Abstract
Pancreatic enzyme supplements (PES) are used in chronic pancreatitis (CP) for correction of pancreatic exocrine insufficiency (PEI) as well as pain and malnutrition. The use of porcine pancreatic enzymes for the correction of exocrine insufficiency is governed by the pathophysiology of the disease as well as pharmacologic properties of PES. Variability in bioequivalence of PES has been noted on in vitro and in vivo testing and has been attributed to the differences in enteric coating and the degree of micro-encapsulation. As a step towards standardizing pancreatic enzyme preparations, the Food and Drug Administration now requires the manufacturers of PES to obtain approval of marketed formulations by April 2010. In patients with treatment failure, apart from evaluating drug and dietary interactions and compliance, physicians should keep in mind that patients may benefit from switching to a different formulation. The choice of PES (enteric coated versus non-enteric coated) and the need for acid suppression should be individualized. There is no current standard test for evaluating adequacy of therapy in CP patients and studies have shown that optimization of therapy based on symptoms may be inadequate. Goals of therapy based on overall patient presentation and specific laboratory tests rather than mere correction of steatorrhea are needed.
Chronic pancreatitis (CP) is a progressive inflammatory condition of the pancreas that is characterized by abdominal pain (usually) and is often associated with exocrine and endocrine insufficiency. The initiation of pancreatic enzyme supplements (PES) is common in the management of CP and other conditions associated with pancreatic enzyme insufficiency (PEI), such as cystic fibrosis (CF) or pancreatic surgery. Through this review we present the existing data and guidelines on the use of PES in CP. The initial portion of the article will address the physiologic effects of PES, followed by the physiochemical properties of these preparations and clinical recommendations regarding their use.
Physiologic effects of pancreatic exocrine insufficiency
Fat malabsorption
The progressive destruction of pancreatic acinar cells leads to PEI. The most common clinical manifestation of PEI is steatorrhea, defined as more than 7 grams of fecal fat per day while consuming a 100 g fat diet.Citation1 Pancreatic fat malabsorption usually precedes malabsorption of other macronutrients in CP, and is related to various factors. There is rapid degradation of pancreatic lipase due to the presence of pancreatic proteases and acid in the duodenum.Citation2,Citation3 In addition, in the acidic duodenal milieu, bile salt precipitation and subsequent adsorption to undigested food reduces the bile salt pool.Citation4,Citation5 And finally, CP patients are believed to have a defect in ileal mucosal absorption of bile salts, effectively reducing the availability of bile salts for enterohepatic circulation.Citation6 A final factor contributing to pancreatic steatorrhea is the presence of neurohormonal disturbances resulting in gallbladder hypomotility and accelerated gastric and intestinal transitCitation7–Citation9 (see section on Motility).
Steatorrhea occurs in CP only after the pancreatic enzyme output has diminished by 90% of the normal output.Citation10,Citation11 The large reserve capacity of the pancreas, noted in these earlier studies, may be due to the non-pancreatic gastric and lingual lipases.Citation12 These enzymes, which play an insignificant role in fat digestion in healthy individuals, can contribute significantly to the digestion of dietary triglycerides (up to 30%) in patients with PEI.
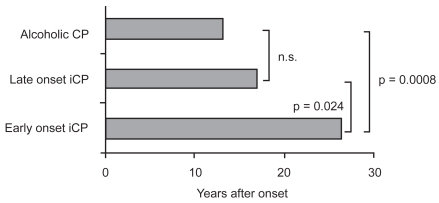
Approximately 50% of CP patients experience steatorrhea within a median of 10–12 years after the onset of CP, but this may vary based on the etiology of CP.Citation13,Citation14 Early studies classified CP into two broad types: alcoholic (ACP) or non-alcoholic (NACP) (which is further subdivided into early-onset and late-onset NACP) (see ). Early-onset NACP occurs in children and adolescents and is often characterized by pain, but with longer preservation of pancreatic function and later development of calcifications as compared to alcoholic CP and late-onset NACP. PEI is less common with NACP than ACP.Citation14
Figure 1 Onset of pancreatic exocrine insufficiency in patients with alcoholic and nonalcoholic etiologies. Reproduced with permission from Layer P, Keller J. 2003. Lipase supplementation therapy: standards, alternatives, and perspectives. Pancreas, 26:1–7. Copyright © 2003 Lippincott Williams & Wilkins.
Abbreviations: CP, chronic pancreatitis; iCP, idiopathic chronic pancreatitis.
Randomized placebo controlled trials have shown that treatment with PES improves steatorrhea, as measured by increased fat absorption, reduced fecal fat excretion, decreased stool weight and frequency, improved stool consistency and improved symptom scores.Citation15–Citation18 Other studies have demonstrated that patients receiving PES report weight gain and improved quality of life, and studies demonstrate decreased defecation rates,Citation19 increased cholesterol absorption and improved enterohepatic cycling of bile salts.Citation5,Citation20
Pain
The pain in CP is the most debilitating symptom of the disease and often leads to malnutrition, especially if the pain is related to meals. ACP and early-onset NACP are more commonly associated with pain as compared to late-onset NACP.Citation14 The pathogenesis of pain is multi-factorial and believed to be a result of perineural inflammation, visceral hyperalgesia, and increased pancreatic ductal and parenchymal pressure. Complications such as stones, strictures, and pseudocysts may also contribute to pain in CP.
Cholecystokinin (CCK) may play an important role in CP related pain. Normal physiology is such that CCK releasing peptide (CCKrp), which is produced in the duodenum, stimulates the release of CCK. In turn, CCKrp is degraded by pancreatic serine proteases. In CP patients with PEI, lack of serine proteases leads to uninhibited production of CCK, a potent stimulator of pancreatic enzymes. This is believed to result in increased pancreatic ductal and parenchymal pressure, and hence pain. Several animalCitation21 and humanCitation22 studies have supported the presence of this regulatory pathway, while others have not.Citation23,Citation24 The potential pain benefit of PES in CP pain is based on restoring this negative feedback mechanism.
Randomized controlled trials have suggested that non-enteric coated PES reduce pain in CP,Citation25,Citation26 whereas enteric coated forms are less beneficial.Citation27–Citation29 A meta-analysis did not support the use of PES for the relief of pain in all patients.Citation30 In the above studies, however, the patients with idiopathic CP and patients with less advanced disease (“small duct CP”) achieved the greatest pain relief with PES. Enzyme preparations with high protease content may be more effective in reducing pain, while enzyme preparations with high lipase content are more effective in patients with steatorrhea.Citation31 It is recommended that even though PES are limited in their effectiveness in pain relief, the non enteric coated forms are worth a trial in patients with less advanced disease, and further studies are needed to define whether certain subsets of patients with painful CP are more likely to respond to enzyme therapy.
