Abstract
The sympathetic nervous system is involved in regulating various cardiovascular parameters including heart rate (HR) and HR variability. Aberrant sympathetic nervous system expression may result in elevated HR or decreased HR variability, and both are independent risk factors for development of cardiovascular disease, including heart failure, myocardial infarction, and hypertension. Epidemiologic studies have established that impaired HR control is linked to increased cardiovascular morbidity and mortality. One successful way of decreasing HR and cardiovascular mortality has been by utilizing β-blockers, because their ability to alter cell signaling at the receptor level has been shown to mitigate the pathogenic effects of sympathetic nervous system hyperactivation. Numerous clinical studies have demonstrated that β-blocker-mediated HR control improvements are associated with decreased mortality in postinfarct and heart failure patients. Although improved HR control benefits have yet to be established in hypertension, both traditional and vasodilating β-blockers exert positive HR control effects in this patient population. However, differences exist between traditional and vasodilating β-blockers; the latter reduce peripheral vascular resistance and exert neutral or positive effects on important metabolic parameters. Clinical evidence suggests that attainment of HR control is an important treatment objective for patients with cardiovascular conditions, and vasodilating β-blocker efficacy may aid in accomplishing improved outcomes.
Introduction
Numerous studies have reported that increased heart rate (HR) is a predictor of cardiovascular mortality in healthy people, those who have had a myocardial infarction (MI), and in patients with heart failure (HF).Citation1 Increased HR is recognized as a negative prognostic factor independent of other clinical parameters, including left ventricular function.Citation1 The increased mortality observed with an increased HR may be a consequence of the deleterious sympathovagal imbalance that can be characterized by sympathetic nervous system predominance, vagal depression, or the combined impact of this dysregulation on cardiovascular function.Citation1,Citation2 Elevated HR increases cardiac output (short term) and myocardial oxygen consumption, while simultaneously reducing time of diastole and myocardial blood supply, conditions that favor the development of myocardial ischemia and arrhythmias in ischemic areas.Citation1
Blockade of β-adrenergic receptors is part of the combined medical prevention of cardiovascular disease.Citation3,Citation4 β-Blockers have been efficacious and beneficial in the treatment of various cardiovascular disease states, including angina, HF, MI, and ventricular arrhythmias.Citation5 Randomized controlled clinical studies consistently demonstrate that β-blockers reduce sudden cardiac death by 30% to 50% in patients with coronary artery disease and HF.Citation6 The clinical benefits of β-blockers have been attributed to their ability to antagonize β-adrenergic receptors in the heart and the periphery.Citation7 Traditional β-blockers (eg, atenolol and propranolol), which target either β1- (cardioselective) or β1- and β2-adrenergic receptors (nonselective), decrease BP primarily via a reduction in HR and cardiac output, but do not appreciably affect peripheral vascular resistance.Citation5 Acutely, uptitration of β-blockers can decrease cardiac output and increase vascular tone, which may exert a detrimental effect on renal perfusion and decrease patient drug tolerability, while exacerbating glucose and lipid metabolism.Citation8,Citation9 In addition, these metabolic perturbations may lead to further vascular complications by adversely affecting endothelial function and promoting the development or progression of diabetes.Citation9,Citation10
Vasodilatory β-blockers (eg, carvedilol, labetalol, and nebivolol) and those that provide more complete adrenergic blockade may, in part, mediate vasodilation via blockade of α1-adrenergic receptors or increased endothelium-derived nitric oxide release, which may lead to a reduction in total peripheral vascular resistance.Citation9 This review will examine the data, including recent analyses from the large cardiovascular trials, related to adrenergic blockade, HR control, and its impact on outcomes across the cardiovascular disease spectrum (ie, patients who have had a MI or who have HF or hypertension).
Heart rate and heart rate variability
Heart rate is not a static hemodynamic parameter but instead changes over time in response to physical and mental demands. Heart rate is normally determined by spontaneous and periodic depolarizations of the sinoatrial node, the frequency of which is modulated by the sympathetic and parasympathetic divisions of the autonomic nervous system, the intrinsic cardiac nervous system, reflexes, and respiration. These neural systems also partially control cardiac contractility and conduction of electrical activity through the heart. As a result, HR (chronotropism), contractility (inotropism), and conduction (dromotropism) are adjusted to meet the changing needs of the body. Aberrant sympathetic activation has been implicated as part of the sequelae consistent with the development of HF, MI, and hypertension.Citation11,Citation12 Profoundly elevated sympathetic activity for an extended period accompanied by parasympathetic withdrawal may result in chronically elevated HR, as well as neurohormonal stimulation, and is associated with a decreased threshold for ventricular fibrillation. This upregulation of the sympathetic nervous system and increased adrenergic activation is also associated with pathologic remodeling, myocyte apoptosis, and a dysregulation of calcium handling that leads to myocardial ischemia, a decrement in contractile function, and an increased risk of ventricular arrhythmias.Citation13,Citation14 Due to the correlative linkage of HR and sympathetic nervous system outflow, HR control may be used as a surrogate for sympathetic nervous system activity.
