IR tablets. OD tramadol exhibited a lower Cmax (maximum observed plasma concentration) and a later Tmax (time required to reach Cmax) than IR tablets (CitationSmith et al 1999).
In the second study, an hydrophilic once-daily tramadol formulation 200 mg (SMB Technology, Belgium) was compared with immediate-release tramadol 50 mg qid. In the single dose study conducted on 29 healthy volunteers, similarly to the previous study (CitationSmith et al 1999) OD tramadol showed a significantly lower Cmax compared to IR tablets, for both (+)-tramadol (300 vs 646 ng/ml) and (−)-tramadol (255 vs 580 ng/ml). Both enantiomers showed longer Tmax in OD tramadol compared to IR tablets (10 vs 1.3 h). However, systemic bioavailability of tramadol and its metabolite enantiomers was similar for both formulations. The AUCt (area under the plasma concentration-time curve) and the AUC∞ calculated as (AUCt + Ct/Ke) were comparable. In the fasting state and after a fatty meal, pharmacokinetic parameters did not exhibit significant differences, showing that food did not modify OD tramadol absorption. Following repeated dosing, in the seven days study, there was no significant difference between the AUC of OD tramadol 200 mg and IR tramadol qid. As expected, the Cmax was lower after the administration of IR tramadol 50 mg, whereas the Cmin (minimum observed plasma concentration) was similar for both formulations. The OD tramadol produced significantly longer Tmax and sustained plasma drug concentrations for at least 24 h (CitationMalonne et al 2003).
The third pharmacokinetic study, conducted by CitationBodalia et al (2003) on 22 healthy volunteers for six days, compared three different formulations of oral tramadol: OD tramadol 150 mg or 200 mg tablets (Napp Pharmaceuticals, UK) and IR tramadol 50 mg capsules every eight hours. The pharmacokinetic profile of tramadol and its metabolite O-desmethyltramadol (M1) followed similar trends. Their AUC24 (area under the plasma concentration-time curve over 24 hours), Cmax, and Cmin values were significantly higher for the IR capsules compared to the OD tablets. However, as the confidence intervals of the Frel (relative systemic availability, expressed as geometric mean) values were within the limits of acceptability for bioequivalence, these three treatments can be considered to have equivalent mean systemic availability. The mean relative systemic availabilities for the OD tablets 150 mg and the OD tablets 200 mg versus the IR capsules were 89.6 % and 90.5%, respectively.
In conclusion, these new sustained release formulations of tramadol have suitable pharmacokinetic characteristics to be administered once-a-day as an effective and safe treatment for acute and chronic pain.
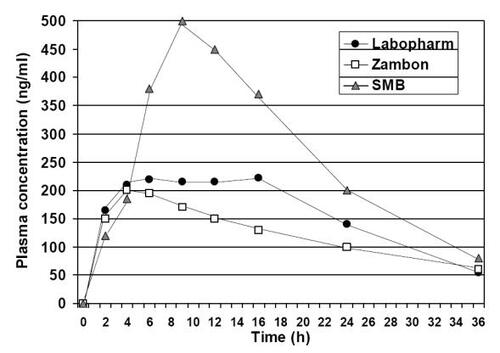
Only recently, a randomized controlled trial comparing two different OD tramadol formulations has been published by CitationHernandez-Lopez et al (2006). This is the first study that compares the bioavailability of a currently marketed OD tramadol formulation 200 mg using an hydrophobic matrix (Zambon, Spain) with the new OD tramadol formulation 200 mg using the Contramid® technology (Labopharm, Canada), both given as a single dose in the fasting state. 24 of 26 subjects were evaluable for the pharmacokinetic analysis of racemic tramadol and racemic O-demethyltramadol. All pharmacokinetic parameters (AUC, Cmax, C24h, and Tmax) were significantly higher for tramadol Contramid® (p < 0.0004), whereas the elimination half-life (T½) was significantly shorter (7.4 vs 14.9 h, p = 0.0001). Following tramadol Contramid® oral administration, mean plasma concentrations maintained a plateau above 200 ng/ml for a long duration (≥12h) from 4 h through 16 h after dose, while for the reference formulation the plasma levels were maintained for only 2 h, from 4 h through 6 h. Mean plasma concentration of tramadol at 24 h were significantly higher after tramadol Contramid® administration (38.9 vs 26.2 ng/ml p = 0.0001). As the confidence intervals fall outside of the range of acceptability