Abstract
Gastroesophageal reflux disease (GERD) is a chronic, relapsing disease that can progress to major complications. Affected patients have poorer health-related quality of life than the general population. As GERD requires continued therapy to prevent relapse and complications, most patients with erosive esophagitis require long-term acid suppressive treatment. Thus GERD results in a significant cost burden and poor health-related quality of life. The effective treatment of GERD provides symptom resolution and high rates of remission in erosive esophagitis, lowers the incidence of GERD complications, improves health-related quality of life, and reduces the cost of this disease. Proton pump inhibitors are accepted as the most effective initial and maintenance treatment for GERD. Oral pantoprazole is a safe, well tolerated and effective initial and maintenance treatment for patients with nonerosive GERD or erosive esophagitis. Oral pantoprazole has greater efficacy than histamine H2-receptor antagonists and generally similar efficacy to other proton pump inhibitors for the initial and maintenance treatment of GERD. In addition, oral pantoprazole has been shown to improve the quality of life of patients with GERD and is associated with high levels of patient satisfaction with therapy. GERD appears to be more common and more severe in the elderly, and pantoprazole has shown to be an effective treatment for this at-risk population.
Introduction
Gastroesophageal reflux disease (GERD) is a chronic, relapsing disease that infrequently progresses (CitationSontag et al 2006) but is associated with a range of potentially serious esophageal complications (esophageal ulcer, esophageal stricture or obstruction, Barrett’s esophagus or esophageal cancer) and extra-esophageal diseases such as respiratory problems, chest pain, angina, and increased mortality (CitationRuigomez et al 2004). It is characterized by reflux of the stomach contents into the esophagus, oropharynx, larynx, or airway and is associated with heartburn, acid regurgitation, and dyspepsia (CitationDent et al 1999; CitationFarup et al 2001a; CitationShaker et al 2003; CitationOrlando 2006). Other less common symptoms of GERD include cough, intermittent wheezing, vocal cord inflammation, atypical chest pain, dysphagia, and hoarseness. Simply put, GERD has been defined as “a condition which develops when the reflux of stomach contents causes troublesome symptoms and/or complications” (CitationVakil et al 2006).
Gastroesophageal reflux disease is one of the most common chronic gastrointestinal disorders (CitationHaag and Holtmann 2003). It has been reported that GERD affects an estimated 19 million individuals in the US (CitationSandler et al 2002), and it can affect up to one-third of adults (CitationHaag and Holtmann 2003). These figures are likely to underestimate the true prevalence of GERD, since many patients self-medicate and do not seek medical advice or diagnosis (CitationFendrick 2001). Similarly, many patients are not aware that they have GERD (CitationHollenz et al 2002). Failure to seek professional medical treatment can lead physicians to under-diagnose and under-treat GERD, with consequent poor control of symptoms, lost productivity, reduced quality of life, and an increased incidence of complications in affected patients. Ultimately, this under-diagnosis and under-treatment result in increased long-term healthcare utilization and costs.
This article provides an overview of GERD and the issues that must be considered during the long-term management of the disease; literature concerning the long-term treatment of GERD with the proton pump inhibitor (PPI) pantoprazole is then reviewed.
Long-term management issues in GERD
In healthy individuals, reflux of gastric contents occurs naturally without causing esophageal damage. However, in susceptible individuals, esophageal exposure to gastric contents causes either microscopic or macroscopic mucosal defects and the symptom of heartburn (CitationOrlando 2006). The exact pathologic process by which this occurs is complex and yet to be fully characterized, but there are two requirements for heartburn, regardless of a diagnosis of erosive or nonerosive disease: these are high concentrations of acid within the esophageal lumen (reflux) and a damaged esophageal epithelium. When these situations co-exist, luminal acid enters the tissue where stimulation of nociceptors results in the symptom of heartburn (CitationOrlando 2006). The major determinants of the severity of esophageal damage are the degree and duration of esophageal acid exposure in patients with impaired esophageal defenses (including increased frequency and duration of transient relaxations of the lower esophageal sphincter, impaired motility, decreased mucosal resistance, delayed gastric emptying, and presence of hiatus hernia) (CitationRai and Orlando 1998; CitationVan Herwaarden et al 2000). In patients with nonerosive GERD, mucosal breaks are only apparent microscopically and are characterized by the presence of dilated intercellular spaces, whereas in patients with erosive esophagitis, breaks in the esophageal epithelium are visible on endoscopy. Nonerosive GERD can progress to erosive disease in susceptible patients (CitationOrlando 2006) although initial severity of GERD is maintained in most patients (CitationVakil et al 2006). Erosive esophagitis is a chronic, recurring disease that can lead to further complications such as ulceration if long-term management is ineffective; secondary fibrosis and scarring can infrequently lead to esophageal stricture (CitationOrlando 1999; CitationSontag et al 2006; CitationVakil et al 2006). A 20-year follow-up of 2306 patients who received symptom-driven antireflux treatment indicated that only one patient with a normal baseline mucosa developed esophageal stricture requiring dilation (0.08%), but that 18 patients with an erosive baseline mucosa were affected (1.9%). The overall incidence of stricture in patients with GERD was <1/1,000 per year (CitationSontag et al 2006).
With time, patients with GERD may develop histopathological changes such as Barrett’s esophagus (CitationSpechler and Goyal 1986). GERD and Barrett’s esophagus are significant risk factors for esophageal adenocarcinoma (CitationLassen et al 2006; CitationVakil et al 2006), the incidence of which has increased in Western industrialized nations over the last two decades (CitationBollschweiler et al 2001). In 2002, the incidence of esophageal adenocarcinoma was 26 per 100 000 person-years among patients with previously diagnosed erosive esophagitis (versus 2.79 per 100 000 person-years in the general population) in a Danish community (CitationLassen et al 2006). The risk of this life-threatening cancer is greatest in patients with more severe, frequent, and prolonged symptoms of GERD (CitationLagergren et al 1999). Severe GERD (GERD characterized by erosions, ulcers, and strictures) occurs more frequently in men, the elderly, and those of white ethnicity than in other populations (CitationEl-Serag and Sonnenberg 1997). Infection with Helicobacter pylori does not appear to contribute to the development of GERD (CitationCsendes et al 1997; CitationLabenz and Malfertheiner 1997; CitationRaghunath et al 2003; CitationSharma and Vakil 2003).
Diagnosis
The differential diagnosis of GERD is often difficult. The intensity and frequency of heartburn and other symptoms of GERD are poor predictors of the presence or severity of esophageal manifestations (CitationJohansson et al 1986; CitationGreen 1993; CitationFennerty et al 2002) meaning that symptom assessment alone is not a reliable method to assess the presence or severity of erosive disease (CitationDent et al 1999; CitationJohnson and Fennerty 2004). However, since objective testing is not common in primary practice, it has been suggested that GERD is likely when heartburn occurs on two or more days a week, although less frequent symptoms do not preclude disease (CitationDent et al 1999).
Initiation of empiric therapy with acid suppressive therapy, usually a PPI, in patients with symptoms consistent with GERD is an efficient and acceptable method to confirm GERD; this method lacks specificity (CitationNumans et al 2004). If symptoms are relieved by therapy, a diagnosis of GERD can be assumed (CitationDeVault and Castell 1999; CitationFass et al 1999, Citation2000; CitationHabermann et al 2002). GERD can also be diagnosed using 24-hour pH monitoring, but this test has limitations because there is no direct information as to the extent of esophageal damage (CitationArango et al 2000). Additional confirmatory diagnostic tests include endoscopy, biopsy, barium radiography, examination of the throat and larynx, esophageal motility testing, emptying studies of the stomach, and esophageal acid perfusion. Of these tests, endoscopy is the only reliable method to diagnose erosive esophagitis and determine its severity (CitationTefera et al 1997).