Optimal heart rate
Heart rate varies between individuals, and in a resting individual HR may vary according to time of day, physical conditioning, environmental influences, and sympathetic nervous system vagal tone. However, recent reports suggest that HR should generally be maintained substantially below the traditionally defined tachycardia threshold of 90 to 100 beats/minute.Citation15 A continuous linear increase in cardiovascular risk has been noted in patients whose HR exceeds 60 beats/minute.Citation16,Citation17 Results from the Global Utilization of Streptokinase and TPA for Occluded Arteries (GUSTO-1) study suggest that an increased risk of cardiovascular disease may even exist when HR is <60 beats/minute.Citation18 Increases in HR exceeding 10 beats/minute are associated with a 14% increase in cardiovascular mortality and a 20% increase in total mortality in patients with hypertension.Citation19 In the general population, the mortality risk is increased three-fold in individuals with a HR of 90 to 99 beats/minute compared with individuals with a HR ≤ 60 beats/minute.Citation20
Heart rate and mortality
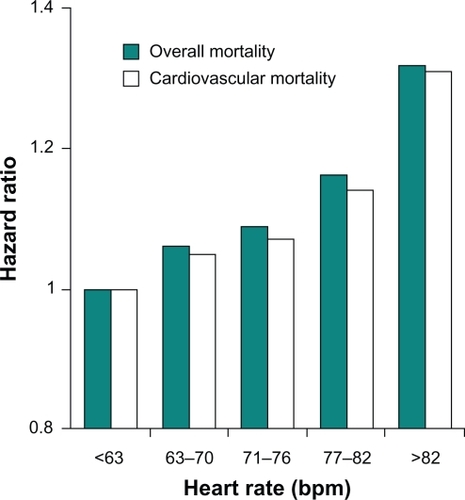
Numerous studies report that a significant association exists between resting HR and cardiovascular and all-cause mortality in the general population, as well as among patients with cardiovascular disease. Epidemiologic studies involving approximately 30,000 individuals over a period of five to 36 years revealed an inverse relationship between HR and survival in the general population.Citation20–Citation25 The risk of coronary artery disease, stroke, death due to noncardiovascular diseases, and total mortality increased with higher HR. Among 5713 healthy male volunteers without known or suspected cardiovascular disease who were observed for an average of 23 years, cardiovascular and all-cause mortality from acute MI increased with progressive elevations in resting HR.Citation17 This independent variable remained significant after adjustment for exercise capacity, age, diabetes, systolic arterial pressure, body mass index, level of physical activity, and other factors. The relationship was most apparent for sudden death ().Citation17 In a study of 10,267 patients with acute coronary syndromes, mortality at 30 days and 10 months progressively increased with increasing HR (P < 0.001).Citation26 Similarly, all-cause and cardiovascular mortality were directly related to resting HR at study entry in 24,913 patients with suspected or proven coronary artery disease who participated in the Coronary Artery Surgery Study (CASS) registry for a period of 15 years (P < 0.0001; ).Citation15,Citation16 The predictive capacity of HR was independent of concomitant hypertension, diabetes, smoking, left ventricular ejection fraction, and number of diseased coronary vessels.
Figure 1 Heart rate and mortality in healthy individuals: Relative risk of death from any cause, nonsudden death from myocardial infarction (MI), and sudden death from MI in 5713 people without known or suspected heart disease. Differences among quintiles with respect to risk of death from any cause, P < 0.001; nonsudden death from cardiac causes, P = 0.02; sudden death from cardiac causes, P < 0.001. Copyright @ 2005. Massachusetts Medical Society. All rights reserved. Reprinted with permission from Jouven X, Empana JP, Schwartz PJ, Desnos M, Courbon D, Ducimetiere P. Heart-rate profile during exercise as a predictor of sudden death. N Engl J Med. 2005;352(19):1951–1958.
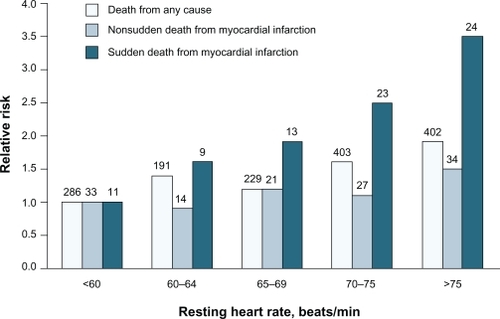
Figure 2 Heart rate and mortality in coronary artery disease: Relationship between resting heart rate and all-cause and cardiovascular mortality in 24,913 patients with suspected or proven coronary artery disease. Based on data from Diaz et al.Citation16 Copyright © 2007. Reprinted with permission from Fox K, Borer JS, Camm AJ, et al. Resting heart rate in cardiovascular disease. J Am Coll Cardiol. 2007;50(9):823–830.
Because the association between HR and mortality is well known, resting HR is currently included in risk assessment indices for patients with acute coronary syndromes (eg, the Global Registry of Acute Coronary Events risk prediction score)Citation27 and acute MI (eg, the Gruppo Italiano per lo Studio della Sopravivenza nell’Infarto Miocardico Prevenzione risk assessment modelCitation28 and the Thrombolysis in Myocardial Infarction Risk ScoreCitation29). However, HR is not included in some of the more widely used indices for cardiovascular risk assessment, including the Copenhagen Risk ScoreCitation30 and the European SCORE project,Citation31 which indicates that HR is not universally accepted as a prognostic factor and a potential therapeutic target in patients with cardiovascular disease.