for bioequivalence, these formulations cannot be considered bioequivalent. OD tramadol using Contramid® technology seems to have a better controlled-release profile and can be evaluated to be suprabioavailable. Finally, authors compared their results with those obtained by CitationMalonne et al (2004) with the hydrophilic once-daily tramadol formulation 200 mg (SMB Technology, Belgium). When comparing the Tmax, expressed as median (min-max), the following values were observed: OD tramadol Contramid® (Labopharm) 9.0 h (2–16), OD tramadol (Zambon) 4.5 h (2–12), and OD tramadol (SMB Technology) 10 h (6–12) (). The hydrophilic formulation (SMB Technology) showed a lag during which no appreciable drug absorption occurs, and the maximum concentration was achieved after about 10 hours, followed by a fast elimination process, similar to the immediate-release formulations. As shown in , there was not a plateau in the plasma concentration-time curve. Thus the author concluded that this should be considered a “delayed-release” formulation, whereas the other two (using the hydrophobic matrix and the Contramid® technology, respectively from Zambon and Labopharm) showed pharmacokinetics characteristics of “controlled-release” formulations (CitationHernandez-Lopez et al 2006).
Figure 1 Mean plasma concentration-time profile for racemic tramadol (sum of both enantiomers) after a single oral dose in the fasting state of three different formulations: OD Tramadol Contramid® 200 mg (Labopharm), OD Tramadol 200 mg (Zambon), and OD Tramadol 200 mg (SMB Technology) (CitationMalonne et al 2003; CitationHernandez-Lopez et al 2006).
Efficacy of once-daily tramadol
The clinical efficacy of once-daily tramadol in treating chronic non-cancer pain was first established in two randomized double-blind clinical trials. These compared the once-daily formulation with the immediate-release tramadol in the treatment of pain in patients with osteoarthritis (CitationAdler et al 2002; CitationBodalia et al 2003).
The first of these trials was a multicenter study, with a double-blind, double-dummy, parallel design (CitationAdler et al 2002). 279 adult patients with radiographic evidence of OA of the spine, hip, and/or knee were assigned to received either OD tramadol (Napp Pharmaceuticals, UK) or IR tramadol, according to a 2:1 randomization, so that more data could be obtained on the OD formulation. During the first week, doses were adjusted until patients required no more than two doses of rescue medication (each dose: Acetaminophen 1000 mg) per day. The OD tramadol group received 150–400 mg on waking (n = 188), while the IR tramadol group received 50–100 mg TDS or QDS (n = 91). At the end of the titration period at the optimal dose level of treatment, patients were assessed for 4 weeks. Both treatments were equally effective in improving pain control. OD and IR tramadol were therapeutically equivalent according to pain intensity scores at all assayed time points (morning and evening), both at baseline (overall 47 and 51 mm, respectively) and after treatment (overall 21 and 22 mm, respectively). The 24 hours duration of the OD tramadol was clinically confirmed by the absence of the “end of dose” effects in the morning scores. Similar dropout rates were recorded (OD tramadol 49% vs IR tramadol 52%). Most of the withdrawals were due to adverse events, with a similar profile between the two treatments. There was no a statistically significant difference between treatments with respect to the number rescue doses over the last 24 hours of the study (overall 0.82 times/day), and the proportion of nights woken. Assessment of successful global pain management was determined by combining patients’ and investigators’ ratings of pain control on a 5 point categorical scale (from poor to excellent) for each treatment. These values were similar for OD tramadol and IR tramadol (overall 65% of the patients who completed the study obtained good to excellent pain relief), further suggesting therapeutic equivalence between these two formulations.