Aims of treatment
The main aim of GERD treatment should be rapid and sustained achievement of comprehensive symptom resolution, because this is associated with marked improvement—often normalization—in health-related quality of life (CitationRevicki et al 1999). The other primary aims are to heal esophageal mucosal damage if it is present and to prevent relapse of erosive esophagitis in the hope that this will reduce the development of other serious complications.
Adequate treatment of GERD should either prevent repeated reflux of gastric contents into the esophagus or reduce the damaging effect of gastric acid. As no pharmaceutical agent can fully correct the motor dysfunction responsible for acid reflux into the esophagus, acid suppression remains the most effective way to relieve symptoms and to promote healing of esophagitis in patients with GERD (CitationOrlando 1997).
Treatment options
A number of pharmacological and surgical treatment options are available for patients with GERD. For most patients, initial acid suppressive therapy with a PPI is recommended. Once healing is achieved, the majority of patients with erosive esophagitis will require continued long-term (maintenance) acid suppressive treatment, usually with a lower dosage of their initial acid-suppressive therapy. This is because GERD is a chronic, usually lifelong disease that often relapses once treatment is stopped. In fact, relapse rates of 81% to 90% have been reported in patients with healed erosive esophagitis 6 to 12 months after drug therapy was withdrawn (CitationHetzel et al 1988; CitationChiba 1997; CitationCarlsson et al 1998) and it is generally accepted that symptoms will persist in most patients (CitationVakil et al 2006).
Pharmacological options
The main acid suppressive agents available for patients with GERD are antacids, H2-receptor antagonists, and PPIs. Antacids do not usually provide sufficient acid suppression for patients with GERD. H2-receptor antagonists decrease gastric acid secretion by competitive and reversible blockade of histamine H2-receptors on the parietal cells of the gastric mucosa. H2-receptor antagonists are significantly more effective than antacids for suppressing acid secretion, but have a slower onset of action (CitationNetzer et al 1998; CitationWyeth et al 1998). Use of H2-receptor antagonist is limited by drug tolerance, which can result in about a 50% reduction in efficacy that cannot be reversed by dose increases (CitationNwokolo et al 1990; CitationKahrilas et al 1999). Over-the-counter preparations of low-dose H2-receptor antagonists (cimetidine, famotidine, nizatidine, and ranitidine) are also available. These are relatively safe, but are not effective in the vast majority of patients (CitationShaw et al 2001).
Proton pump inhibitors are widely recognized as the most effective agents for treating GERD. They are the mainstay of initial GERD management (CitationDeVault and Castell 1999) and are the preferred agents for maintenance therapy in patients with healed erosive esophagitis (CitationDeVault and Castell 1999; CitationCrawley and Maclin Schmitt 2000). PPIs provide more rapid symptom control and better healing of erosive esophagitis than both H2-receptor antagonists and antacids (CitationChiba et al 1997; CitationDent et al 1999; CitationDeVault and Castell 1999; CitationCaro et al 2001; CitationDonnellan et al 2004).
Proton pump inhibitors block the final step in the secretion of hydrochloric acid by binding to and inactivating H+/K+ATPase in parietal cells of the gastric mucosa (CitationBell and Hunt 1992; CitationSachs 1997). PPIs thus produce a considerable but dose-dependent elevation of gastric pH (CitationDajani 2000). The prolonged hypochlorhydria seen with PPI therapy has raised safety concerns for patients receiving long-term therapy with these agents (possible enterochromaffin-like cell hyperplasia and gastric carcinoids, colorectal adenocarcinoma and polyps, and bacterial overgrowth as a result of achlorhydria). However, the magnitude of hypergastrinemia associated with PPI use is similar to that observed after vagotomy, and is 3-to 6-fold lower than that observed with pernicious anemia. Evidence to date indicates that any morphological changes in gastric endocrine cells are minimal, self-limiting, nondysplastic and non-neoplastic, suggesting that hypergastrinemia observed during PPI therapy has little clinical significance (CitationFreston 1997). Thus, monitoring of serum gastrin levels and fundic enterochromaffin-like cells is of no clinical relevance even during long-term therapy with PPIs (CitationArnold 1994). PPIs are associated with a low rate of drug-drug reactions, other than those expected by the lowering of intragastric pH (CitationLabenz et al 2003; CitationRobinson and Horn 2003). Of the PPIs, omeprazole has the highest risk for hepatic-based interactions, and rabeprazole and pantoprazole appear to have the lowest risk (CitationRobinson and Horn 2003). Of these lower risk agents, pantoprazole is the only PPI with a well characterized interaction profile (CitationBlume et al 2006).
Surgery
Although surgery (open, endoscopic, or laparoscopic) is an option for some patients with GERD, the outcomes of corrective procedures vary widely depending on the experience and skill of the surgeon (CitationWatson et al 1996; CitationJohnson 2003). Surgery is not an ideal option for the majority of patients, and many patients will continue to use acid reducing medications on a regular basis after undergoing surgery (CitationSpechler et al 2001; CitationJohnson 2003). In comparison with pharmacotherapy in the US, surgical antireflux therapy (open Nissen fundoplication) produces no significant differences in grade of esophagitis, frequency of treatment of esophageal stricture, and subsequent antireflux operations, incidence of esophageal cancer, quality of life measures, and overall satisfaction with antireflux therapy when assessed more than 9 years after initiation of therapy (CitationSpechler et al 2001). Similarly, in Europe, PPI therapy demonstrates similar efficacy to open antireflux surgery in terms of prevalence of Barrett’s esophagus or strictures requiring dilatation, incidence of GERD-associated symptoms or quality of life at 3 years’ follow up (CitationLundell et al 2000), but after 5 years is associated with lower total medical costs (operation, endoscopy, visits to the outpatient clinic, and medication) for chronic GERD (CitationMyrvold et al 2001). Laparoscopic fundoplication is not without complications: surgical complications such as gastric perforation or hernia can occur; medical therapy is required for control of heartburn in approximately one third of patients after this procedure; and new gastric symptoms are common after surgery (CitationVakil et al 2003).
Efficacy, safety, and tolerability of pantoprazole
Efficacy
Initial therapy
Oral pantoprazole is an effective treatment option for the initial treatment of nonerosive GERD or erosive esophagitis. It is most effective for healing erosive esophagitis when administered at a dose of 40 mg once daily (Citationvan Rensburg et al 1996; CitationRichter and Bochenek 2000).
In patients with endoscopically confirmed mild to severe erosive esophagitis, oral pantoprazole 20 mg/day or 40 mg/day is more effective for healing of erosions and relief of GERD symptoms than the H2-receptor antagonists with which it has been compared (CitationCheer et al 2003; CitationBochenek et al 2004) and generally has similar efficacy to other PPIs on a mg per mg basis (CitationCheer et al 2003; CitationScholten et al 2003; CitationGillessen et al 2004; CitationAchim et al 2005; CitationGlatzel et al 2006). Oral pantoprazole 20 mg daily also provided clinical improvement in symptoms of erosive esophagitis in children aged 6 to 13 years enrolled in a small uncontrolled trial (CitationMadrazo-de la Garza et al 2003). These latter findings are supported by the results of two recently completed studies. In these studies, oral pantoprazole at doses of 20 mg and 40 mg once daily for 8 weeks rapidly reduced symptom scores in 53 children aged 5 to 11 years with erosive or histological esophagitis (p < 0.001) (CitationTolia et al 2006) and in 136 adolescents aged 12 to 16 years with clinically diagnosed GERD (p < 0.001) (CitationTsou et al 2006). Pantoprazole 10 mg daily also produced significant improvement in symptoms, but was not as effective as the higher doses in children (CitationTolia et al 2006).