Motility disorders
Motility disorders are common in patients with CP, and are related to alterations in neurohormonal regulation. GI hormones such as CCK and pancreatic polypeptide (PP) are important in the regulation of GI motility.Citation8,Citation9 The endogenous release of these hormones is adversely affected by the presence of undigested food in the intestines. Abnormal CCK and PP levels have been observed in CP patients with PEI. In addition, the development of secondary (apancreatic) diabetes mellitus leading to autonomic neuropathy can further compromise GI motility.Citation32
Abnormal motility patterns in CP patients include accelerated gastric emptying,Citation7,Citation33 altered post-prandial antroduodenal motility,Citation9 and alterations in gallbladder motility (delayed gallbladder contraction and reduced gallbladder emptying).Citation7,Citation8 The severity of these abnormalities is often related to the degree of PEI and their presence often compounds the maldigestion and abdominal discomfort associated with CP.
PES therapy is effective in normalizing the altered levels of GI hormones,Citation7,Citation34 and correcting accelerated gastric emptyingCitation7,Citation33 and abnormal antroduodenal motility.Citation8,Citation35 The normalization of such motility disorders may be attributed to improved lipid digestion and ileal braking induced by breakdown products such as oleic acids, triglycerides and short chain fatty acids. Improvement in gallbladder contraction with PES has been demonstrated in some studiesCitation36,Citation37 but not in others.Citation7
Malnutrition
In CP patients with PEI, maldigestion of dietary macronutrients (fat, protein and carbohydrates) and poor oral intake lead to health problems associated with malnutrition. CP patients often suffer from malnutrition and have a low body mass index and asthenic body type.
Deficiencies in fat-soluble vitamins A, E and K may lead to symptoms such as impaired nighttime vision, cerebellar ataxia, and/or increased prothrombin time.Citation38–Citation40 When compared to healthy controls, CP patients have lower serum levels of vitamin D, decreased bone mineral density and an increased incidence of osteoporosis.Citation41–Citation43 In addition, they may suffer from vitamin B12 deficiency due to both impaired release of B12 from complexes and bacterial overgrowth (a frequent finding in CP patients).Citation44
Atherogenic alteration in serum lipoproteins(low levels of HDL-C and Apo-A)Citation45 along with lifestyle factors such as smoking and alcohol may account for the increased prevalence of life-threatening cardiovascular lesions seen in CP patients.Citation46,Citation47
Although elaborate trials are lacking, PES does help to ameliorate the malnutrition. A higher body weight and improved serum albumin levels have been demonstrated in CP patients who received PES.Citation48 In malnourished CP patients with PEI, the optimization of PES therapy based on the results of C-13 Mixed Triglyceride breath test showed an improvement in fat digestion, body weight, serum levels of retinol binding protein (RBP) and the normalization of prealbumin after one year of optimized therapy.Citation49 In addition, serum HDL levels have been shown to rise significantly, whereas levels of cholesterol or triglycerides in other lipoproteins remained unchangedCitation20 and this may have a cardioprotective effect. PES, however, is not sufficient for correcting fat soluble vitamin (A, D, E and K) deficiencies or B12 deficiency, without simultaneous vitamin supplementation.Citation38,Citation44
Endocrine insufficiency
Long-standing CP often culminates in brittle diabetes due to progressive destruction of the pancreas, and the clinical management of secondary (apancreatic) diabetes mellitus can be challenging.Citation50 Carbohydrate malabsorption eases glucose intolerance, and the administration of PES may exacerbate diabetes. One randomized controlled trial with PES in patients with apancreatic diabetes revealed major difficulties with controlling blood sugars on changing from active enzyme replacement to placebo and vice versa, suggesting that enzyme adjustment should be carefully supervised in a hospital.Citation16 In another randomized controlled trial of insulin- dependent diabetics with PEI, there were no significant differences in hemoglobin A1C, fasting glucose levels, or 2-hour postprandial glucose levels in patients receiving PES as compared to those not receiving PES.Citation51 A reduction in mild and moderate hypoglycemia was observed in patients receiving PES and the authors concluded that PES therapy can be used safely in patients with diabetes mellitus and exocrine dysfunction.
Effect on incretins
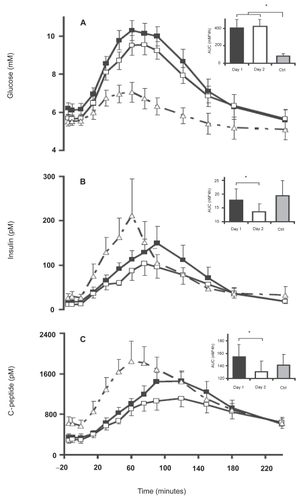
Incretins (mainly GLP-1 (glucagon like peptide-1) and GIP (glucose-dependent insulinotropic polypeptide)) are insulinotropic intestinal peptide hormones released in response to simple carbohydrates and lipids, that cause an increase in the amount of insulin released from the beta cells in the pancreas.Citation52 PES has been shown to restore the GIP response in CP patients.Citation53 An increase in GLP-1 has also been described following PES.Citation54 The increase in incretin levels was accompanied by an increase in plasma insulin and c-peptide levels, but without a significant lowering of plasma glucose levels (). Knop et al concluded that the postprandial response of incretins is preserved in CP patients, and may be enhanced by the increased absorption of nutrients facilitated by pancreatic enzyme replacement.
Figure 2 Plasma glucose (A), plasma insulin (B), and plasma C-peptide (C) concentrations in patients with chronic pancreatitis (CP) and pancreatic exocrine insufficiency (PEI) following ingestion of a liquid meal over 15 min (0–15 min) with pancreatic enzyme substitution (PES; day 1, ▪) and without PES (day 2, □). Punctuated curves (▴) represent healthy control subjects (Ctrl) given an equal liquid meal without PES. Data are mean values ± SE. Insets: AUC values. *Significant difference (p < 0.05). Reproduced with permission from Knop FK, Vilsboll T, Larsen S, et al 2007. Increased postprandial responses of GLP-1 and GIP in patients with chronic pancreatitis and steatorrhea following pancreatic enzyme substitution. Am J Physiol Endocrinol Metab, 292:E324–30. Copyright © 2007 American Physiological Society.
Pharmacology and clinical use of panceatic enzyme supplements
PES preparations
Porcine pancreatic enzymes are the current standard of treatment for PEI, and when protected from exposure to gastric acid, porcine lipase will not be degraded in the stomach. Pancreatin and pancrelipase are the two primary forms of porcine PES available, and pancrelipase has higher enzyme content (see below). Bovine enzymes are a potential alternative for individuals who refuse to consume porcine products for religious or other cultural reasons.Citation55 The bovine preparations, however, contain approximately 75% less lipase activity than the porcine and human preparations, and there is some concern about transmittable pathogens (Foot and mouth disease and Bovine spongiform encephalopathy) from bovine preparations.