Heart rate variability
Heart rate variability (HRV) refers to the beat-to-beat difference or R-R interval change in the intrinsic rhythm of the heart.Citation32 Assessment of HRV may provide a surrogate measure of cardiac health, as defined by the degree of equilibrium between sympathetic and parasympathetic (vagus nerve) activity.Citation33 HRV can be assessed by time or frequency domain indices.Citation32 Time domain measures are based on the amount of time in milliseconds in the beat-to-beat intervals of the heart or on the differences between the normal beat-to-beat intervals.Citation33 Frequency domain measures of HRV provide information about the frequency distribution of the components of HRV using power spectral density analysis.Citation33 Nonlinear dynamic analysis (eg, Poincaré plots) may also be used to quantify HRV, but the clinical utility of this method has not been fully established.Citation32 As discussed in subsequent sections, numerous studies have demonstrated the positive prognostic power of reduced HRV to predict all-cause mortality, sudden cardiac death, and cardiac events in patients who have experienced an MI, as well as in patients who have HF or hypertension.
Heart rate control in heart failure
HF is frequently associated with a decreased threshold for ventricular fibrillation, as well as an increased risk of other malignant arrhythmias and sudden cardiac death. Increased HR (eg, atrial fibrillation with a rapid ventricular rate or multiple premature contractions) may contribute to the development of HF and is also associated with a poor prognosis in patients with HF.Citation34 In the normal heart, a stepwise increase in contractility develops as HR increases. Ninety percent of patients with HF die of cardiovascular causes.Citation35 Approximately half of these patients die from progressive, advanced disease and the remaining patients die suddenly, most frequently because of arrhythmia despite a perceivably stable clinical condition. Sudden cardiac death occurs most frequently in patients in New York Heart Association Functional Class II or III. Risk factors for sudden cardiac death include elevated resting HR, and reduced HRV and left ventricular ejection fraction.Citation36
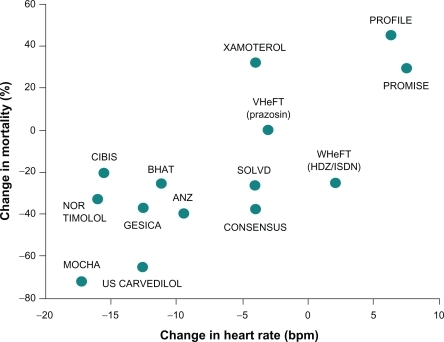
Numerous studies have established a relationship between reduction in HR and improved survival of patients with HF who are receiving β-blocker therapy ().Citation37 In a recent meta-analysis of 35 studies of patients with chronic systolic HF (n = 22,926), a strong correlation was observed between HR and annualized all-cause mortality (P = 0.004) and between change in HR and change in left ventricular ejection fraction (P < 0.001).Citation38 As a result, it was suggested that the HR-lowering effect of β-blockers was a major contributor to the clinical benefit associated with these agents. In a study of 152 patients with HF who were receiving β-blocker therapy, greater reductions in HR were associated with better clinical outcomes for patients overall, and higher β-blocker doses provided additional clinical benefits among patients with persistently elevated HR.Citation39 These results suggest that the magnitude of reduction in HR may be more important than achieving the target dose of β-blocker therapy in patients with HF.Citation38,Citation39 In the Cardiac Insufficiency BIsoprolol Study (CIBIS), treatment of 557 patients with bisoprolol reduced HR by approximately 15 beats/minute relative to placebo (P < 0.001), and HR change was the most powerful predictor of survival (P < 0.01).Citation40 In the larger CIBIS II study (n = 2539), baseline HR and HR change were both significant predictors of mortality (P ≤ 0.005).Citation41 The most favorable prognosis occurred in patients with the lowest baseline HR and with the greatest HR reduction, conditions which were encountered more frequently in the bisoprolol group than in the placebo group.
Figure 3 Heart rate reduction and mortality in heart failure: Relationship between change in heart rate and mean change in mortality among patients with chronic heart failure who received β-blocker therapy. Copytright © 1999. Reprinted with permission from Kjekshus Kjekshus J, Gullestad L. Heart rate as a therapeutic target in heart failure. Eur Heart J Suppl. 1999;1(Suppl H):H64–H69.