Maintenance therapy
Pantoprazole 20 mg or 40 mg daily as maintenance therapy prevents relapse of erosive esophagitis for 6 to 24 months in most patients with healed disease (CitationMossner et al 1997; CitationEscourrou et al 1999; CitationVan Rensburg et al 1999; CitationPlein et al 2000), regardless of patients’ initial disease severity (CitationMetz and Bochenek 2003; CitationRichter et al 2004). Pantoprazole 20 mg once daily has generally shown similar efficacy for preventing endoscopic or symptomatic relapse to pantoprazole 40 mg once daily (CitationEscourrou et al 1999; CitationPlein et al 2000). In the larger of the two trials designed to statistically compare these pantoprazole regimens, daily doses of 20 mg and 40 mg maintained 75% and 78% of patients, respectively, in endoscopic remission after 12 months, with Savary-Miller stage I disease accounting for about 50% of the endoscopic relapses (CitationPlein et al 2000). Symptomatic remission rates after 12 months were also similar with each pantoprazole regimen: 77% with the 20 mg dose and 76% with the 40 mg dose. No correlation was seen between endoscopic relapse and perception of symptoms, or between the baseline severity of GERD and the maintenance dose of pantoprazole (CitationPlein et al 2000). However, in two dose-ranging comparisons with ranitidine, patients receiving pantoprazole 40 mg daily were significantly more likely to remain in remission than patients receiving pantoprazole 20 mg daily (p < 0.03 and p < 0.001) () (CitationMetz and Bochenek 2003; CitationRichter et al 2004).
Table 1 Randomized clinical trials comparing the efficacy of maintenance therapy with pantoprazole versus other acid suppressing agents in patients with healed erosive esophagitisTable Footnotea
In comparisons with other active treatments, pantoprazole has demonstrated high remission rates. Pantoprazole 20 mg or 40 mg is more effective than ranitidine 150 mg once or twice daily for maintaining healing of GERD after 12 months of therapy () (CitationAdamek et al 2001; CitationMetz and Bochenek 2003; CitationRichter et al 2004). Patients receiving pantoprazole have significantly higher endoscopic remission rates at 12 months () and symptomatic control is also significantly better, as measured by the proportion of symptom-free patients at 12 months () (CitationAdamek et al 2001), the number of symptom-free days during the 12-month period (83% of days vs 58% of days, p < 0.001 [CitationRichter et al 2004] and 78% vs 48%, p < 0.001 [CitationMetz and Bochenek 2003]) and the number of nights without heartburn (93% of nights vs 77% of nights, p = 0.001 [CitationRichter et al 2004] and, p = 0.002 [CitationMetz and Bochenek 2003]). In addition, pantoprazole maintains patients in remission for a longer period of time than does ranitidine (CitationMetz and Bochenek 2003). Pantoprazole is more effective than ranitidine in maintaining endoscopically confirmed healing, regardless of initial disease severity or H. pylori status (CitationMetz and Bochenek 2003, CitationRichter et al 2004).
Only a few studies have evaluated the efficacy of maintenance therapy with pantoprazole in comparison with other PPIs. The data available indicate that pantoprazole 20 mg has similar efficacy to omeprazole 20 mg for maintaining endoscopic and symptomatic remission in patients with healed erosive esophagitis (CitationLauritsen et al 2000). In comparisons with esomeprazole 20 mg daily, there are two studies showing conflicting results. Whereas the study by CitationLabenz and colleagues (2005) showed esomeprazole 20 mg daily to be superior to pantoprazole 20 mg daily, the study by CitationGoh and colleagues (2007) showed esomeprazole 20 mg daily to be as effective as pantoprazole 20 mg daily in keeping patients in combined endoscopic and symptomatic remission ().
In the above trials the symptoms assessed were heartburn, dysphagia or pain on swallowing, and acid regurgitation. In some instances, additional gastric symptoms were also included (CitationPlein et al 2000; CitationLabenz et al 2005), but long-term data regarding the efficacy of pantoprazole for control of respiratory or laryngeal symptoms of GERD are not available. However, long-term high-dose PPI therapy is the first-line approach to controlling these extraesophageal GERD symptoms (CitationHalstead 2005).
Pantoprazole has also demonstrated efficacy in difficult-to-treat patients. In 66 patients with aggressive, complicated GERD refractory to H2-receptor antagonists, but healed with oral pantoprazole, continued therapy with oral pantoprazole 40 mg daily maintained remission in most patients at 24 months (percentages were not reported) (CitationBardhan et al 2001).
It is common for many patients with mild disease and infrequent symptom relapses to use a PPI only when symptoms demand. Patients with symptomatic or mild erosive GERD are therefore ideal candidates for on-demand or intermittent treatment (CitationBardhan 2003). On-demand treatment with oral pantoprazole 20 mg or 40 mg daily provided effective symptomatic control in 634 patients with endoscopically confirmed Savary-Miller grade 0/I GERD and heartburn, with the mean perceived average daily symptom load of heartburn over a 6-month period reduced from 3.93 with placebo to 2.71 with the 40 mg dose and 2.91 with the 20 mg dose (p < 0.0001 for both pantoprazole doses vs placebo) (CitationScholten, Dekkers, et al 2005). The discontinuation rate due to insufficient control of heartburn or unsatisfactory treatment (insufficient control of heartburn or other gastrointestinal symptoms) was significantly lower in both pantoprazole groups than in the placebo group, despite placebo recipients using significantly more antacid therapy (p < 0.05 for all pantoprazole vs placebo comparisons). No significant differences between pantoprazole 20 mg and 40 mg were reported.
These advantages of on-demand pantoprazole over placebo for control of heartburn were confirmed for a wider range of GERD-associated symptoms in another trial. On-demand treatment with pantoprazole 20 mg for 6 months was effective, compared with placebo, in maintaining control of the symptoms of heartburn, acid regurgitation, and pain on swallowing in 439 patients with healed Savary-Miller grade 0/I GERD. Patients’ perceived average daily symptom load was 1.5 and 2.2 for the pantoprazole and placebo group, respectively (p < 0.05), and pantoprazole-treated patients experienced fewer episodes requiring treatment (p < 0.01), and had a lower discontinuation rate due to insufficient control of symptoms or unsatisfactory treatment. Again, antacid usage was significantly higher in placebo recipients than in pantoprazole-treated patients (p < 0.05) (CitationKaspari et al 2005).
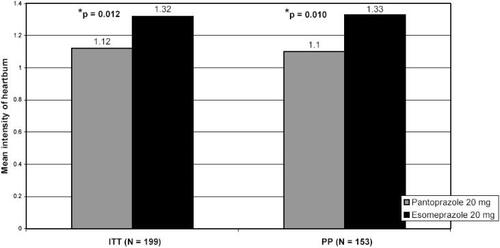
In the only identified comparison of on-demand administration of active treatments, pantoprazole 20 mg significantly reduced the symptom load for heartburn compared with esomeprazole 20 mg (1.12 vs 1.32, p = 0.0115) in 199 patients with Los Angeles classification grade A or B GERD or nonerosive GERD and moderate or severe heartburn. Mean intensities of heartburn were significantly lower in the pantoprazole compared with the esomeprazole treatment group during the 6 months on-demand treatment (1.10 vs 1.33, p = 0.0096) () (CitationScholten, Bohuschke, et al 2005).