Microbial preparations of pancreatic enzymes (lipase, protease, and amylase) also exist.Citation56–Citation59 Certain bacteria (eg, Burkholderia plantarii) and fungi (eg, Aspergillus niger, Rhizopus arrhizus) produce pancreatic enzymes with substantial lipolytic activity and greater resistance to gastric acid degradation. The microbial preparations do not require colipase for activation (see below for the importance of colipase).Citation55 Of the microbial preparations fungal lipase is remarkably stable in the acidic gastric milieu, and is rapidly inactivated by bile acids and proteases whereas bacterial lipase has remarkable stability in both gastric and duodenal milieu, particularly in moderately acidic and neutral pH. In vitro studies have demonstrated bacterial lipase stability against proteases and bile salts and in vivo canine experiments show that bacterial lipase is more potent and efficacious than porcine PES.Citation60–Citation62 The efficacy of bacterial lipases is directly proportional to the fat content in the diet. The coefficient of fat absorption (explained below), which is about 70% with bacterial lipase and a low fat diet increases to about 90% with a high fat meal.Citation58,Citation59
A novel PES product, TheraCLEC-Total (TCT) containing a proprietary formulation of bacterial lipase and fungal protease and amylase, is being developed to aid the digestion of macronutrients.Citation58,Citation59 CF patients with PEI who were treated with TCT experienced improvements in fat and nitrogen absorption, with the greatest improvement in patients with baseline fat absorption of less than 40%. The most commonly reported adverse effects from TCT were mild gastrointestinal disorders and abnormal transaminases. Rarely, more serious pulmonary adverse effects and an episode of intestinal obstruction have also been reported. The mechanisms responsible for these adverse effects are not known.
Human lipase genes have been transfected and expressed using recombinant adenovirus carrier in vitro, ex vivo as well as in vivo. These genes have produced large amounts of human lipase, and in the future, ectopic expression of human lipase in the pancreatobiliary system may become an available treatment modality.Citation63
When to initiate PES
PES should be initiated in patients suffering from CP and steatorrhea. In particular, the greatest benefit is seen in patients who experience weight loss and excrete greater than 15 g of fecal fat per day.Citation64–Citation66 A recent prospective trial was performed where the C-13 medium chain triglyceride breath test was used to optimize PES therapy in CP patients who excrete less than 15 g of fecal fat per day. The results showed a significant improvement in the nutritional status of patients at one year follow up.Citation66 Other indications to consider a trial of PES include patients with idiopathic or small duct CP who suffer from pain unresponsive to other simple treatment measures.
When to administer PES
It is widely accepted that PES should be given at the time of meals. This was demonstrated in 1977, by DiMagno et al who compared two PES administration schedules (hourly administration versus prandial administration) in patients with CP. Prandial administration of PES was more convenient and was as effective as hourly administration in abolishing steatorrhea and perhaps more effective in abolishing azotorrhea.Citation67 A recent prospective crossover randomized controlled trial compared three different prandial administration schedules of enteric coated mini-microspheres (less than 2 mm in diameter) in CP patients with PEI. The schedules were 4 capsules before meals, 4 capsules after meals and 4 capsules during meals (1 before–2 during–1 after meals).Citation17 Fat digestion was optimal when the enzyme preparations were taken during or after meals and was better than the fat digestion observed when capsules were administered just before meals. Interestingly, there was no difference in patient’s preference for the three dosing schedules in this study.
Role of colipase
Normal physiology mandates that colipase, a protein cofactor of lipase, is required in sufficient amounts in the small intestine to digest fat.Citation68 Although devoid of enzymatic activity, colipase promotes pancreatic lipase activity by anchoring the enzyme on the surface of lipid droplets. Isolated colipase deficiency has been demonstrated as a sole cause of steatorrhea in patients with PEICitation69 and is a potential cause of treatment failure in patients receiving PES. All of the PES preparations commercially available in 1992 contained adequate quantities of colipase for effective lipid digestion.Citation70
Role of simultaneous acid supression
The intraduodenal pH in untreated CP patients is acidic due to (1) increased production of gastric acid,Citation71 (2) defective inhibition of gastric acid secretion,Citation72 and (3) impaired secretion of bicarbonate into the duodenum from diseased pancreatic ductal epithelial cells. The resulting acidic intraduodenal milieu is responsible for the irreversible inactivation of pancreatic lipase,Citation73,Citation74 and the decreased functioning of bile salts.Citation64 It has been demonstrated that patient response to conventional PES is enhanced if gastric acid secretion is suppressed.Citation75
The need for additional therapy aimed at increasing intraduodenal pH to improve the response to PES is critical. This is most commonly accomplished using proton pump inhibitors (PPIs) and H2 receptor antagonists. When used concomitantly with ‘conventional’ PES preparations, acid suppression improves the concentration of lipase in the duodenum in patients with PEI.Citation74 The use of acid suppression may appear unnecessary in patients receiving enteric coated forms of PES; however, some studies suggest that acid suppression is still required.Citation76 It should be noted that the release of pancreatic enzymes from the enteric coating is dependent on the intraluminal pH (see section on enteric coated preparations). At the low intraduodenal pH levels seen in CP, dissolution of the coating of these enzymes in the duodenum is, at best, partial with a more complete dissolution occurring distally in the small bowel as the pH rises.Citation15 Patients who receive concomitant acid suppression with enteric coated PES have improved duodenal delivery of PES and more efficient utilization of the absorptive capacity of the intestines.Citation77
Randomized controlled trials have demonstrated a significant improvement in fecal fat excretion with both enteric coated and non enteric coated PES and with simultaneous acid suppression (cimetidine or omeprazole) as compared to PES monotherapy.Citation6,Citation73,Citation77,Citation78 DiMagnoCitation74 concluded that the addition of either H2 receptor antagonists or PPI to an adequate dose of PES will decrease fat malabsorption in most cases. One study suggested that if enteric coated mini-microsphere PES were administered with high dose PPI (omeprazole 60 mg), lower doses (10,000 lipase U tid) of the PES could achieve equal reduction in fecal fat excretion, improvement in abdominal symptom score and general well being when compared to standard (20,000 U tid) doses.Citation79
It should be noted that impaired protein assimilation has been described in patients treated with omeprazole.Citation80 The improvement in fat digestion seen with PES may be at the cost of decreased efficiency of protein digestion with the use of acid suppression. This was demonstrated in a prospective crossover study where the use of acid suppression with PES was associated with a marked decrease in the fat-protein content ratio in stool,Citation81 suggesting an increase in fat absorption with a decrease in protein absorption. This concern should be kept in mind when prescribing acid suppression to patients with PEI.
Enteric coated and micro-encapsulated pancreatic enzyme products
The finding that acid degrades PES is well described.Citation2 Along with the concomitant use of medication to suppress gastric acid, enteric coated PES preparations have been designed to resist degradation in the gastric lumen. The first generation of these preparations was the enteric coated tablet with a diameter of 11–20 mm, which did not show any additional benefit over conventional preparations.Citation82,Citation83 Scintigraphic and breath testing demonstrated poor gastric empyting of these preparations; a finding attributed to the large size of these early enteric coated preparations.Citation84–Citation86
The next generation of enteric coated preparations was coated microspheres. Each particle (over 2 mm in size) in the PES capsule was coated with its own acid resistant coating which was designed to stay intact at a pH of less than 4, and immediately released between a pH of 5.0–5.5, thus theoretically improving duodenal delivery of the PES preparation.