The Carvedilol Post-Infarct Survival Control in Left Ventricular Dysfunction (CAPRICORN) trial evaluated patients with left ventricular dysfunction or HF after a myocardial infarction (n = 1959),Citation42 whereas the Carvedilol Prospective Randomized Cumulative Survival (COPERNICUS) trial enrolled only patients with severe HF (n = 2289).Citation43 The Metoprolol CR/XL Randomized Intervention Trial in Congestive Heart Failure (MERIT-HF) enrolled patients with New York Heart Association Class II–IV HF with an ejection fraction <40% (n = 3991).Citation44 These trials each independently demonstrated benefits of β-blockade in patients with HF throughout a large spectrum of disease. Additionally, the Carvedilol or Metoprolol (tartrate) European Trial (COMET; n = 3029) may suggest that nonselective neurohumoral blockade has an additional benefit compared with selective β1-blockade.Citation45 Consequently, adrenergic-receptor pathophysiology and thereafter specific signal transduction pathways may underlie the benefit of using specific β-blockers.Citation46 Although studies using one of the three β-blockers approved for HF in the US (carvedilol, metoprolol succinate, or bisoprolol) have demonstrated benefit in patients with HF, nebivolol has also received approval in Europe for the treatment of mild-to-moderate HF in patients ≥70 years of age.Citation47 Nebivolol is a β1-selective β-blocker without α1-adrenergic receptor blocking activity. Nebivolol, which is approved for the treatment of hypertension in the US, has a neutral effect on metabolic parameters in patients with hypertension.Citation48 Nebivolol has been shown to reduce BP and HR to a similar extent as atenolol at one-tenth of the dose.Citation49 More importantly, the hemodynamic effect observed with nebivolol treatment better preserved cardiac output by decreasing peripheral vascular resistance and increasing stroke volume compared with atenolol.Citation50
Comparison of bisoprolol, carvedilol, and nebivolol in patients with HF demonstrated that each agent decreased HR to a similar extent.Citation51 Additionally, exercise capacity increases during β-blocker therapy. For example, among 16 healthy male volunteers, HR during exercise decreased by 14% in the bisoprolol group, 15% in the carvedilol group, and 13% in the nebivolol group (P < 0.05).Citation51 Additionally, the effect of carvedilol and nebivolol on exercise capacity were compared in a 12-month study of patients with nonischemic dilated cardiomyopathy.Citation52 Exercise duration improved significantly in both groups of patients (P = 0.01), although patients treated with nebivolol experienced an initial decrease in exercise capacity over the first three months.Citation52 In patients with HF, reduction in peak VO2 is associated with left ventricular systolic dysfunction and increased neurohormonal response. Treatment with carvedilol improved left ventricular systolic function, exercise tolerance (at 12 months, exercise was prolonged by 143.9 sec; P = 0.001), and peak oxygen consumption as well as significant reductions in brain natriuretic peptide, endothelin-1, and associated cytokines (ie, interleukin-6 and tumor necrosis factor-α).Citation53 In a recent analysis of 47 randomized studies of HF, a significant increase in the six-minute walk test was observed in three of 17 studies that involved β-blocker therapy.Citation54 Similar to the results of exercise treadmill tests, patients who received β-blocker therapy for more severe HF experienced greater improvements in the six-minute walk test compared with those having milder HF. Therefore, administration of β-blocker therapy to patients with HF is associated with improved HR control, improvement in clinical functioning, and reduction in mortality and hospitalization risk. The benefits of β-blocker therapy are clear, ie, mortality and HF hospital admissions are reduced by approximately one-third when eligible patients receive β-blocker therapy.Citation55,Citation56
Chronotropic incompetence in heart failure
Patients with HF experience severe chronic exercise intolerance. Although the pathophysiology of exercise intolerance is not completely understood, chronotropic incompetence, defined as an impaired capacity to increase HR during exercise, and diastolic dysfunction are important determinants of this condition.Citation57 Chronotropic incompetence occurs in >70% of patients with advanced HF and is believed to arise as a result of β-receptor desensitization and impaired norepinephrine release.Citation58 Risk factors for the development of chronotropic incompetence include increased left ventricular mass, enlarged cavity size, and depressed systolic function.Citation59 Chronotropic incompetence is predictive of mortality and coronary artery disease risk, even after adjusting for age, physical fitness, and other standard cardiovascular risk factors.Citation60 Although some studies have reported that chronotropic incompetence was more common in patients taking β-blockers,Citation61 β-blockade has been reported to have a minimal effect on the association between chronotropic incompetence and cardiovascular mortality.Citation62,Citation63 At doses <10 mg, nebivolol did not attenuate the exercise-induced increase in HR, thereby suggesting that nebivolol may mitigate the risk of chronotropic incompetence suggested to occur with β-blockade.Citation64 Similarly, carvedilol dose did not affect the HR dynamics during treadmill exercise testing among patients with HF who were stratified by resting HR ≤ (60 beats/minute or >60 beats/minute).Citation65 In a trial comparing the β1 effects of metoprolol succinate and carvedilol, carvedilol did not attenuate exercise-induced HR to the same degree as metoprolol.Citation66 Cardiac pacing may be required to restore chronotropic competence and exercise capacity in patients with persistent bradycardia, as well as allowing for continued β-blocker therapy.Citation67 There is a developing body of literature regarding the treatment of diastolic HF and chronotropic incompetence, but the clinical relevance of this information has yet to be determined.