Figure 1 On-demand therapy with pantoprazole leads to lower heartburn intensity than with esomeprazole in patients with mild GERD.
Abbreviations: ITT, intention to treat population; PP, per protocol population.
Safety and tolerability
Results of numerous clinical trials indicate that oral pantoprazole is safe and well tolerated for short-term treatment of GERD and for longer term maintenance therapy in patients with healed erosive esophagitis. Oral pantoprazole at dosages of up to 40 mg daily was safe and well tolerated in studies of 1 to 2 years in duration (CitationMossner et al 1997; CitationEscourrou et al 1999; CitationVan Rensburg et al 1999; CitationPlein et al 2000; CitationAdamek et al 2001; CitationMetz and Bochenek 2003; CitationRichter et al 2004; CitationLabenz et al 2005). Although serum gastrin levels tended to increase initially in some, but not all, studies, they generally stabilized and were not associated with adverse histological findings. Adverse events most commonly experienced by patients receiving pantoprazole in these long-term trials are those expected in patients receiving PPI therapy. Events most frequently include diarrhea, nausea, vomiting, headache, dizziness, abdominal pain, infection, and raised liver enzymes. These are usually of mild to moderate intensity and seldom necessitate discontinuation of treatment.
Two longer-term trials have been performed. One reported data for treatment with oral pantoprazole for up to 3 years. In this study, only 4 of 111 patients had adverse events definitely related to pantoprazole. Elevations in gastrin were modest and there were no significant changes in gastric endocrine cells (CitationBardhan et al 2001). The other is an ongoing 10-year study, in which maintenance therapy with pantoprazole 40 mg to 160 mg daily was well tolerated in patients with healed peptic ulcers or erosive esophagitis. There were no increases in signs associated with an enhanced risk of gastric cancer, although fasting serum gastrin levels increased slightly after the second year of treatment but remained at this level thereafter. Of 134 patients originally enrolled in this long-term study, 99 patients were treated with pantoprazole for at least 5 years, and 25 had completed 10 years of treatment (CitationHeinze et al 2003).
The safety profile of pantoprazole in elderly patients is discussed later in this review. Short-term (up to 8 weeks) use of pantoprazole is safe and well tolerated in children and adolescents (aged 5 to 16 years) (CitationMadrazo-de la Garza et al 2003; CitationTolia et al 2006; CitationTsou et al 2006).
Impact of GERD on quality of life
Patients with GERD have significantly (p < 0.05) poorer health-related quality of life than the general population (CitationMcDougall et al 1996; CitationRevicki et al 1998; CitationEnck et al 1999; CitationKaplan-Machlis et al 1999; CitationFarup et al 2001a; CitationPare et al 2003), patients with diabetes or hypertension (CitationRevicki et al 1998; CitationEnck et al 1999), and patients with severe angina pectoris or mild heart failure (CitationDimenas et al 1993). Although there are no relevant differences in health-related quality of life between patients with Barrett’s esophagus, erosive esophagitis and non-erosive GERD (CitationKulig et al 2003), impairment is proportional to the frequency and severity of symptoms, regardless of the presence or absence of esophagitis (CitationDimenas et al 1996; CitationDent et al 1999; CitationKaplan-Machlis et al 1999), is more severe in females and younger patients (CitationHoltmann et al 2006b) and is exacerbated by the presence of nocturnal symptoms (CitationFarup et al 2001a, Citation2001b). Although the frequency and intensity of acid complaints significantly influence the health-related quality of life of patients with GERD (CitationHoltmann et al 2006a), a number of other gastrointestinal symptoms, such as upper abdominal/stomach complaints, lower abdominal/digestive complaints, and nausea, also have a major role (CitationMalagelada et al 2006). The impact of GERD is most striking on measures of pain, mental health, and social function (CitationRevicki et al 1998; CitationEnck et al 1999; CitationFarup et al 2001a). The presence of GERD is also associated with reduced work productivity for affected individuals in the labor force (CitationHenke et al 2000; CitationSandler et al 2002).
The treatment of GERD improves symptoms and health-related quality of life outcomes (CitationWiklund et al 1998; CitationRevicki et al 1999; CitationPrasad et al 2003). Control of heartburn strongly predicts improvement in health-related quality of life during the acute treatment of GERD (CitationPare et al 2003). Although no trials of maintenance therapy have reported quality of life assessments for pantoprazole, several studies have evaluated the effect of short-term pantoprazole on health-related quality of life, and results of these studies generally showed the PPI to improve health-related quality of life (Citationde-Souza-Cury et al 2006) and be superior to H2-receptor antagonists (CitationKaspari et al 2001; CitationPare et al 2003). Health-related quality of life improved more rapidly and to a greater extent following treatment with pantoprazole 40 mg once daily compared with nizatidine 150 mg twice daily in a total of 208 patients with GERD characterized by heartburn (with or without erosive esophagitis). After 7 days, scores for all assessment scales improved more with pantoprazole than nizatidine. Patients receiving pantoprazole showed significantly greater improvement in two SF-36 domains, bodily pain (p < 0.01) and vitality (p < 0.05), and in the gastrointestinal system rating scale (GSRS) reflux score (p < 0.01). After 28 days of treatment, the changes in scores relative to baseline were still greater with pantoprazole than with nizatidine (CitationPare et al 2003). Similarly, in comparison with ranitidine, quality of life parameters tended to improve more with pantoprazole 20 mg once daily than ranitidine 150 mg twice daily according to the gastrointestinal quality of life index (GIQLI) and SF-36, with a significant advantage seen for pantoprazole in the SF-36 vitality score (p < 0.05), in a mixed population of patients with nonerosive GERD or endoscopically confirmed erosive esophagitis. Patients’ assessment of treatment also appeared to be more favorable for pantoprazole in this short-term study (CitationKaspari et al 2001). Patient satisfaction with treatment is similar with pantoprazole, omeprazole, and lansoprazole (at 4 and 8 weeks, respectively, patient satisfaction was 79% and 91% [pantoprazole], 79% and 89% [omeprazole multiple unit pellet system (MUPS)] and 76% and 86% [lansoprazole] in one study [CitationMulder et al 2002]).
Recently, a new GERD specific, reliable, sensitive, and validated questionnaire for the evaluation of health-related quality of life was developed. The GERDyzer™ covers 10 dimensions of quality of life (general well-being, pain/discomfort, physical health, energy, daily activities, leisure activities, social life, diet/eating/drinking habits, mood and sleep) and has demonstrated very high internal consistency, good test-retest reliability, responsiveness and construct validity in patients treated with pantoprazole (CitationHoltmann et al 2005). Using this questionnaire in conjunction with the ReQuest™- GI (CitationStanghellini V et al 2005), all dimensions of treatment satisfaction were shown to increase during 4 weeks of treatment with pantoprazole, with good treatment satisfaction reported after the first week of therapy (CitationDeVault et al. 2006).
Treating patients with GERD is about 2-fold more costly than treating those without GERD (CitationBloom et al 2001). However, PPIs have the lowest total cost per patient of the available pharmacological treatments, when total costs (defined as the costs of diagnosis and initial treatment, and the costs associated with treatment success, treatment failure and remission) are calculated, despite having higher acquisition costs than other acid suppressive agents (CitationHolzer et al 1998). Scant pharmacoeconomic data specific for pantoprazole are available. The only study identified, a modelling study in the Netherlands, showed that pantoprazole may have a more favorable pharmacoeconomic profile than omeprazole. Assumptions were based on available documentation concerning the effectiveness and costs of omeprazole and pantoprazole and findings are only valid if the substitution of omeprazole by pantoprazole can be achieved without loss of efficacy or tolerability (Citationvan Hout et al 2003).