No therapeutic benefit of these preparations was seen, due to failure of the larger microcapsules to exit the stomach with the meal they were intended to accompany, and hence the mini-microsphere (particle size 1–3 mm) was designed.Citation84 The small particle size ensured optimal mixing and synchronous delivery with food. Marked improvement in fat absorption was observed in a randomized controlled trial using mini-microsphere preparations;Citation87 however, in a separate double blind multi-center cross-over study, there was no difference between the enteric coated microspheres and mini-microspheres in patients with PEI.Citation88 Patients, though, preferred the mini-microsphere preparations over the microsphere preparations. Whether the use of these enteric coated mini-microsphere preparations adds any special advantage over the existing therapeutic modalities for the treatment of PEI with CP remains debatable.
The most recent innovation in the formulation of PES has been the development of enteric coated “buffered” microsphere preparations which have 1.5–2.5 mEq of bicarbonate per capsule. Two randomized clinical trials have been conducted comparing these preparations to standard enteric coated microsphere preparations in CF patients with PEI,Citation89,Citation90 only one of which demonstrated reduction in steatorrhea with buffered PES.Citation89
In vitro and in vivo studies have been performed on various commercially available PES preparations.Citation91–Citation93 Although most preparations had similar enzyme composition (ie, the quantity of amylase, lipase and protease), differences in dissolution properties have been observed. For example, even though each preparation tested contained the same amount of lipase, the amount of lipase released as a function of time and pH were found to be different, which was attributed to differences in the physiochemical properties of the enteric coating. The enteric coating may be detrimental to the release of pancreatic enzyme in vivo and may be associated with increased risk of complications (see below). Based on in vitro tests, Aloulou et al propose that the efficacy of enteric coated PES could be enhanced by adding unprotected enzymes. The efficacy of combining unprotected powder enzymes and enteric coated PES was not found to be superior to enteric coated microspheres alone in patients with CF.Citation94 This combination therapy, however, has not been investigated in patients with CP.
Dose and formulation
Since pancreatic steatorrhea does not occur until pancreatic lipase output is decreased by more than 90%,Citation10 the initial dose recommendations for PES is based on achieving 10% of normal postprandial lipolytic activity in the duodenal lumen. Based on these recommendations, the PES preparation must be able to produce 60 IU/min of lipase activity in postprandial chyme throughout the digestive period. A dose of 25–40,000 IU is thus recommended for the digestion of a regular mealCitation55 which may be increased up to 2–3 fold in cases where it appears to lack a therapeutic effect ().
Figure 3 Current standard enzyme treatment of steatorrhea in chronic pancreatitis. Reproduced with permission from Layer P, Keller J. 2003. Lipase supplementation therapy: standards, alternatives, and perspectives. Pancreas, 26:1–7. Copyright © 2003 Lippincott Williams & Wilkins.
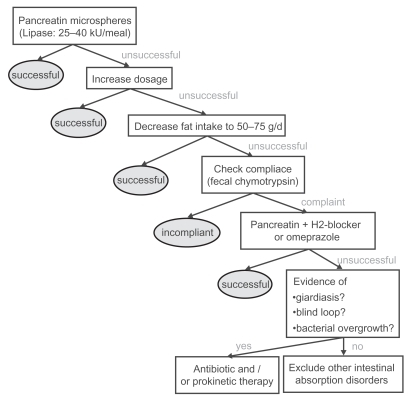
A recent study has suggested that even higher than recommended doses of PES may be needed to digest fats, as the specific activity of human pancreatic lipase on dietary triglycerides was found to be three times less potent in vivo than seen previously under experimental conditions.Citation95 Based on these findings, the authors suggest that higher doses of lipase may be required to completely normalize fat digestion. PES preparations containing higher lipase levels have proven to be more useful than standard preparations in the correction of PEI.Citation96–Citation98 Enteric coated microspheres with increased lipase content are currently available; however, higher doses of PES may cause serious side effects. Fibrosing colonopathy has been described in CF children taking PES, and hence doses greater than 75,000 IU of lipase per meal are not currently recommended (see below).
Dietary interactions
The ingestion of dietary fiber is associated with a small but significant increase in fecal fat excretion in CP patients with PEI.Citation99 Recommending a high fiber diet or fiber supplements in CP patients may be problematic, despite the CP patient’s tendency for constipation due to analgesic use. In addition, alcohol consumption has been noted to decrease lipase activity in CP patients by poorly characterized mechanisms. These levels recover in approximately 6 weeks in patients who abstain from alcohol.Citation100 Therefore it is doubly important that all patients on PES abstain from alcohol.
Calcium and magnesium containing antacids are associated with the formation of calcium and magnesium soaps and the precipitation of glycine conjugated bile salts in the intestine.Citation101 This leads to worsened steatorrhea in patients with PEI and thus such antacids are not recommended.
Treatment failures, patient compliance and alternatives
Lack of patient compliance may be a cause of treatment failure, and can be assessed clinically by measuring fecal chymotrypsin levels.Citation55,Citation102 In compliant patients not responding to PES, increasing the dose of PES by 2–3 fold along with distribution of calories across 5–6 smaller meals is recommended. PES preparations containing higher lipase levels have proven to be more useful for steatorrhea and may be tried in patients who do not respond to standard preparations. Medium chain triglycerides are not recommended as they do not offer any additional improvement in lipid digestion in patients receiving PES.Citation103
Despite drug compliance and adequate dosing, treatment with PES alone in some patients with severe PEI will not lead to clinical improvement. Other factors may be responsible, either separately or in interplay with PEI. Such factors to consider include bacterial overgrowth of the small intestine, inadequate acid suppression, intestinal infections such as giardiasis, or other intestinal absorption disorders. Treatment failures can also occur following the substitution of a preferred brand with the generic formulation of PES. The lack of bioequivalence among different PES preparations is attributed to differences in the physicochemical properties of the enteric coatingCitation104,Citation105 and has been confirmed by in vitro and in vivo studies (see below).
There is no standardized technique to assess treatment adequacy in patients receiving PES. Despite an adequate clinical response of malabsorption and steatorrhea in patients receiving PES, malnutrition may persist. Fecal fat estimation is considered the most reliable measure of fat malabsorption and various techniques ranging from clinical observationCitation106 to the gold standard measures such as the van de Kramer method,Citation107 the near infrared spectrometryCitation108 and Nuclear magnetic Resonance (NMR) spectrometric fecal fat analysisCitation109 have been described. Indices such as the coefficient of fat absorption ((ingested fat – excreted fat)/ingested fat *100), and daily fat excretion (excreted fat/ingested fat * 100) can be derived from dietary and fecal fat estimation. Various other clinical (Body weight, nutritional status, frequency of bowel movements, stool character, abdominal pain, global disease symptom score, quality of life score) as well as laboratory indicators (fecal elastase, fecal chymotrypsin, etc) may be used to test adequacy of PES in various studies. Of the laboratory tests, fecal elastase is a useful non-invasive test for detection of PEI,Citation110–Citation112 but its usefulness in evaluating treatment compliance with PES has not been described.