The second trial comparing the efficacy of OD tramadol with IR tramadol was published in 2003 (CitationBodalia et al 2003). This multicenter, randomized, double-blind, double-dummy, crossover trial, evaluated the efficacy and tolerability of three different medications in patients with moderate pain caused by radiographically confirmed OA of the spine, hip, and/or knee. Tested drugs were OD tramadol (Napp Pharmaceuticals, UK) 150 mg tablets in the morning, OD tramadol 200 mg tablets in the morning, and IR tramadol 50 mg capsules three times every day (in the morning, afternoon, and at bedtime). Patients were randomized to one of six treatment sequence groups. Patients received the appropriate medication for five to eight days, and then were switched to the alternative treatments. Paracetamol was allowed as escape medication. 134 patients were recruited from 22 participating centers. 108 completed all three treatment periods. There was not statistically significant difference in the median VAS pain scores in any of the four time points investigated: before and after the morning dose (range 33 to 40 mm), before the afternoon dose, and at bedtime dose (range 26 to 31 mm). The use of escape medications was similar for the three treatments, both during the washout period (overall 2–3 doses/day) and during the last five days of treatment (overall 0.4–0.6 doses/day). Also the number of nights woken was similar between treatments. One-third of the patients did not wake from pain at all during the last three nights of each treatment period. Finally, according to the number of patients expressing a preference, there were no significant differences between groups in patients’ treatment preference.
In 2004, CitationMongin et al (2004) published a randomized, double-blind, multicenter study to compare the OD tramadol Contramid® formulation (Labopharm) with a twice-daily formulation. At the baseline phase, analgesic washout was programmed prior to randomization, and baseline evaluations were performed. 431 patients with diagnosis of moderate to moderately severe osteoarthritis of the knee (according to ACR criteria) were randomized. During the titration phase, dose escalation by 100 mg every 2nd and 3rd day was conducted until minimum effective or maximum tolerated dose was achieved. Once the optimum dose level was established, the efficacy and safety of medications was evaluated in the maintenance phase for 84 days. Most patients (50.9% in the OD tramadol arm and 49% in the tramadol twice-daily arm) received 200 mg daily as the optimal dose. Similar discontinuation rates due to adverse events were recorded (OD tramadol 8.8% vs twice-daily tramadol 10.2%). Both formulations provided similar analgesia, with a 58% reduction on the primary efficacy parameter (percentage change in the WOMAC pain subscale score) at 12 weeks, which is comparable with pain relief obtained with other analgesics, such as codeine and diclofenac. Similarly, no statistically significant differences were observed for each of the secondary endpoints (WOMAC stiffness, physical function, global score and VAS 24-hours evaluation). The majority of patients (about 83%) and investigators (86%) gave an overall rating of the study medication as effective or very effective for both formulations.
In 2004, the results of the first two placebo-controlled studies evaluating the efficacy of OD tramadol were published (CitationBabul et al 2004; CitationMalonne et al 2004).
The first of these trials was a multicenter, double-blind, parallel-group, placebo-controlled study, that enrolled patients with osteoarthritis of the hip or knee, according to European League Against Rheumatism (EULAR) criteria, with symptomatology for ≥ 6 months, requiring regular analgesic treatment for ≥ 1 month. Patients were eligible for this study if they had pain scores ≥35 mm on the 100 mm Huskisson horizontal VAS (0 mm = no pain, 100 mm = worst possible pain), and functional discomfort ≥4 on the Lequesne discomfort index (total score 0 = no pain, total score 20 = most intense pain). Patients were randomized to receive either OD tramadol (SMB Technology, Belgium) 200 mg or placebo for 14 days. Acetaminophen was allowed as rescue analgesia. Regular assessments were programmed at day −7 and days 0, 7, and 14. Of 231 randomized patients, 197 completed the study (OD tramadol n = 85; placebo n = 112). Patients who received OD tramadol had a lower pain intensity scores both on day 7 and day 14 (P = 0.0002 and P = 0.010 respectively) than control patients. Mean decrease in pain intensity was 2.43 cm in the OD tramadol group, compared with 1.55 cm in the placebo group. The proportion of responders was significantly higher in the OD tramadol group compared with the placebo group (64.7% vs 50.0% respectively; P = 0.039). Similarly, the proportion of patients who did not require rescue doses was higher in the OD tramadol group compared with the placebo group (60.0% vs 36.6% respectively; P = 0.001). The onset of efficacy was also faster for OD tramadol than placebo (3 vs 6 days, respectively; P < 0.001). Functional improvement, as measured on Lequesne discomfort index, was statistically different between groups only at day 7, however there was no difference at day 14. The patients’ global assessment of treatment was similar for OD tramadol and placebo based on a 7-item verbal scale (from much improved to much worse). However OD tramadol was ranked as a “very good” or “good” method of pain management by significantly more investigators (61.2% vs 30.4%; P < 0.001) compared with placebo.