Special considerations in the elderly
GERD appears to be more common and more severe in the elderly than in younger individuals; in fact age is an important risk factor for the development of severe forms of GERD (CitationEl-Serag and Sonnenberg 1997; CitationJohnson and Fennerty 2004). In the primary care setting in the US, as many as 20% of older patients report acid reflux (CitationMold et al 1991), and in a Japanese study, the prevalence of erosive esophagitis in patients aged >70 years was more than triple the prevalence in patients younger than 39 years (CitationMaekawa et al 1998). In common with the general population, the intensity and frequency of heartburn and other symptoms of GERD are poor predictors of the presence or severity of esophageal manifestations. In addition, older patients are less likely to experience severe heartburn than younger patients (CitationJohnson and Fennerty 2004) and the majority (over 75%) do not experience acid regurgitation as an initial symptom (CitationRäihä et al 1991; CitationPilotto and Franceschi 2003). More frequently, elderly patients with GERD report symptoms such as dysphagia, vomiting and respiratory difficulties, anorexia, weight loss, and anemia-melena (CitationPilotto and Franceschi 2003). Because of this different symptom profile of GERD in the elderly, the disease, particularly in milder form, may remain undiagnosed for a considerable period of time (CitationMaekawa et al 1998) resulting in hospital admittance for more severe disease (CitationZimmerman et al 1997).
Elderly patients require endoscopy as the initial diagnostic test for GERD, irrespective of the severity or duration of their symptoms—endoscopy is even indicated in elderly patients without current typical symptoms, but with a past history of GERD (CitationRichter 2000). However, endoscopy can be associated with the risk of complications, particularly in elderly patients with heart or pulmonary disease, and so use of well validated symptom assessment tools may increasingly have a role in the diagnosis and long term management of GERD in elderly patients. Based on their safety profiles and success in the general patient population, PPIs as a class are considered first-line treatment for GERD and erosive esophagitis in the elderly (CitationBacak et al 2006).
Results of a retrospective analysis, based on combined data from two prospective, double-blind, randomized trials in patients with Hetzel-Dent grade ≥2 erosive esophagitis, show that healing rates with pantoprazole 40 mg are similar in elderly patients and in younger patients. At 8 weeks, healing rates were 86% in the 44 patients aged ≥65 years and 83% in the 210 patients aged <65 years. Pantoprazole was more effective than a combined placebo/nizatidine treatment group (p < 0.001) (CitationDeVault et al 2003).
Results of a prospective study have confirmed the efficacy of oral pantoprazole in 164 patients aged ≥65 years with Savary-Miller grade I-III GERD. Patients initially received pantoprazole 40 mg daily for 8 weeks and 81% achieved documented healing of erosive esophagitis. All healed patients subsequently received maintenance therapy with pantoprazole 20 mg daily; 82% remained in remission at 6 months. Continued therapy with pantoprazole 20 mg daily for a further 6 months maintained a remission rate of 80% at 1 year, whereas switching to placebo for the last 6 months of the trial resulted in a remission rate of 30% (CitationPilotto et al 2003). These results show that pantoprazole is highly effective for healing and reducing the relapse of erosive esophagitis, and that discontinuing active treatment after 6 months is associated with a significant increase in the risk of relapse. In this study, the most commonly reported adverse events were glossitis, headache, and diarrhea. These findings are in agreement with data for nonelderly populations.
When treating elderly patients with GERD, concomitant medications should be considered for two main reasons. Firstly, it is known that a number of medications commonly prescribed for elderly patients may promote gastroesophageal reflux and, secondly, drug interactions may be of particular importance in these patients as they are frequently receiving multiple drug therapies (CitationPilotto et al 2005; CitationGorard 2006; CitationSteinman et al 2006). When considering treatment with PPIs, it is important to note that interactions caused by changes in gastric pH are a group-specific effect, but each PPI differs in its propensity to interact with other drugs and the extent to which its interaction profile has been defined. The interaction profiles of omeprazole and pantoprazole have been studied most extensively: omeprazole carries a considerable potential for drug interactions, whereas pantoprazole appears to have lower potential for interactions with other medications. The interaction profiles of esomeprazole, lansoprazole, and rabeprazole have been less extensively investigated, but evidence suggests that lansoprazole and rabeprazole have weaker potentials for interactions than omeprazole, and esomeprazole has a propensity for drug interactions similar to that of omeprazole. (CitationBlume et al 2006). This pharmacokinetic profile suggests that pantoprazole is well suited for use in elderly patients who as a group frequently present with comorbidities and receive multiple therapies.
Conclusion
The optimal treatment of GERD is vital for a number of reasons. GERD is a chronic, relapsing disease that can progress to major complications; affected patients have significantly poorer health-related quality of life than the general population, with impairment being proportional to the frequency and severity of symptoms; and as GERD requires continued therapy to prevent relapse and complications, most patients with erosive esophagitis require long-term acid suppressive treatment. Thus GERD results in a significant cost burden.
The effective treatment of GERD provides symptom resolution and high rates of remission in erosive esophagitis, lowers the incidence of GERD complications, improves health-related quality of life and reduces the cost of this disease. PPIs are accepted as the most effective treatment for GERD and are the mainstay of initial GERD management, providing more rapid symptom control and better healing of erosive esophagitis than H2-receptor antagonists and antacids. PPIs are also the preferred agents for maintenance therapy in patients with healed erosive esophagitis (CitationLauritsen et al 2003). As few differences in safety or efficacy have been reported between the available PPIs, the decision to select one PPI over another is most likely to be based on the agents’ acquisition costs, formulations, Food and Drug Administration-labeled indications, and overall safety profiles (CitationWelage and Berardi 2000).
The data reviewed here show that oral pantoprazole is a safe, well tolerated and effective initial and maintenance treatment for patients with nonerosive GERD or erosive esophagitis. Oral pantoprazole has greater efficacy than that of H2-receptor antagonists and generally has similar efficacy to other PPIs for the initial and maintenance treatment of GERD. In addition, oral pantoprazole has been shown to improve the quality of life of patients with GERD and is associated with high levels of patient satisfaction with therapy. GERD appears to be more common and more severe in the elderly. Furthermore, as elderly are taking multiple medications at the same time, or drugs with a narrow therapeutic window, drug interactions may be of particular importance in those patients. Pantoprazole has also shown to be an effective and safe treatment for this at-risk population.