Another test that has been used in various studies in patients with PEI is the C-13 mixed triglyceride (MTG) breath test.Citation113 It is a highly sensitive, specific, accurate and simple non-invasive test of exocrine pancreatic function with excellent correlation between pancreatic lipase output in the duodenum and the 6-hour cumulative 13CO2 excretion in breath. The C-13 breath test has been used in trials as a measure of adequacy of PES therapy in asymptomatic CP patients and adjustment of PES based on C-13 MTG breath test has been associated with improved nutritional status.Citation77 Thus, improvement in clinical symptoms alone may not accurately predict therapeutic adequacy of PES, and better indicators to insure therapeutic benefit with enzyme supplementation are needed.
In vitro tests
The United States PharmacopoeiaCitation114 has specific guidelines for in vitro assays for enzyme activity as well as dissolution characteristics for PES. The USP guidelines specify that each mg of Pancreatin contains no less than 2 USP units of lipase activity and 25 USP units of amylase and protease activity and each mg of pancrelipase contains no less than 24 USP units of lipase activity and 100 USP units of amylase and protease activity. Each capsule of these preparations should contain between 90% and 165% of the labeled lipase and not less than 90% of labeled activities of amylase and lipaseCitation92 (). The enteric coating of these enzymes is designed such that it remains intact at a pH of less than 4.0 and should dissolve rapidly and completely once the threshold pH (between 5.0 and 5.5 as selected by the manufacturer) is reached.
Table 1 Commercially available pancreatic enzyme (pancrelipase) preparations (Reproduced with permission from Ferrone M, Raimondo M, Scolapio JS. 2007. Pancreatic enzyme pharmacotherapy. Pharmacotherapy, 27:910–20. Copyright © 2007 Pharmacotherapy Publications)
In vitro and in vivo studies have been performed to evaluate the bioequivalence of PES using these recommendations. Citation91–Citation93 All PES products evaluated in these tests were within the USP requirements for levels of amylase, lipase and protease and most preparations had far greater enzyme activity than the lower limit required by the USP. These studies raise the interesting concept of “overfill” seen with PES preparations to allow for enzyme deterioration during storage, so as to prolong “shelf life”. This difference in dissolution properties of the enteric coating (see below) influences the enzyme activity in vitro as observed in these studies, and may be responsible for the observed difference in in vivo potency of the PES preparations.
Food and Drug Administration (FDA) regulations
PES drug product marketing in the United States predates the 1938 passage of the Federal Food, Drug, and Cosmetic Act. These drugs are required on a lifelong basis in patients with PEI to prevent malnutrition and associated complications, and it may be necessary to substitute a preferred product with a different or generic brand in patients with PEI for a variety of reasons. Unfortunately, therapeutic failures (gastrointestinal symptoms and fat malabsorption) have been noted in patients with CF after pharmacists substituted a preferred brand of PES with generic pancrelipase, which rapidly resolved after initial therapy was reinstituted.Citation105
FDA’s review of data and information on pancreatic extract drug productsCitation115 found significant variations in bioavailability among the various dosage forms and among products from different manufacturers of the same dosage form. In the last two decades, the FDA has been making efforts to regulate these inadequacies. On April 28, 2004, the FDA announced that all manufacturers of PES are required to submit a new drug application (NDA) and obtain approval by April 28, 2008, to be able to market these drug products. The approval deadline has recently been deferred until April 28, 2010, if the manufacturers have investigational new drug (IND) applications on active status on or before April 28, 2008, and have submitted an NDA on or before April 28, 2009. With these new requirements, there was only one approved PES preparation. This product Cotazym® (Organon, NJ, USA) was given FDA approval in 1996 but was taken off the market in August 2001.
Adverse effects
Hyperuricemia and hyperuricosuria leading to dysuria and uric acid crystaluria have been described in CF patients receiving PES.Citation116 Allergic reactions to the porcine proteins may also occur.Citation117 A fibrosing colonopathy has been described in children with CF receiving doses of PES above 24,000 U of lipase/kg/day.Citation118 Recent studies have demonstrated that intake of high doses of methacrylic copolymer used as acid resistant coating in PES rather than the lipase itself may be the cause of fibrosing colonopathy.Citation119–Citation121 This condition has also been reported in patients who have never received PES, but rather a different drug coated with methacrylic copolymer.Citation122 Pancreatin extracts are also prone to form insoluble complexes with folic acid, with the result that folic acid deficiency can develop in patients receiving PES. More commonly seen adverse effects include nausea and diarrhea. PES are defined as pregnancy category B drugs, as there is inconclusive evidence for its use in lactation.Citation123
Summary
Patients suffering from CP should be evaluated for the presence of PEI. PES is effective in the correction of steatorrhea and may have a role in reducing pain, improving motility, and correcting malnutrition in these patients. The choice of PES (enteric coated versus non-coated, tablets versus mini-microspheres, etc) and the need for acid suppression should be individualized. There is no current standard test for evaluating adequacy of therapy in CP patients and studies have shown that optimization of therapy based on symptoms alone may be inadequate. Goals of therapy based on overall patient presentation and specific laboratory tests rather than mere correction of steatorrhea are needed. Improved nutritional status is seen in patients receiving pancreatic enzyme replacement therapy, and the use of PES along with other medical and surgical modalities of treatment will significantly improve quality of life of patients with PEI.
Abbreviations
| CP | = | chronic pancreatitis |
| PEI | = | pancreatic exocrine insufficiency |
| PES | = | pancreatic enzyme supplements |
| CF | = | cystic fibrosis |
| PPI | = | proton pump inhibitors |
Disclosures
None of the authors have conflicts of interest to disclose.