A second placebo-controlled study assessed the efficacy of OD tramadol (Biovail Technology, USA) in 246 patients with radiographically confirmed OA of the knee and pain scores ≥40 mm (CitationBabul et al 2004). Patients received either OD tramadol (n = 124) from 100 mg QD to a maximum of 400 mg QD, after the first week, or placebo (n = 122) for 12 weeks. Clinical evaluations were conducted at Week 1, Week 2, Week 4, Week 8, and Week 12 or at early termination. In the Arthritis Pain Intensity mean change was significantly greater for OD tramadol than placebo (30.4 vs. 17.7 mm; P < 0.001) Treatment differences emerged into the first week of therapy. Similarly, mean change on the WOMAC (Western Ontario and McMaster Universities) pain subscale was significantly greater for OD tramadol over placebo (120.1 vs 69.0 mm; P < 0.001). Results from all the other efficacy outcome measures, such as WOMAC Physical Function Subscale, WOMAC Stiffness Subscale, and chronic pain sleep inventory (CPSI®), were similar to these main findings, with OD tramadol resulting significantly superior to placebo. Finally, on both the Patient and the Physician Global Assessment of Therapy, tramadol was significantly different from placebo.
The results of these two placebo-controlled trials show that OD tramadol given at doses of 200 to 400 mg provided effective analgesia, when compared to placebo.
The last available study on once-daily tramadol is a multicenter, randomized, double-blind, placebo-controlled clinical trial that included 1020 adults with osteoarthritis of the knee or hip, with baseline pain intensity ≥ 40 on a 100 mm VAS (CitationGana et al 2006). Patients in the OD tramadol active arm were titrated to a target dose of 100, 200, 300, or 400 mg once daily. Mean changes in WOMAC Osteoarthritis Index Pain and Physical Function Subscale were significantly different between OD tramadol and placebo (p ≤ 0.021), and for each dose (p ≤ 0.05). OD tramadol resulted more effective than placebo also in the other WOMAC items (joint stiffness subscale, composite score, pain intensity of the index joint, and daily pain intensity score). Global patient assessment of disease activity and pain intensity was significantly better for OD tramadol 200 and 300 mg than placebo (p ≤ 0.05). Tramadol 400 mg was associated to a higher incidence of adverse events.
In conclusion, six RCTs confirmed the clinical efficacy of different OD tramadol formulations in chronic non-cancer pain management, in particular in the treatment of moderate to severe osteoarthritis ( and ).
Table 1 Efficacy of OD tramadol vs other formulation (IR and SR)
Table 2 Efficacy of OD tramadol vs placebo
Safety and tolerability of once-daily tramadol
To date, the safety and tolerability of OD tramadol has been examined in a total of 7 published clinical studies (CitationAdler et al 2002; CitationBodalia et al 2003; CitationBabul et al 2004; CitationMalonne et al 2004, Citation2005; CitationMongin et al 2004; CitationGana et al 2006). As expected with an opioid agonist such as tramadol, the 3 most affected systems were the gastrointestinal system, central nervous system, and peripheral nervous system. Adverse events (AEs) associated with OD tramadol included nausea, vomiting, diarrhea, constipation, drowsiness, dizziness, headache, somnolence, and pruritus. Nausea and dizziness were the most common adverse events. Most (91%) of the AEs were reported to be mild (CitationBodalia et al 2003). No serious adverse events were reported. No patient treated with OD tramadol developed clinical respiratory depression. Tramadol is unlikely to produce clinically relevant respiratory depression at the recommended dose (CitationWarren et al 2000; CitationNieuwenhuijs et al 2001). We reported a case of iatrogenic respiratory depression following tramadol overuse in a patient undergoing haemodialysis treatment (CitationMattia et al 2004).