References
- AchimARiddermannTPfaffenbergerBPantoprazole 40 mg is at least comparable to esomeprazole 40 mg in achieving endoscopically confirmed healing and symptom relief of gastroesophageal reflux disease (GERD) after 4, 8 and 12 weeks of treatmentCan J Gastroenterol200519Suppl C DR.0038
- AdamekRJBehrendtJWenzelCRelapse prevention in reflux oesophagitis with regard to Helicobacter pylori status: a double-blind, randomized, multicentre trial to compare the efficacy of pantoprazole versus ranitidineEur J Gastroenterol Hepatol2001138111711474311
- ArangoLAngelAMolinaRIComparison between digestive endoscopy and 24-hour esophageal pH monitoring for the diagnosis of gastroesophageal reflux esophagitis: “presentation of 100 cases.Hepatogastroenterology2000471748010690605
- ArnoldRSafety of proton pump inhibitors—an overviewAliment Pharmacol Ther1994865708180297
- BacakBSPatelMTweedEWhat is the best way to manage GERD symptoms in the elderly?J Fam Pract2006552514,816510061
- BardhanKDIntermittent and on-demand use of proton pump inhibitors in the management of symptomatic gastroesophageal reflux diseaseAm J Gastroenterol200398S40812644030
- BardhanKDCherianPBishopAEPantoprazole therapy in the long-term management of severe acid peptic disease: clinical efficacy, safety, serum gastrin, gastric histology, and endocrine cell studiesAm J Gastroenterol20019617677611419827
- BellNJHuntRHProgress with proton pump inhibitionYale J Biol Med19926564957 discussion 89–921341069
- BloomBSJayadevappaRWahlPTime trends in cost of caring for people with gastroesophageal reflux diseaseAm J Gastroenterol200196S64911510775
- BlumeHDonathFWarnkeAPharmacokinetic drug interaction profiles of proton pump inhibitorsDrug Safety2006297698416944963
- BochenekWJMackMEFragaPDPantoprazole provides rapid and sustained symptomatic relief in patients treated for erosive oesophagitisAliment Pharmacol Ther20042011051415569113
- BollschweilerEWolfgartenEGutschowCDemographic variations in the rising incidence of esophageal adenocarcinoma in white malesCancer2001925495511505399
- CarlssonRDentJWattsRGastro-oesophageal reflux disease in primary care: an international study of different treatment strategies with omeprazole. International GORD Study GroupEur J Gastroenterol Hepatol199810119249581986
- CaroJJSalasMWardAHealing and relapse rates in gastroesophageal reflux disease treated with the newer proton-pump inhibitors lansoprazole, rabeprazole, and pantoprazole compared with omeprazole, ranitidine, and placebo: evidence from randomized clinical trialsClin Ther200123998101711519776
- CheerSMPrakashAFauldsDPantoprazole: an update of its pharmacological properties and therapeutic use in the management of acid-related disordersDrugs2003631013312487624
- ChibaNProton pump inhibitors in acute healing and maintenance of erosive or worse esophagitis: a systematic overviewCan J Gastroenterol199711Suppl B66B73B
- ChibaNDe GaraCJWilkinsonJMSpeed of healing and symptom relief in grade II to IV gastroesophageal reflux disease: a meta-analysisGastroenterology199711217988109178669
- CrawleyJAMaclin SchmittCHow satisfied are chronic heartburn sufferers with their prescription medications? Results of the patient unmet needs surveyJ Clin Outcomes Manag200072934
- CsendesASmokGCerdaGPrevalence of Helicobacter pylori infection in 190 control subjects and in 236 patients with gastroesophageal reflux, erosive esophagitis or Barrett’s esophagusDis Esophagus19971038429079272
- DajaniEZGastroesophageal reflux disease: pathophysiology and pharmacology overviewJ Assoc Acad Minor Phys20001171110826019
- DentJBrunJFendrickAAn evidence-based appraisal of reflux disease management—the Genval Workshop reportGut199944S1S1610741335
- de-Souza-CuryMFerrariAPCiconelliREvaluation of health-related quality of life in gastroesophageal reflux disease patients before and after treatment with pantoprazoleDiseases of the Esophagus2006192899316866863
- DeVaultKLynnRBochenekWSuccessful treatment of elderly patients with erosive esophagitis (EE) using pantoprazole 40 mgAm J Gastroenterol2003SepSuppl.S3
- DeVaultKRCastellDOUpdated guidelines for the diagnosis and treatment of gastroesophageal reflux disease. The Practice Parameters Committee of the American College of GastroenterologyAm J Gastroenterol19999414344210364004
- DeVaultKMalageladaJHoltmannGGERDyzer™ treatment satisfaction module: correlation with symptom assessment by ReQuest™—GI (abstract)Am J Gastroenterol2006101Suppl. 2S400
- DimenasECarlssonGGliseHRelevance of norm values as part of the documentation of quality of life instruments for use in upper gastrointestinal diseaseScand J Gastroenterol Suppl19962218139110389
- DimenasEGliseHHallerbackBQuality of life in patients with upper gastrointestinal symptoms. An improved evaluation of treatment regimens?Scand J Gastroenterol19932868178210982
- DonnellanCSharmaNPrestonCMedical treatments for the maintenance therapy of reflux oesophagitis and endoscopic negative reflux diseaseCochrane Database Syst Rev20044CD003245
- El-SeragHBSonnenbergAAssociations between different forms of gastro-oesophageal reflux diseaseGut19974159499414963
- EnckPDuboisDMarquisPQuality of life in patients with upper gastrointestinal symptoms: results from the Domestic/International Gastroenterology Surveillance Study (DIGEST)Scand J Gastroenterol Suppl1999231485410565623
- EscourrouJDeprezPSaggioroAMaintenance therapy with pantoprazole 20 mg prevents relapse of reflux oesophagitisAliment Pharmacol Ther19991314819110571605
- FarupCKleinmanLSloanSThe impact of nocturnal symptoms associated with gastroesophageal reflux disease on health-related quality of lifeArch Intern Med2001a161455211146697
- FarupCKleinmanLSloanSThe impact of nocturnal symptoms associated with gastroesophageal reflux disease on health-related quality of lifeArch Intern Med2001b161455211146697
- FassROfmanJJGralnekIMClinical and economic assessment of the omeprazole test in patients with symptoms suggestive of gastroesophageal reflux diseaseArch Intern Med19991592161810527293
- FassROfmanJJSamplinerREThe omeprazole test is as sensitive as 24-h oesophageal pH monitoring in diagnosing gastro-oesophageal reflux disease in symptomatic patients with erosive oesophagitisAliment Pharmacol Ther2000143899610759617
- FendrickAMManagement of patients with symptomatic gastroesophageal reflux disease: a primary care perspectiveAm J Gastroenterol200196S293311510767
- FennertyMBZuckermanSSpreenKAHeartburn severity does not predict disease severity in gastroesophageal reflux patients with erosive esophagitis2002Las Vegas, NVAmerican Osteopathic Association
- FrestonJWLong-term acid control and proton pump inhibitors: interactions and safety issues in perspectiveAm J Gastroenterol19979251S5S discussion 5S–7S9127627
- GillessenABeilWModlinIM40 mg pantoprazole and 40 mg esomeprazole are equivalent in the healing of esophageal lesions and relief from gastroesophageal reflux disease-related symptomsJ Clin Gastroenterol2004383324015087692
- GlatzelDAbdel-QaderMGatzGPantoprazole 40 mg is as effective as esomeprazole 40 mg to relieve symptoms of gastroesophageal reflux disease (GERD) after 4 weeks of treatment and superior regarding prevention of symptomatic relapseDigestion2006741455417230024