Heart rate control after myocardial infarction
Increased HR in patients with atherosclerosis may impair the stability of coronary plaques because of repetitive changes in BP that induce mechanical stress. Increased HR (> 80 beats/minute) is associated with more plaque ruptures compared with lower HR in patients with coronary artery disease (n = 106).Citation68 HRs in patients following MI are higher than in patients who have not experienced an acute event.Citation69 Consequently, HR has been identified as an independent risk factor for the development of plaque rupture. In addition, HR but not HRV was identified as an independent prognostic indicator of mortality in a study of 366 patients after MI (P < 0.001).Citation70 However, a subsequent study reported that decreased HRV and increased randomness of HR shortly after MI are independent risk factors for mortality in this patient population.Citation71 Similar to HF, increased HR or reduced HRV are associated with increased cardiovascular mortality in patients after MI.Citation32 A meta-analysis of the GISSI-2 and GISSI-3 trials that included approximately 20,000 patients demonstrated that inhospital mortality rates after MI increased from 3% for patients with HR <60 beats/minute on admission to 10% for patients with HR >100 beats/minute on admission.Citation72 Furthermore, higher HR at hospital discharge correlated with increased mortality rates after one year.Citation69
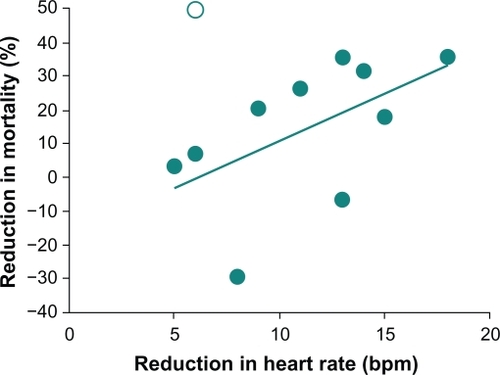
Traditional β-blockers exert beneficial effects on HR and HRV and improve mortality rates in patients who have experienced an MI. Administration of β-blockers to 1427 patients within six hours of the onset of MI symptoms resulted in a mean reduction in infarct size that was directly proportional to the mean reduction in HR (P < 0.001).Citation73 Furthermore, a significant association was reported between reduction in HR and reduction in mortality in 11 long-term β-blocker studies that involved more than 16,000 patients (; r = 0.60; P < 0.05).Citation73 The Norwegian Timolol study reported similar results in that β-blocker-mediated HR reductions in patients who had experienced an MI were a significant predictor of overall mortality.Citation74 Compared with placebo, timolol treatment was associated with a 42% reduction in overall mortality compared with placebo (P < 0.001); in logistic regression analysis, HR during follow-up remained predictive but treatment did not, suggesting that the beneficial effect of timolol on mortality could be ascribed to its effect on HR. HRV was also significantly improved among 28 patients who were treated with atenolol or metoprolol tartrate for six weeks after an acute MI (P ≤ 0.01); trends toward lower HR were also observed in both treatment groups.Citation2 Similarly, treatment of 30 patients who were stable following an MI with atenolol or metoprolol controlled-release (succinate) for six weeks decreased HR (P < 0.001) and increased HRV.Citation75 Propranolol treatment was also associated with significantly greater improvements in HRV after an acute MI compared with placebo (P <0.05; n =184). Citation76
Figure 4 Heart rate reduction and mortality after myocardial infarction: Relationship between mean reduction in heart rate and mean change in mortality relative to placebo in randomized, placebo-controlled studies of β-blockers after myocardial infarction (r = 0.60; P < 0.05). Copyright © 1986. Reprinted with permission from Kjekshus JK. Importance of heart rate in determining beta-blocker efficacy in acute and long-term acute myocardial infarction intervention trials.Am J Cardiol. 1986;57(12):43F–49F.
Similar to the traditional β-blockers, vasodilating β-blockers exert beneficial effects on HR and HRV in patients who have experienced an MI. Carvedilol produced reductions in HR relative to placebo in 151 patients with an acute MI (P < 0.0001).Citation77 Labetalol, a nonselective β-blocker that targets α1-, β1-, and β2-adrenergic receptors, is used for the treatment of hypertension of all severities and during hypertensive emergencies.Citation78,Citation79 When given acutely, labetalol decreases peripheral vascular resistance and BP but may have limited effects on HR and cardiac output.Citation80 In another study, administration of labetalol to 32 patients with sustained elevations in systemic arterial pressure after a recent MI resulted in significant reductions in HR relative to pretreatment levels (P < 0.01).Citation81 Nebivolol and atenolol both decreased HR in patients who had ischemic heart disease and a previous MI (n = 40); however, nebivolol maintained cardiac output and improved ejection fraction (P < 0.05).Citation82 The relationship between improved HR control and decreased mortality has not been assessed among patients who have been treated with vasodilating β-blockers after MI.