The medical examinations and laboratory tests showed that OD tramadol had no clinically meaningful effects on any laboratory test results, vital signs, physical examination findings, or ECG findings (CitationBodalia et al 2003; CitationBabul et al 2004). Adverse events occurred most often with higher doses (400 mg) (CitationGana et al 2006).
In both the placebo-controlled trials, the overall incidence of adverse events was significantly higher for patients treated with OD tramadol compared to those treated with placebo (P < 0.001) (CitationBabul et al 2004; CitationMalonne et al 2004). Similarly, the proportion of patients who dropped out of the study as a result of AEs was significantly higher in the OD tramadol group compared to placebo (P < 0.001) (CitationBabul et al 2004; CitationMalonne et al 2004) However, the frequency and severity of AEs with OD tramadol were similar to those observed for the immediate- and slow-release formulations. (CitationAdler et al 2002; CitationBodalia et al 2003; CitationMongin et al 2004) The percentages of subjects reporting at least one symptom were similar, ranging from 16% to 22%, with the OD tramadol and the IR tramadol (CitationBodalia et al 2003). Obviously, the AE profiles were also similar for the different formulations.
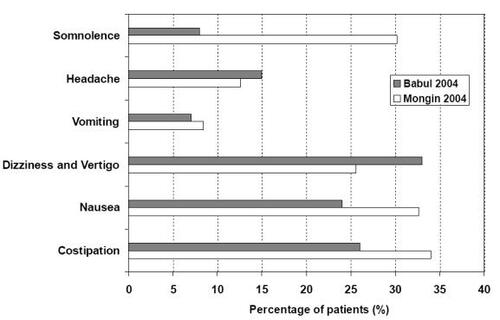
The long-term tolerability open study conducted by CitationMalonne et al (2005) on 193 patients with OA and low back pain for 12 weeks showed that once-daily tramadol (Laboratoires SMB, Belgium) is safe and well tolerated in most of rheumatological patients. The incidence rate of adverse events was clearly higher during the first week (approximately 19%) than in the following weeks, and decreased after the first month of treatment (between 1 and 5%). This confirms the long-term tolerability of OD tramadol. According to the results of this open study, the safety profile of OD tramadol appears extremely more favorable than in the two 12 weeks RCTs (CitationBabul et al 2004; CitationMongin et al 2004), as shown in . One reason for this difference could be the more stringent conditions of randomized, controlled, double-blind trials (CitationBabul et al 2004; CitationMongin et al 2004) compared to postmarketing surveillance open studies.
Figure 2 Most common adverse events likely related to OD tramadol in 12 weeks double-blind RCTs (CitationBabul et al 2004; CitationMongin et al 2004).
However, also in this long-term tolerability open study, there is a main limit that could represent the difference between the observed study results and current clinical practice. Despite polipharmacotherapy is the most commonly used therapeutic strategy in chronic noncancer pain, concomitant treatment with corticosteroids, non-steroidal anti-inflammatory agents, local anesthetics, centrally acting analgesics, neuroleptics, antidepressants, or hypnotics was prohibited in this study (CitationMalonne et al 2005). In the clinical setting, the risk of drug interaction should be always considered when using tramadol with certain compounds, in particular with serotoninergic medications (additive effect on increasing serotonin) leading to an increased possibility of serotonin syndrome and seizures, and with other drugs which compete for the same liver metabolic pathways (CYP2D6 and CYP3A4 of the cytochrome P450 system) (CitationClose 2005).
Studies suggested that the incidence of tramadol-induced seizures is rare, especially in the therapeutic dosage range, and no cases of seizure were recorded in OD tramadol clinical studies. However, there has been a recent warning about the potential risk of seizure when tramadol is used in patients with conditions predisposing to seizure (diagnoses of epilepsy, malignant brain tumor, stroke, head trauma, alcoholism, etc.) or in conjunction with commonly prescribed drugs in chronic pain management, such as anticonvulsants and antidepressants (tricyclic antidepressants and serotonin selective reuptake inhibitors) (CitationGardner et al 2000; CitationClose 2005).