- GohKWuCBenamouzigRSanderPEfficacy of Pantoprazole 20 mg daily compared to Esomeprazole 20 mg daily in the maintenance of gastroesophageal reflux disease: a randomized, double-blind comparative trial: the EMANCIPATE studyEuro J Gastro Hepatol20071920511
- GorardDAEscalating polypharmacyQJM20069979780017030528
- GreenJIs there such an entity as mild oesophagitis?Eur J Clin Res199342934
- HaagSHoltmannGReflux disease and Barrett’s esophagusEndoscopy2003351121712561004
- HabermannWKieslerKEhererAShort-term therapeutic trial of proton pump inhibitors in suspected extraesophageal refluxJ Voice2002164253212395996
- HalsteadLAExtraesophageal manifestations of GERD: diagnosis and therapyDrugs Today (Barc)200541Suppl B192616200228
- HeinzeHPreinfalkJAthmannCClinical efficacy and safety of pantoprazole in severe acid-peptic disease during up to 10 years maintenance treatmentGut200352Suppl. VIA63
- HenkeCJLevinTRHenningJMWork loss costs due to peptic ulcer disease and gastroesophageal reflux disease in a health maintenance organizationAm J Gastroenterol2000957889210710076
- HetzelDJDentJReedWDHealing and relapse of severe peptic esophagitis after treatment with omeprazoleGastroenterology198895903123044912
- HollenzMStolteMLabenzJPrevalence of gastro-oesophageal reflux disease in general practiceDeutsche Medizinische Wochenschrift200212710071211997867
- HoltmannGChassanyODeVaultKGERDyzer™: validation of a new scale for the assessment of health related quality of life in gastroesophageal reflux disease (GERD) [abstract]Gut200554Suppl. VIIA52
- HoltmannGDeVaultKChassanyOFast onset of action: the initial dose of pantoprazole is superior to esomeprazole in reducing the frequence and intensity of acid episodes determined by ReQuest™ [abstract]Gut2006a55Suppl. VA271
- HoltmannGMalageladaJChassanyOGender and age influence health-related quality of life (HRQoL) in GERD: patients assessed by GERDyzerTM [abstract]Gut2006b55Suppl VA269
- HolzerSSJudayTRJoelssonBDetermining the cost of gastroesophageal reflux disease: a decision analytic modelAm J Manag Care1998414506010338737
- JohanssonKEAskPBoerydBOesophagitis, signs of reflux, and gastric acid secretion in patients with symptoms of gastrooesophageal reflux diseaseScand J Gastroenterol198621837473775250
- JohnsonDAEndoscopic therapy for GERD—baking, sewing, or stuffing: an evidence-based perspectiveRev Gastroenterol Disord20033142914502118
- JohnsonDAFennertyMBHeartburn severity underestimates erosive esophagitis severity in elderly patients with gastroesophageal reflux diseaseGastroenterology2004126660414988819
- KahrilasPJFennertyMBJoelssonBHigh- versus standard-dose ranitidine for control of heartburn in poorly responsive acid reflux disease: a prospective, controlled trialAm J Gastroenterol1999949279934737
- Kaplan-MachlisBSpieglerGERevickiDAHealth-related quality of life in primary care patients with gastroesophageal reflux diseaseAnn Pharmacother1999331032610534213
- KaspariSBiedermannAMeyJComparison of pantoprazole 20 mg to ranitidine 150 mg bid in the treatment of mild gastroesophageal reflux diseaseDigestion2001631637011351143
- KaspariSKupcinskasLHeinzeHPantoprazole 20 mg on demand is effective in the long-term management of patients with mild gastro-oesophageal reflux diseaseEur J Gastroenterol Hepatol2005179354116093871
- KuligMLeodolterAViethMQuality of life in relation to symptoms in patients with gastro-oesophageal reflux disease—an analysis based on the ProGERD initiativeAliment Pharmacol Ther2003187677614535869
- LabenzJArmstrongDLauritsenKEsomeprazole 20 mg vs. pantoprazole 20 mg for maintenance therapy of healed erosive oesophagitis: results from the EXPO studyAliment Pharmacol Ther2005228031116225489
- LabenzJMalfertheinerPHelicobacter pylori in gastro-oesophageal reflux disease: causal agent, independent or protective factor?Gut199741277809378377
- LabenzJPetersenKURoschWA summary of Food and Drug Administration-reported adverse events and drug interactions occurring during therapy with omeprazole, lansoprazole and pantoprazoleAliment Pharmacol Ther20031710151912694083
- LagergrenJBergströmRLindgrenASymptomatic gastroesophageal reflux as a risk factor for esophageal adenocarcinomaN Engl J Med19993408253110080844
- LassenAHallasJde MuckadellOBEsophagitis: incidence and risk of esophageal adenocarcinoma—a population-based cohort studyAm J Gastroenterol20061011193916771936
- LauritsenKDevièreJBigardMAEsomeprazole 20 mg and lansoprazole 15 mg in maintaining healed reflux oesophagitis: Metropole study resultsAm J Gastroenterol20031719
- LauritsenKJaupBCarlingLComparable efficacy of pantoprazole and omeprazole to prevent relapse in patients with GERD [abstract]Gut200047Suppl. IIIA60
- LundellLMiettinenPMyrvoldHELong-term management of gastro-oesophageal reflux disease with omeprazole or open antireflux surgery: results of a prospective, randomized clinical trial. The Nordic GORD Study GroupEur J Gastroenterol Hepatol2000128798710958215
- Madrazo-De la GarzaADibildoxMVargasAEfficacy and safety of oral pantoprazole 20 mg given once daily for reflux esophagitis in childrenJ Pediatr Gastroenterol Nutr200336261512548064
- MaekawaTKinoshitaYOkadaARelationship between severity and symptoms of reflux oesophagitis in elderly patients in JapanJ Gastroenterol Hepatol199813927309794192
- MalageladaJChassanyODeVaultKHealth-related quality of life (HRQoL) in GERD patients is significantly infl uenced by gastrointestinal symptoms [abstract]Gut200655Suppl. VA253
- McDougallNIJohnstonBTKeeFNatural history of reflux oesophagitis: a 10 year follow up of its effect on patient symptomatology and quality of lifeGut19963848168707073
- MetzDCBochenekWJPantoprazole maintenance therapy prevents relapse of erosive oesophagitisAliment Pharmacol Ther2003171556412492745
- MoldJWReedLEDavisABPrevalence of gastroesophageal reflux in elderly patients in a primary care settingAm J Gastroenterol199186965701858762
- MossnerJKoopHPorstHOne-year prophylactic efficacy and safety of pantoprazole in controlling gastro-oesophageal reflux symptoms in patients with healed reflux oesophagitisAliment Pharmacol Ther1997111087929663834
- MulderCJWesterveldBDSmitJMA double-blind, randomized comparison of omeprazole Multiple Unit Pellet System (MUPS) 20 mg, lansoprazole 30 mg and pantoprazole 40 mg in symptomatic reflux oesophagitis followed by 3 months of omeprazole MUPS maintenance treatment: a Dutch multicentre trialEur J Gastroenterol Hepatol2002146495612072599
- MyrvoldHELundellLMiettinenPThe cost of long term therapy for gastro-oesophageal reflux disease: a randomised trial comparing omeprazole and open antireflux surgeryGut2001494889411559644
- NetzerPBrabetz-HofligerABrundlerRComparison of the effect of the antacid Rennie versus low-dose H2-receptor antagonists (ranitidine, famotidine) on intragastric acidityAliment Pharmacol Ther199812337429690722
- NumansMELauJde WitNJShort-term treatment with proton-pump inhibitors as a test for gastroesophageal reflux disease: a meta-analysis of diagnostic test characteristicsAnn Intern Med20041405182715068979
- NwokoloCUSmithJTGaveyCTolerance during 29 days of conventional dosing with cimetidine, nizatidine, famotidine or ranitidineAliment Pharmacol Ther19904Suppl 129451983345
- OrlandoRYamadaTAlpersDReflux esophagitisTextbook of gastroenterology1999PhiladelphiaLippincott Williams & Wilkins123563
- OrlandoRCThe pathogenesis of gastroesophageal reflux disease: the relationship between epithelial defense, dysmotility, and acid exposureAm J Gastroenterol1997923S5S discussion S–7S9127620