Heart rate control in hypertension
In patients with hypertension, sympathetic nervous system overactivity increases HR, contributing to cardiac output and raised BP. The association between increased HR and the development of hypertension was demonstrated in the HARVEST (Hypertension and Ambulatory Recording VEnetia STudy) trial, which revealed a strong linkage between elevated HR and increases in BP among patients with Stage 1 hypertension.Citation83 Patients whose HR was persistently elevated during the six-year study period had a two-fold higher risk of developing hypertension compared with patients with normal HR (n = 796). In patients with hypertension, normal sinus rhythm, and cardiovascular risk factors (n = 18,900), increasing HR from 81 to 119 beats/minute was associated with an increasing proportion of patients with microalbuminuria (63% to 69%, respectively; P < 0.0001).Citation84 Elevated HR is also an independent predictor of microalbuminuria, a predictor for cardiovascular events, and an indicator of renal impairment in patients with hypertension (n = 18,900).Citation84 In addition, greater impairment of HRV responsiveness to autonomic challenge was observed in patients with hypertension compared with a normotensive group (n = 40).Citation85 Increased HR generally results in a poor prognosis for patients with hypertension. The rate of complications caused by cardiovascular disease as well as total mortality in patients with hypertension increased two-fold when HR increased by 40 beats/minute (n =4530). Citation86
The importance of lowering systemic vascular resistance and increasing tissue perfusion in patients with hypertension is well recognized, given that clinical evidence has established an association between impairment of microcirculation and development of end organ damage.Citation87,Citation88 Consequently, a goal of hypertension management is effective BP reduction while maintaining tissue perfusion. Traditional β-blockers reduce BP via decreased cardiac output but do not directly affect central aortic pressure or peripheral resistance, although a slight compensatory increase in peripheral resistance may occur.Citation9 Administration of the traditional β-blocker, atenolol, to patients with hypertension significantly reduced HRV compared with placebo or losartan (P < 0.05).Citation89,Citation90 HR and BP at rest and during exercise was decreased in 10 patients with mild to moderate hypertension who received atenolol therapy for five years; however, systemic vascular resistance was elevated and cardiac output remained depressed compared with pretreatment levels.Citation91 Similar results have also been reported using 10 different traditional β-blockers.Citation9 Therefore, although traditional β-blockers lower BP, they do not appear to normalize cardiac hemodynamics in patients with hypertension. In addition, traditional β-blockers are associated with an increased risk for the development of abnormalities in metabolic parameters (eg, diabetes or endothelial dysfunction) or stroke compared with other antihypertensive agents.Citation92–Citation94
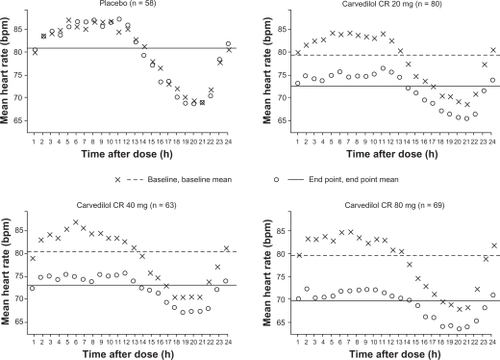
Vasodilatory β-blockers reduce BP via the lowering of peripheral vascular resistance and only slightly decreased in cardiac output; decreases in central aortic pressure have also been observed with vasodilatory β-blockers.Citation79,Citation95 In contrast with traditional β-blockers, carvedilol was shown to maintain cardiac output, decrease vascular resistance, and decrease HR to a lesser extent.Citation96 A once-daily formulation of the vasodilatory β-blocker carvedilol controlled-release was administered to 320 patients with hypertension, resulting in greater reductions in HR () and 24-hour diastolic BP compared with placebo (P ≤ 0.001).Citation97 In the Glycemic Effects in Diabetes Mellitus: Carvedilol-Metoprolol Comparison in Hypertensives (GEMINI) study of 1235 patients with hypertension and Type 2 diabetes mellitus, reductions in diastolic BP were similar in the carvedilol and metoprolol tartrate treatment groups (10.0 ± 0.4 and 10.3 ± 0.3 mmHg, respectively). At mean doses required to achieve target BP (carvedilol 35 mg/day; metoprolol 256 mg/day), both agents effectively reduced HR, although decreases were less among carvedilol- versus metoprolol-treated patients (6.7 ± 0.4 versus 8.3 ± 0.4 beats/minute, respectively; P < 0.001).Citation98 Of clinical importance, carvedilol demonstrated neutral or positive effects on glycemic control and lipid metabolism in analyses of the GEMINI study. After six weeks of treatment, once-daily nebivolol reduced HR by 10.6 ± 10.3 beats/minute, systolic BP by 29 ± 17 mmHg, and diastolic BP by 16 ± 10 mmHg in an observational study of 6376 patients with hypertension.Citation99 Patients with higher initial values experienced greater reductions in HR and BP compared with patients having moderately elevated initial values.Citation99 In other clinical trials, nebivolol reduced vascular resistance and improved endothelial function in patients with hypertension, and also lowered the levels of the inflammatory marker, high-sensitivity C-reactive protein, in healthy volunteers who smoked cigarettes.Citation100,Citation101
Figure 5 Twenty-four-hour heart rate in patients with hypertension at baseline and after six weeks of treatment with carvedilol controlled-release (CR) or placebo. Copyright © 2006. Reprinted with permission from Weber MA, Bakris GL, Tarka EA, Iyengar M, Fleck R, Sica DA. Efficacy of a once-daily formulation of carvedilol for the treatment of hypertension. J Clin Hypertens (Greenwich). 2006;8(12):840–849.