Conclusion
The efficacy and safety profile of tramadol make it suitable as a long-term treatment in a variety of CNCP conditions. OD tramadol formulations show the advantage of smoother plasma concentration profile, with more gradual absorption and lower peak concentrations. Based on results of several controlled clinical studies, the efficacy of OD tramadol is similar to other tramadol formulations for the management of chronic non-cancer pain. The OD tramadol allows patients to maintain an acceptable level of analgesia following a single daily administration, while avoiding peaks in plasma concentration and reducing the incidence of adverse events. OD tramadol has a clinically favorable adverse events profile, in particular with regard to reduction of dizziness and vomiting. Furthermore, OD tramadol has the potential to provide patients with rheumatological pain optimal analgesic effect, with fewer interruptions in sleep, and enhanced physical function. Patient satisfaction was demonstrated through the high percentage of patients rating therapy with OD tramadol as effective or very effective. The OD tramadol formulations could respond to the problem of inconsistent analgesia resulting from lack of compliance to treatment with higher frequency dosing regimens.
References
- ACR GuidelinesRecommendations for the Medical Management of Osteoarthritis of the Hip and knee: 2000 update. American College of Rheumatology Subcommittee on Osteoarthritis GuidelinesArthritis Rheum20004319051511014340
- AdlerLMcDonaldCO”BrienCcomparison of once-daily tramadol with normal release tramadol in the treatment of pain in osteoarthritisJ Rheumatol2002292196912375333
- APS GuidelinesAmerican Pain Society guideline for treatment of arthritis painJ Pain Palliat Care Pharmacother200216130214635836
- BabulNNoveckRChipmanHEfficacy and safety of extended-release, once-daily tramadol in chronic pain: a randomized 12-week clinical trial in osteoarthritis of the kneeJ Pain Symptom Manage200428597115223085
- Biovail Investors Relations [online] Accessed September, 2006. URL: http://www.biovail.com
- BirdHAHillJStratfordMA double blind cross-over study comparing the analgesic efficacy of tramadol with pentazocine in patients with osteoarthritisJ Drug Dev Clin Pract19957818
- BodaliaBMcDonaldCJSmithKJA comparison of the pharmacokinetics, clinical efficacy, and tolerability of once-daily tramadol tablets with normal release tramadol capsulesJ Pain Symptom Manage200325142912590030
- [CDC] Centers for Disease Control and PreventionUpdate: Direct and in direct costs of arthritis and other rheumatic conditions – United States [online]1997 Accessed September 2006. URL: http://www.cdc.gov
- CipherpharmaProduct overview, CIP Tramadol [online] Accessed December, 2006. URL: http://www.cipherpharma.com
- ClaxonAJCramerJPierceCA systematic review of the associations between dose regimens and medication complianceClin Ther200123129631011558866
- CloseBRTramadol: does it have a role in emergency medicine?Emerg Med Australas200517738315675908
- DesmeulesJAPiguetVCollartLContribution of monoaminergic modulation to the analgesic effect of tramadolBr J Clin Pharmacol1996417128824687
- De WitteJLSchoenmaekersBSesslerDIThe analgesic efficacy of tramadol is impaired by concurrent administration of ondansetronAnesth Analg20019213192111323369
- FrankMSturmMArnauHQuality of life and patient compliance during pain therapy: multicenter study using Tramundin retard [in German]Fortschr Med199911738910384747
- GanaTJPascualMLFlemingRRExtended-release Tramadol in the treatment of osteoarthritis: a multicenter, randomized, double-blind, placebo-controlled clinical trialCurr Med Res Opin200622139140116834838
- GardnerJSBloughDDrinkardCRTramadol and seizures: a surveillance study in a managed care populationPharmacotherapy2000201223431
- GoodwinJLKraemerJJBajwaZHThe use of opioids in the treatment of osteoarthritis: when, why, and how?Curr Pain Headache Rep20059390816282039
- GrondSSablotzkyAClinical pharmacology of TramadolClin Pharmacokinet20044387992315509185