References
- RobertsIMPoturichCWaldAUtility of fecal fat concentrations as screening test in pancreatic insufficiencyDig Dis Sci198631102110243757718
- LayerPGoVLDimagnoEPFate of pancreatic enzymes during small intestinal aboral transit in humansAm J Physiol1986251G4754802429560
- HoltmannGKellyDGSternbyBSurvival of human pancreatic enzymes during small bowel transit: effect of nutrients, bile acids, and enzymesAm J Physiol1997273G5535589277437
- ReganPTMalageladaJRDimagnoEPReduced intraluminal bile acid concentrations and fat maldigestion in pancreatic insufficiency: correction by treatmentGastroenterology197977285289447041
- DuttaSKAnandKGadaczTRBile salt malabsorption in pancreatic insufficiency secondary to alcoholic pancreatitisGastroenterology198691124312493758616
- BrunoMJRauwsEAHoekFJComparative effects of adjuvant cimetidine and omeprazole during pancreatic enzyme replacement therapyDig Dis Sci1994399889928174440
- MizushimaTOchiKIchimuraMPancreatic enzyme supplement improves dysmotility in chronic pancreatitis patientsJ Gastroenterol Hepatol2004191005100915304117
- VuMKVechtJEddesEHAntroduodenal motility in chronic pancreatitis: are abnormalities related to exocrine insufficiencyAm J Physiol Gastrointest Liver Physiol2000278G45846610712266
- GielkensHAEddesEHVechtJGallbladder motility and cholecystokinin secretion in chronic pancreatitis: relationship with exocrine pancreatic functionJ Hepatol1997273063129288605
- DimagnoEPGoVLSummerskillWHRelations between pancreatic enzyme ouputs and malabsorption in severe pancreatic insufficiencyN Engl J Med19732888138154693931
- LankischPGLembckeBWemkenGFunctional reserve capacity of the exocrine pancreasDigestion1986351751813781113
- CarriereFGrandvalPGregoryPCDoes the pancreas really produce much more lipase than required for fat digestionJOP2005a620621515883471
- AmmannRWBuehlerHMuenchRDifferences in the natural history of idiopathic (nonalcoholic) and alcoholic chronic pancreatitis. A comparative long-term study of 287 patientsPancreas198723683773628234
- LayerPYamamotoHKalthoffLThe different courses of early- and late-onset idiopathic and alcoholic chronic pancreatitisGastroenterology1994107148114877926511
- GuarnerLRodriguezRGuarnerFFate of oral enzymes in pancreatic insufficiencyGut1993347087128504976
- O’KeefeSJCariemAKLevyMThe exacerbation of pancreatic endocrine dysfunction by potent pancreatic exocrine supplements in patients with chronic pancreatitisJ Clin Gastroenterol20013231932311276275
- Dominguez-MunozJEIglesias-GarciaJIglesias-ReyMEffect of the administration schedule on the therapeutic efficacy of oral pancreatic enzyme supplements in patients with exocrine pancreatic insufficiency: a randomized, three-way crossover studyAliment Pharmacol Ther200521993100015813835
- SafdiMBekalPKMartinSThe effects of oral pancreatic enzymes (Creon 10 capsule) on steatorrhea: a multicenter, placebo-controlled, parallel group trial in subjects with chronic pancreatitisPancreas20063315616216868481
- CzakóLTakácsTHegyiPQuality of life assessment after pancreatic enzyme replacement therapy in chronic pancreatitisCan J Gastroenterol20031759760314571298
- VuoristoMVaananenHMiettinenTACholesterol malabsorption in pancreatic insufficiency: effects of enzyme substitutionGastroenterology19921026476551732134
- FolschURCantorPWilmsHMRole of cholecystokinin in the negative feedback control of pancreatic enzyme secretion in conscious ratsGastroenterology1987924499582431952
- OwyangCNegative feedback control of exocrine pancreatic secretion: role of cholecystokinin and cholinergic pathwayJ Nutr19941241321S1326S7914921
- BozkurtTAdlerGKoopIPlasma CCK levels in patients with pancreatic insufficiencyDig Dis Sci1988332762813342719
- JansenJBHopmanWPLamersCBPlasma cholecystokinin concentrations in patients with pancreatic insufficiency measured by sequence-specific radioimmunoassaysDig Dis Sci198429110911176499629
- IsakssonGIhseIPain reduction by an oral pancreatic enzyme preparation in chronic pancreatitisDig Dis Sci198328971026825540
- SlaffJJacobsonDTillmanCRProtease-specific suppression of pancreatic exocrine secretionGastroenterology19848744526202586
- HalgreenHPedersenNTWorningHSymptomatic effect of pancreatic enzyme therapy in patients with chronic pancreatitisScand J Gastroenterol1986211041083633631
- MalesciAGaiaEFiorettaANo effect of long-term treatment with pancreatic extract on recurrent abdominal pain in patients with chronic pancreatitisScand J Gastroenterol1995303923987610357
- MossnerJPalliation of pain in chronic pancreatitis. Use of enzymesSurg Clin North Am199979861872xi10470332
- BrownAHughesMTennerSDoes pancreatic enzyme supplementation reduce pain in patients with chronic pancreatitis: a meta-analysisAm J Gastroenterol199792203220359362186
- GreenbergerNJEnzymatic therapy in patients with chronic pancreatitisGastroenterol Clin North Am19992868769310503144
- RosaESLTronconLEGalloLJRFactors associated with abnormal gastric emptying in alcohol-related chronic pancreatitisJ Clin Gastroenterol20074130631117426472
- LongWBWeissJBRapid gastric emptying of fatty meals in pancreatic insufficiencyGastroenterology1974679209254609827
- NustedeRKohlerHFolschURPlasma concentrations of neuro-tensin and CCK in patients with chronic pancreatitis with and without enzyme substitutionPancreas199162602651713670
- LayerPVon Der OheMRHolstJJAltered postprandial motility in chronic pancreatitis: role of malabsorptionGastroenterology1997112162416349136842
- MascleeAAJansenJBCorstensFHReversible gall bladder dysfunction in severe pancreatic insufficiencyGut1989308668722753411
- GlasbrennerBMalfertheinerPPieramicoOGallbladder dynamics in chronic pancreatitis. Relationship to exocrine pancreatic function, CCK, and PP releaseDig Dis Sci1993384824898444080
- DuttaSKBustinMPRussellRMDeficiency of fat-soluble vitamins in treated patients with pancreatic insufficiencyAnn Intern Med1982975495526922690
- MarottaFLabadariosDFrazerLFat-soluble vitamin concentration in chronic alcohol-induced pancreatitis. Relationship with steatorrheaDig Dis Sci1994399939988174441
- NakamuraTTakebeKImamuraKFat-soluble vitamins in patients with chronic pancreatitis (pancreatic insufficiency)Acta Gastroenterol Belg19965910148686411
- MoranCESosaEGMartinezSMBone mineral density in patients with pancreatic insufficiency and steatorrheaAm J Gastroenterol1997928678719149203
- HaaberABRosenfalckAMHansenBBone mineral metabolism, bone mineral density, and body composition in patients with chronic pancreatitis and pancreatic exocrine insufficiencyInt J Pancreatol200027212710811020
- MannSTStrackeHLangeUAlterations of bone mineral density and bone metabolism in patients with various grades of chronic pancreatitisMetabolism20035257958512759887