The clinical relevance of β-blocker-mediated HR control to long-term clinical outcomes is less clear in hypertension than in HF or after MI. However, it is clear that reducing peripheral vascular resistance with a vasodilatory β-blocker is a beneficial mechanism to patients with hypertension, ie, a state of inherently elevated peripheral vascular resistance. In addition, vasodilating β-blockers maintain cardiac output but decrease peripheral vascular resistance, which improves peripheral blood flow. Improved blood flow is a major contributing factor to the more favorable tolerability and metabolic profiles of vasodilating β-blockers compared with traditional β-blockers.Citation48,Citation98
Recently, the use of β-blockade in essential hypertension has been called into question. Bangalore et al report increased cardiac events in hypertensive patients being treated with β-blockade.Citation102 A lower HR achieved from β-blockade compared with other antihypertensives or placebo in a meta-analysis of over 34,000 patients with hypertension was associated with an increase in all-cause mortality, cardiovascular mortality, MI, stroke, and HF. One caveat to this study, however, is that 78% of those studied were prescribed atenolol, and it has been suggested that atenolol, and not β-blockade itself, was the cause. The results were certainly provocative, and clearly additional testing needs to be conducted to determine whether this is a class effect or an effect based on receptor specificity.Citation46
Conclusion
An elevated or invariant HR is associated with the development of complications or various cardiovascular diseases including HF, MI, and hypertension. Patients with impaired HR control are at increased risk for all-cause and cardiovascular mortality, especially sudden cardiac death. As a result, HR should be included among the major risk factors for cardiovascular disease and should be used to establish individual cardiovascular risk profiles. Epidemiologic studies have demonstrated that β-blockers improve HR control and decrease mortality in patients with cardiovascular disease. Clinical evidence has established a clear relationship between improved HR control and decreased mortality in patients who have had an MI or who have HF. Although HR is an important contributor to the development of hypertension, a definite association between improved HR control and decreased mortality has yet to be established in this patient population. However, the importance of decreased peripheral vascular resistance while maintaining tissue perfusion is well recognized in patients with certain cardiovascular conditions, such as hypertension. Traditional β-blockers do not decrease but may in fact increase peripheral vascular resistance during long-term treatment. In contrast, vasodilating β-blockers reduce peripheral vascular resistance and maintain cardiac output. Consequently, vasodilating β-blockers are an appropriate treatment option for patients with cardiovascular disease who are at high risk of sudden cardiac death, HF, or coronary artery disease, and for those with concordant comorbidities, including diabetes and peripheral vascular disease.
Acknowledgements
ProEd Communications provided editorial assistance with this paper and was supported by GlaxoSmithKline, Philadelphia, Pennsylvania.
Disclosures
DF has received grant support from NIH Grant HL084498, NIH Grant HD 058997, the Heart Failure Society of America, the GlaxoSmithKline Research Fund, and the Medtronic Research Fund. TE has received grant support from NIH Grant HL 48848 and NIH Grant HD-58997. RW has received grant support from the Pfizer Fellowship in Health Disparities, the American Academy of Family Physicians Foundation, Cardiomems DSMB, and CVRx Research. DM declares no conflicts of interest in this work.
References
- LanzaGAFoxKCreaFHeart rate: A risk factor for cardiac diseases and outcomes? Pathophysiology of cardiac diseases and the potential role of heart rate slowingAdv Cardiol200643116
- LurjeLWennerblomBTygesenHKarlssonTHjalmarsonAHeart rate variability after acute myocardial infarction in patients treated with atenolol and metoprololInt J Cardiol19976021571649226286
- LonnEGrewalJDrug therapies in the secondary prevention of cardiovascular diseases: Successes, shortcomings and future directionsCurr Vasc Pharmacol200643253268
- PoulterNRDobsonJESeverPSDahlofBWedelHCampbellNRBaseline heart rate, antihypertensive treatment, and prevention of cardiovascular outcomes in ASCOT (Anglo – Scandinavian Cardiac Outcomes Trial)J Am Coll Cardiol2009541311541161
- FrishmanWHA historical perspective on the development of β-adrenergic blockersJ Clin Hypertens200794 Suppl 31927
- EganBMBasileJChiltonRJCohenJDCardioprotection: The role of beta-blocker therapyJ Clin Hypertens (Greenwich)200577409416
- Lopez-SendonJSwedbergKMcMurrayJExpert consensus document on beta-adrenergic receptor blockersEur Heart J2004251513411362
- BakrisGLHartPRitzEBeta blockers in the management of chronic kidney diseaseKidney Int200670111905191317021610
- MesserliFHGrossmanEBeta-blockers in hypertension: Is carvedilol different?Am J Cardiol2004939A7B12B
- BrocqMLLeslieSJMillikenPMegsonILEndothelial dysfunction: From molecular mechanisms to measurement, clinical implications, and therapeutic opportunitiesAntioxid Redox Signal200810916311674
- KrumHSympathetic activation and the role of beta-blockers in chronic heart failureAust N Z J Med1999293418427
- ManciaGGrassiGGiannattasioCSeravalleGSympathetic activation in the pathogenesis of hypertension and progression of organ damageHypertension1999344 Pt 272472810523349
- De JongMJRandallDCHeart rate variability analysis in the assessment of autonomic function in heart failureJ Cardiovasc Nurs2005203186195quiz 196–19715870589