- Hernandez-LopezCMartinez-FarnosLKarhuDComparative bioavailability between two Tramadol once-daily oral formulationsMethods Find Exp Clin Pharmacol200628373816894407
- HoganJEHydroxypropyl methylcellulose sustained release technologyDrug Dev Ind Pharm1989152797599
- Ispas-SzaboPRavenelleFHassanIStructure-properties relationship in cross-linked high-amylose starch for use in controlled drug releaseCarbohydr Res20003231637510782298
- JensenEMGinsbergFTramadol versus dextropropoxyphene in the treatment of osteoarthritisDrug Invest1994821118
- KalsoEAllanLDellemijnPLIRecommendations for using opioids in chronic non-cancer painEur J Pain20037381612935789
- KalsoEEdwardsJEMooreRAOpioids in chronic non-cancer pain: systematic review of efficacy and safetyPain20041123728015561393
- KalsoEAllanLDobrogowskyJDo strong opioids have a role in the early management of back pain?. Recommendations from a European expert panelCurr Med Res Opin20052118192816307703
- KeatingGMTramadol sustained-release capsulesDrugs2006662233016451094
- KlotzUTramadol-the impact of its pharmacokinetic and pharmacodynamic properties on the clinical management of painAnzneimittelforschung2003536817
- Labopharm [online] Accessed September, 2006. URL: http://www.labopharm.com
- MalonneHCoffinerMFontaineDLong-term tolerability of tramadol LP, a new once-daily formulation, in patients with osteoarthritis or low back painJ Clin Pharm Ther2005301132015811163
- MalonneHCoffinerMSonetBEfficacy and tolerability of sustained-release tramadol in the treatment of symptomatic osteoarthritis of the hip or knee: a multicenter, randomized, double-blind, placebo-controlled studyClin Ther20042617748215639689
- MalonneHSonetBStreelBPharmacokinetic evaluation of a new oral sustained release dosage form of tramadolBr J Clin Pharmacol200357270814998423
- MattiaCColuzziFOnce-daily Tramadol in rheumatological painExpert Opin Pharmacother2006718112316925507
- MattiaCColuzziFTramadolFocus on musculoskeletal and neuropathic painMinerva Anestesiol2005715658416163147
- MattiaCMazzaferroSColuzziFRespiratory depression following iatrogenic tramadol overuse in a patient with chronic renal failureJ Headache Pain200451379
- MonginGYakusevichVKpeAEfficacy and safety assessment of a novel once-daily tablet formulation of TramadolClin Drug Invest20042454558
- NieuwenhuijsDBruceJDrummondGBInfluence of oral tramadol on the dynamic ventilatory response to carbon dioxide in healthy volunteersBr J Anaesth200187860511878687
- PavelkaKPeliskovaZStelikovaHIntraindividual differences in pain relief and functional improvement in osteoarthritis with diclofenac or tramadolClin Drug Invest19981619
- RauckRLRuoffGEMcmillenJIComparison of tramadol and acetaminophen with codeine for long-term pain management in elderly patientsCurr Ther Res Clin Exp199455141731
- RichterAAntonSEKochPThe Impact of Reducing Dose Frequency on Health OutcomesClin Ther20032523073514512137
- ScottLJPerryCMTramadol: a review of its use in periopera-tive painDrugs2000601397610929933
- SmithKJMillerAJNicholsTPOnce-daily Tramadol tablets: linear pharmacokinetics [abstract]19999th World Congress on Pain in Vienna, Austria, 1999SeattleIASP Press3367
- SorgeJStadlerTComparison of the analgesic efficacy and tolerability of tramadol 100mg sustained-release tablets and tramadol 50 mg capsules for the treatment of chronic low back painClin Drug Invest19971415764
- TaylorHThe Nuprin pain report1985New YorkLouis Harris and Associates
- Theraquest Biosciences [online] Accessed May, 2006. URL: http://www.theraquestinc.com
- TiwariSBMurthyTKPaiMRControlled release formulation of tramadol hydrochloride using hydro-philic and hydrophobic matrix SystemAAPS PharmSciTech2003416
- WarrenPMTaylorJHNicholsonKEInfluence of tramadol on the ventilatory response to hypoxia in humansBr J Anaesth2000852111610992826
- Wilder-SmithCHHillLSpargoKTreatment of severe pain from osteoarthritis with slow-release tramadol or dihydrocodeine in combination with NSAID’s: a randomised study comparing analgesia, antinociception and gastrointestinal effectsPain200191233111240075