- Bang JorgensenBThorsgaard PedersenNWorningHShort report: lipid and vitamin B12 malassimilation in pancreatic insufficiencyAliment Pharmacol Ther199152072101888821
- MontaltoGSoresiMCarroccioALipoproteins and chronic pancreatitisPancreas199491371388108368
- TuzhilinDADreilingDACardiovascular lesions in pancreatitisAm J Gastroenterol1975633813881146795
- GulloLStellaALabriolaECardiovascular lesions in chronic pancreatitis: a prospective studyDig Dis Sci1982277167227094792
- TrolliPAConwellDLZuccaroGJRPancreatic enzyme therapy and nutritional status of outpatients with chronic pancreatitisGastroenterol Nurs200124848711847733
- Dominguez-MunozJEPancreatic enzyme therapy for pancreatic exocrine insufficiencyCurr Gastroenterol Rep2007911612217418056
- AndersenDKMechanisms and emerging treatments of the metabolic complications of chronic pancreatitisPancreas20073511517575539
- EwaldNBretzelRGFantusIGPancreatin therapy in patients with insulin-treated diabetes mellitus and exocrine pancreatic insufficiency according to low fecal elastase 1 concentrations. Results of a prospective multi-centre trialDiabetes Metab Res Rev20072338639117103488
- CreutzfeldtWThe [pre-] history of the incretin conceptRegul Pept2005128879115780427
- EbertRCreutzfeldtWReversal of impaired GIP and insulin secretion in patients with pancreatogenic steatorrhea following enzyme substitutionDiabetologia1980191982046997121
- KnopFKVilsbollTLarsenSIncreased postprandial responses of GLP-1 and GIP in patients with chronic pancreatitis and steatorrhea following pancreatic enzyme substitutionAm J Physiol Endocrinol Metab2007292E32433016954337
- LayerPKellerJLipase supplementation therapy: standards, alternatives, and perspectivesPancreas2003261712499909
- MoreauJBouissonMSaint-Marc-GirardinMFComparison of fungal lipase and pancreatic lipase in exocrine pancreatic insufficiency in man. Study of their in vitro properties and intraduodenal bioavailabilityGastroenterol Clin Biol1988127877923220231
- Zentler-MunroPLAssoufiBABalasubramanianKTherapeutic potential and clinical efficacy of acid-resistant fungal lipase in the treatment of pancreatic steatorrhoea due to cystic fibrosisPancreas199273113191594552
- BorowitzDGossCHLimauroSStudy of a novel pancreatic enzyme replacement therapy in pancreatic insufficient subjects with cystic fibrosisJ Pediatr2006a14965866217095338
- BorowitzDGossCHStevensCSafety and preliminary clinical activity of a novel pancreatic enzyme preparation in pancreatic insufficient cystic fibrosis patientsPancreas2006b3225826316628080
- RaimondoMDimagnoEPLipolytic activity of bacterial lipase survives better than that of porcine lipase in human gastric and duodenal contentGastroenterology19941072312358020666
- SuzukiAMizumotoASarrMGBacterial lipase and high-fat diets in canine exocrine pancreatic insufficiency: a new therapy of steatorrheaGastroenterology1997112204820559178698
- SuzukiAMizumotoARerknimitrREffect of bacterial or porcine lipase with low- or high-fat diets on nutrient absorption in pancreatic-insufficient dogsGastroenterology19991164314379922325
- KuhelDGZhengSTsoPAdenovirus-mediated human pancreatic lipase gene transfer to rat bile: gene therapy of fat malabsorptionAm J Physiol Gastrointest Liver Physiol2000279G1031103611053001
- BrunoMJHaverkortEBTytgatGNMaldigestion associated with exocrine pancreatic insufficiency: implications of gastrointestinal physiology and properties of enzyme preparations for a cause-related and patient-tailored treatmentAm J Gastroenterol199590138313937661155
- LayerPKellerJLankischPGPancreatic enzyme replacement therapyCurr Gastroenterol Rep2001310110811276376
- Dominguez-MunozJEIglesias-GarciaJVilarino-InsuaM13C-mixed triglyceride breath test to assess oral enzyme substitution therapy in patients with chronic pancreatitisClin Gastroenterol Hepatol2007548448817445754
- DimagnoEPMalageladaJRGoVLFate of orally ingested enzymes in pancreatic insufficiency. Comparison of two dosage schedulesN Engl J Med19772961318132216213
- BrockmanHLKinetic behavior of the pancreatic lipase-colipase-lipid systemBiochimie20008298799511099795
- GaskinKJDuriePRLeeLColipase and lipase secretion in childhood-onset pancreatic insufficiency. Delineation of patients with steatorrhea secondary to relative colipase deficiencyGastroenterology198486176689652
- Erlanson-AlbertssonCWisenOEnzyme substitution in pancreatic disease: is colipase activity sufficientScand J Gastroenterol1992271081101561522
- GulloLGastric acid secretion in chronic pancreatitisHepatogastoenterology1983306062
- SaundersJHCargillJMWormsleyKGGastric secretion of acid in patients with pancreatic diseaseDigestion197817365369669079
- ReganPTMalageladaJRDimagnoEPComparative effects of antacids, cimetidine and enteric coating on the therapeutic response to oral enzymes in severe pancreatic insufficiencyN Engl J Med197729785485820572
- DimagnoEPGastric acid suppression and treatment of severe exocrine pancreatic insufficiencyBest Pract Res Clin Gastroenterol20011547748611403540
- GrahamDYPancreatic enzyme replacement: the effect of antacids or cimetidineDig Dis Sci1982274854906282548
- FranciscoMPWagnerMHShermanJMRanitidine and omeprazole as adjuvant therapy to pancrelipase to improve fat absorption in patients with cystic fibrosisJ Pediatr Gastroenterol Nutr200235798312142815
- SaundersJHDrummondSWormsleyKGInhibition of gastric secretion in treatment of pancreatic insufficiencyBr Med J1977141841913906
- Dominguez-MunozJEIglesias-GarciaJIglesias-ReyMOptimising the therapy of exocrine pancreatic insufficiency by the association of a proton pump inhibitor to enteric coated pancreatic extractsGut2006551056105716766768
- VechtJSymerskyTLamersCBEfficacy of lower than standard doses of pancreatic enzyme supplementation therapy during acid inhibition in patients with pancreatic exocrine insufficiencyJ Clin Gastroenterol20064072172516940886
- EvenepoelPClausDGeypensBEvidence for impaired assimilation and increased colonic fermentation of protein, related to gastric acid suppression therapyAliment Pharmacol Ther199812101110199798807
- DelhayeMMeurisSGohimontACComparative evaluation of a high lipase pancreatic enzyme preparation and a standard pancreatic supplement for treating exocrine pancreatic insufficiency in chronic pancreatitisEur J Gastroenterol Hepatol199686997038853261
- GrahamDYEnzyme replacement therapy of exocrine pancreatic insufficiency in man. Relations between in vitro enzyme activities and in vivo potency in commercial pancreatic extractsN Engl J Med19772961314131716212