- OrlandoRCCurrent understanding of the mechanisms of gastrooesophageal reflux diseaseDrugs200666Suppl 115 discussion 29–3316869342
- ParePArmstrongDPericakDPantoprazole rapidly improves health-related quality of life in patients with heartburn: a prospective, randomized, double blind comparative study with nizatidineJ Clin Gastroenterol200337132812869883
- PilottoAFranceschiMPilottoAMalfertheinerPHoltPGastro-esophageal reflux disease in the elderlyAging and the gastrointestinal tract. Interdisciplinary topics in gerontology2003BaselKarger Press10017
- PilottoAFranceschiMParisFRecent advances in the treatment of GERD in the elderly: focus on proton pump inhibitorsInt J Clin Pract2005591204916178989
- PilottoALeandroGFranceschiMShort- and long-term therapy for reflux oesophagitis in the elderly: a multi-centre, placebo-controlled study with pantoprazoleAliment Pharmacol Ther200317139940612786634
- PleinKHotzJWurzerHPantoprazole 20 mg is an effective maintenance therapy for patients with gastro-oesophageal reflux diseaseEur J Gastroenterol Hepatol2000124253210783996
- PrasadMRentzAMRevickiDAThe impact of treatment for gastro-oesophageal reflux disease on health-related quality of life: a literature reviewPharmacoeconomics2003217699012859219
- RaghunathAHunginAPWooffDPrevalence of Helicobacter pylori in patients with gastro-oesophageal reflux disease: systematic reviewBMJ200332673712676842
- RaiAOrlandoRGastroesophageal reflux diseaseCur Opin Gastroenterol19981432633
- RäihäIHietanenESouranderLSymptoms of gastro-oesophageal reflux disease in elderly peopleAge Ageing199120365701755393
- RevickiDACrawleyJAZodetMWComplete resolution of heartburn symptoms and health-related quality of life in patients with gastrooesophageal reflux diseaseAliment Pharmacol Ther19991316213010594397
- RevickiDAWoodMMatonPNThe impact of gastroesophageal reflux disease on health-related quality of lifeAm J Med199810425289552088
- RichterJEGastroesophageal reflux disease in the older patient: presentation, treatment, and complicationsAm J Gastroenterol2000953687310685737
- RichterJEBochenekWOral pantoprazole for erosive esophagitis: a placebo-controlled, randomized clinical trial. Pantoprazole US GERD Study GroupAm J Gastroenterol20009530718011095320
- RichterJEFragaPMackMPrevention of erosive oesophagitis relapse with pantoprazoleAliment Pharmacol Ther2004205677515339328
- RobinsonMHornJClinical pharmacology of proton pump inhibitors: what the practising physician needs to knowDrugs20036327395414664653
- RuigomezAGarcia RodriguezLAWallanderMANatural history of gastro-oesophageal reflux disease diagnosed in general practiceAliment Pharmacol Ther2004207516015379835
- SachsGProton pump inhibitors and acid-related diseasesPharmacotherapy19971722379017763
- SandlerRSEverhartJEDonowitzMThe burden of selected digestive diseases in the United StatesGastroenterology200212215001111984534
- ScholtenTBohuschkeMGatzGOn-demand therapy with pantoprazole 20 mg leads to lower heartburn intensity than with esomeprazole 20 mg in patients with mild GERDGut200554Suppl. VIIA109
- ScholtenTDekkersCPSchutzeKOn-demand therapy with pantoprazole 20 mg as effective long-term management of reflux disease in patients with mild GERD: the ORION trialDigestion200572768516113546
- ScholtenTGatzGHoleUOnce-daily pantoprazole 40 mg and esomeprazole 40 mg have equivalent overall efficacy in relieving GERD-related symptomsAliment Pharmacol Ther2003185879412969085
- ShakerRCastellDOSchoenfeldPSNighttime heartburn is an under-appreciated clinical problem that impacts sleep and daytime function: the results of a Gallup survey conducted on behalf of the American Gastroenterological AssociationAm J Gastroenterol20039814879312873567
- SharmaPVakilNReview article: Helicobacter pylori and reflux diseaseAliment Pharmacol Ther20031729730512562442
- ShawMJFendrickAMKaneRLSelf-reported effectiveness and physician consultation rate in users of over-the-counter histamine-2 receptor antagonistsAm J Gastroenterol200196673611280532
- SontagSJSonnenbergASchnellTGThe long-term natural history of gastroesophageal reflux diseaseJ Clin Gastroenterol20064039840416721220
- SpechlerSJGoyalRKBarrett’s esophagusN Engl J Med1986315362712874485
- SpechlerSJLeeEAhnenDLong-term outcome of medical and surgical therapies for gastroesophageal reflux disease: follow-up of a randomized controlled trialJAMA20012852331811343480
- StanghelliniVArmstrongDMonnikesHDetermination of ReQuest-based symptom thresholds to define symptom relief in GERD clinical studiesDigestion2005711455115870502
- SteinmanMALandefeldCSRosenthalGEPolypharmacy and prescribing quality in older peopleJ Am Geriatr Soc20065415162317038068
- TeferaLFeinMRitterMPCan the combination of symptoms and endoscopy confirm the presence of gastroesophageal reflux disease?Am Surg19976393369322676
- ToliaVBishopPTsouVMulticenter, randomized, double-blind study comparing 10, 20 and 40 mg pantoprazole in children (5–11 years) with symptomatic gastroesophageal reflux diseaseJ Pediatr Gastroenterol Nutr2006423849116641576
- TsouVBakerRBookLMulticenter, randomized, double-blind study comparing 20 and 40 mg of pantoprazole for symptom relief in adolescents (12 to 16 years of age) with gastroesophageal reflux disease (GERD)Clin Pediatr2006457419
- VakilNShawMKirbyRClinical effectiveness of laparoscopic fundoplication in a U.S. communityAm J Med20031141512543281
- VakilNvan ZantenSVKahrilasPThe Montreal definition and classification of gastroesophageal reflux disease: a global evidence-based consensusAm J Gastroenterol200610119002016928254
- Van HerwaardenMASamsomMSmoutAJExcess gastroesophageal reflux in patients with hiatus hernia is caused by mechanisms other than transient LES relaxationsGastroenterology200011914394611113064
- van HoutBAKlokRMBrouwersJRA pharmacoeconomic comparison of the efficacy and costs of pantoprazole and omeprazole for the treatment of peptic ulcer or gastroesophageal reflux disease in The NetherlandsClin Ther2003256354612749518
- van RensburgCJHoniballPJGrundlingHDEfficacy and tolerability of pantoprazole 40 mg versus 80 mg in patients with reflux oesophagitisAliment Pharmacol Ther1996103974018791969
- Van RensburgCJHoniballPJVan ZylJHSafety and efficacy of pantoprazole 40 mg daily as relapse prophylaxis in patients with healed reflux oesophagitis-a 2-year follow-upAliment Pharmacol Ther1999131023810468676
- WatsonDIJamiesonGGBaigrieRJLaparoscopic surgery for gastro-oesophageal reflux: beyond the learning curveBr J Surg199683128478983630
- WelageLSBerardiRREvaluation of omeprazole, lansoprazole, pantoprazole, and rabeprazole in the treatment of acid-related diseasesJ Am Pharm Assoc (Wash)2000405262 quiz 121–310665250
- WiklundIBardhanKDMuller-LissnerSQuality of life during acute and intermittent treatment of gastro-oesophageal reflux disease with omeprazole compared with ranitidine. Results from a multicentre clinical trial. The European Study GroupItal J Gastroenterol Hepatol19983019279615259
- WyethJWPounderRESercombeJCThe effects of low doses of ranitidine on intragastric acidity in healthy menAliment Pharmacol Ther199812255619570260
- ZimmermanJShohatVTsvangEEsophagitis is a major cause of upper gastrointestinal hemorrhage in the elderlyScand J Gastroenterol19973290699299669