- DuttaSKRubinJHarveyJComparative evaluation of the therapeutic efficacy of a pH-sensitive enteric coated pancreatic enzyme preparation with conventional pancreatic enzyme therapy in the treatment of exocrine pancreatic insufficiencyGastroenterology1983844764826549746
- MeyerJHElashoffJPorter-FinkVHuman postprandial gastric emptying of 1-3-millimeter spheresGastroenterology198894131513253360258
- MeyerJHLakeRMismatch of duodenal deliveries of dietary fat and pancreatin from enterically coated microspheresPancreas1997152262359336785
- BrunoMJBormJJHoekFJGastric transit and pharmacodynamics of a two-millimeter enteric-coated pancreatin microsphere preparation in patients with chronic pancreatitisDig Dis Sci1998432032139508526
- SternRCEisenbergJDWagenerJSA comparison of the efficacy and tolerance of pancrelipase and placebo in the treatment of steatorrhea in cystic fibrosis patients with clinical exocrine pancreatic insufficiencyAm J Gastroenterol2000951932193810950038
- HalmULoserCLohrMA double-blind, randomized, multicentre, crossover study to prove equivalence of pancreatin minimicrospheres versus microspheres in exocrine pancreatic insufficiencyAliment Pharmacol Ther19991395195710383531
- BradyMSGarsonJLKrugSKAn enteric-coated high-buffered pancrelipase reduces steatorrhea in patients with cystic fibrosis: a prospective, randomized studyJ Am Diet Assoc20061061181118616863712
- KalninsDEllisLCoreyMEnteric-coated pancreatic enzyme with bicarbonate is equal to standard enteric-coated enzyme in treating malabsorption in cystic fibrosisJ Pediatr Gastroenterol Nutr20064225626116540792
- KraisingerMHochhausGStecenkoAClinical pharmacology of pancreatic enzymes in patients with cystic fibrosis and in vitro performance of microencapsulated formulationsJ Clin Pharmacol1994341581668163716
- CaseCLHennigesFBarkinJSEnzyme content and acid stability of enteric-coated pancreatic enzyme products in vitroPancreas20053018018315714141
- AloulouAPuccinelliDSarlesJIn vitro comparative study of three pancreatic enzyme preparations: dissolution profiles, active enzyme release and acid stabilityAliment Pharmacol Ther20082728329217973644
- KalninsDCoreyMEllisLCombining unprotected pancreatic enzymes with pH-sensitive enteric-coated microspheres does not improve nutrient digestion in patients with cystic fibrosisJ Pediatr200514648949315812451
- CarriereFGrandvalPRenouCQuantitative study of digestive enzyme secretion and gastrointestinal lipolysis in chronic pancreatitisClin Gastroenterol Hepatol2005b3283815645402
- GanKHHeijermanHGGeusWPComparison of a high lipase pancreatic enzyme extract with a regular pancreatin preparation in adult cystic fibrosis patientsAliment Pharmacol Ther199486036077696449
- MalesciAMarianiAMezziGNew enteric-coated high-lipase pancreatic extract in the treatment of pancreatic steatorrheaJ Clin Gastroenterol19941832358113582
- GulloLMedical treatment of chronic pancreatitisAnn Ital Chir200071333710829521
- RogginGMIberFLLinscheerWGIntraluminal fat digestion in the chronic alcoholicGut1972131071115045703
- DuttaSKHlaskoJDietary fiber in pancreatic disease: effect of high fiber diet on fat malabsorption in pancreatic insufficiency and in vitro study of the interaction of dietary fiber with pancreatic enzymesAm J Clin Nutr1985415175252579539
- GrahamDYSackmanJWMechanism of increase in steatorrhea with calcium and magnesium in exocrine pancreatic insufficiency: an animal modelGastroenterology1982836386447095367
- LankischPGWhat to do when a patient with exocrine pancreatic insufficiency does not respond to pancreatic enzyme substitution, a practical guideDigestion199960Suppl 19710310026441
- CaliariSBeniniLSembeniniCMedium-chain triglyceride absorption in patients with pancreatic insufficiencyScand J Gastroenterol19963190948927947
- HendelesLDorfAStecenkoATreatment failure after substitution of generic pancrelipase capsules. Correlation with in vitro lipase activityJAMA1990263245924612329633
- HendelesLHochhausGKazerounianSGeneric and alternative brand-name pharmaceutical equivalents: select with cautionAm J Hosp Pharm1993503233298480793
- LankischPGDrögeMHofsesSSteatorrhoea: you cannot trust your eyes when it comes to diagnosisLancet1996347162016218667884
- Van De KamerJHTen Bokkel HuininkHWeyersHARapid method for the determination of fat in fecesJ Biol Chem194917734735518107439
- BeniniLCaliariSGuidiGCNear infrared spectrometry for faecal fat measurement: comparison with conventional gravimetric and titrimetric methodsGut198930134413472583563
- SchneiderMUDemlingLDomschkeSNMR spectrometric stool fat analysis – a new technique for quantifying steatorrhea and establishing the indication for enzyme replacement in chronic pancreatitisHepatogastroenterology1985322102152414199
- LoserCMollgaardAFolschURFaecal elastase 1: a novel, highly sensitive, and specific tubeless pancreatic function testGut1996395805868944569
- SonwalkarSAHolbrookIBPhillipsIA prospective, comparative study of the para-aminobenzoic acid test and faecal elastase 1 in the assessment of exocrine pancreatic functionAliment Pharmacol Ther20031746747112562462
- NaruseSIshiguroHKoSBFecal pancreatic elastase: a reproducible marker for severe exocrine pancreatic insufficiencyJ Gastroenterol20064190190817048055
- VantrappenGRRutgeertsPJGhoosYFMixed triglyceride breath test: a noninvasive test of pancreatic lipase activity in the duodenumGastroenterology198996112611342494097
- USPPancrelipase: Official MonographThe United States Pharmacopeia, The National FormularyThe United States Pharmacoepia Convention17(ed.)Rockville, MD1989
- CDERGuidelines for IndustryExocrine pancreatic Insufficiency Drug Products – Submitting NDAsCenter or Drug Evaluation and Research, Food and Drug Administration, US Department of Health and Human Services2006
- StapletonFBKennedyJNousia-ArvanitakisSHyperuricosuria due to high-dose pancreatic extract therapy in cystic fibrosisN Engl J Med1976295246248934188
- PitchumoniCSChronic pancreatitis: pathogenesis and management of painJ Clin Gastroenterol1998271011079754770
- FitzsimmonsSCBurkhartGABorowitzDHigh-dose pancreatic-enzyme supplements and fibrosing colonopathy in children with cystic fibrosisN Engl J Med1997336128312899113931
- Van VelzenDBallLMDezfulianARComparative and experimental pathology of fibrosing colonopathyPostgrad Med J199672Suppl 2S39S48 discussion S49–S518869182
- PrescottPPancreatic enzymes and fibrosing colonopathyLancet199935425010421323
- PrescottPBakowskiMTPathogenesis of fibrosing colonopathy: the role of methacrylic acid copolymerPharmacoepidemiol Drug Saf1999837738415073899
- GaiaESambatoroADe GiuliPAdult fibrosing colonopathy associated with mesalazine treatmentAm J Gastroenterol2001962508250911513205
- FerroneMRaimondoMScolapioJSPancreatic enzyme pharmacotherapyPharmacotherapy20072791092017542772