- FeldmanDSEltonTSSunBMartinMMZioloMTMechanisms of disease: Detrimental adrenergic signaling in acute decompensated heart failureNat Clin Pract Cardiovasc Med200854208218
- FoxKBorerJSCammAJResting heart rate in cardiovascular diseaseJ Am Coll Cardiol2007509823830
- DiazABourassaMGGuertinMCTardifJCLong-term prognostic value of resting heart rate in patients with suspected or proven coronary artery diseaseEur Heart J2005261096797415774493
- JouvenXEmpanaJPSchwartzPJDesnosMCourbonDDucimetierePHeart-rate profile during exercise as a predictor of sudden deathN Engl J Med2005352191951195815888695
- LeeKLWoodliefLHTopolEJPredictors of 30-day mortality in the era of reperfusion for acute myocardial infarction. Results from an international trial of 41,021 patients. GUSTO-I InvestigatorsCirculation199591616591668
- KannelWBRisk stratification in hypertension: New insights from the Framingham StudyAm J Hypertens2000131 Pt 23S10S
- WilhelmsenLBerglundGElmfeldtDThe multifactor primary prevention trial in Goteborg, SwedenEur Heart J198674279288
- DyerARPerskyVStamlerJHeart rate as a prognostic factor for coronary heart disease and mortality: Findings in three Chicago epidemiologic studiesAm J Epidemiol19801126736749
- GillumRFMakucDMFeldmanJJPulse rate, coronary heart disease, and death: The NHANES I Epidemiologic Follow-up StudyAm Heart J19911211 Pt 1172177
- GoldbergRJLarsonMLevyDFactors associated with survival to 75 years of age in middle-aged men and women. The Framingham StudyArch Intern Med19961565505509
- KannelWBWilsonPBlairSNEpidemiological assessment of the role of physical activity and fitness in development of cardiovascular diseaseAm Heart J19851094876885
- SinghBNMorbidity and mortality in cardiovascular disorders: Impact of reduced heart rateJ Cardiovasc Pharmacol Ther20016431333111907634
- KovarDCannonCPBentleyJHCharlesworthARogersWJDoes initial and delayed heart rate predict mortality in patients with acute coronary syndromes?Clin Cardiol20042728086
- EagleKALimMJDabbousOHA validated prediction model for all forms of acute coronary syndrome: Estimating the risk of 6-month postdischarge death in an international registryJAMA20042912227272733
- MarchioliRAvanziniFBarziFAssessment of absolute risk of death after myocardial infarction by use of multiple-risk-factor assessment equations: GISSI-Prevenzione mortality risk chartEur Heart J200122222085210311686666
- MorrowDAAntmanEMCharlesworthATIMI risk score for ST-elevation myocardial infarction: A convenient, bedside, clinical score for risk assessment at presentation: An intravenous nPA for treatment of infarcting myocardium early II trial substudyCirculation20001021720312037
- ThomsenTFDavidsenMIbsenHJorgensenTJensenGBorch-JohnsenKA new method for CHD prediction and prevention based on regional risk scores and randomized clinical trials: PRE-CARD and the Copenhagen Risk ScoreJ Cardiovasc Risk200185291297
- ConroyRMPyoralaKFitzgeraldAPEstimation of ten-year risk of fatal cardiovascular disease in Europe: The SCORE projectEur Heart J20032411987100312788299
- ChattipakornNIncharoenTKanlopNChattipakornSHeart rate variability in myocardial infarction and heart failureInt J Cardiol2007120328929617349699
- Heart rate variability: Standards of measurement, physiological interpretation and clinical use. Task Force of the European Society of Cardiology and the North American Society of Pacing and ElectrophysiologyCirculation1996935104310658598068
- ReilJCBohmMThe role of heart rate in the development of cardiovascular diseaseClin Res Cardiol2007969585592
- YoungJBSudden cardiac death syndrome and pump dysfunction: The linkJ Heart Lung Transplant200019Suppl 8S27S31
- NesslerJNesslerBKitlinskiMSudden cardiac death risk factors in patients with heart failure treated with carvedilolKardiol Pol2007651214171422discussion 1423–142418181053
- KjekshusJGullestadLHeart rate as a therapeutic target in heart failureEur Heart J Suppl19991Suppl HH64H69
- FlanneryGGehrig-MillsRBillahBKrumHAnalysis of randomized controlled trials on the effect of magnitude of heart rate reduction on clinical outcomes in patients with systolic chronic heart failure receiving beta-blockersAm J Cardiol2008101686586918328855
- HuangRLListermanJGoringJGiesbergCNadingMAButlerJBeta-blocker therapy for heart failure: Should the therapeutic target be dose or heart rate reduction?Congest Heart Fail200612420610quiz 211–212
- LechatPEscolanoSGolmardJLPrognostic value of bisoprolol-induced hemodynamic effects in heart failure during the Cardiac Insufficiency BIsoprolol Study (CIBIS)Circulation1997967219722059337190
- LechatPHulotJSEscolanoSHeart rate and cardiac rhythm relationships with bisoprolol benefit in chronic heart failure in CIBIS II TrialCirculation2001103101428143311245648
- DargieHJEffect of carvedilol on outcome after myocardial infarction in patients with left-ventricular dysfunction: The CAPRICORN randomised trialLancet2001357926613851390
- PackerMCoatsAJFowlerMBEffect of carvedilol on survival in severe chronic heart failureN Engl J Med2001344221651165811386263
- Effect of metoprolol CR/XL in chronic heart failure: Metoprolol CR/XL Randomised Intervention Trial in Congestive Heart Failure (MERIT-HF)Lancet1999353916920012007
- Poole-WilsonPASwedbergKClelandJGComparison of carvedilol and metoprolol on clinical outcomes in patients with chronic heart failure in the Carvedilol Or Metoprolol European Trial (COMET): Randomised controlled trialLancet2003362937771312853193
- FeldmanDSCarnesCAAbrahamWTBristowMRMechanisms of disease: Beta-adrenergic receptors – alterations in signal transduction and pharmacogenomics in heart failureNat Clin Pract Cardiovasc Med200529475483
- Veteran’s Health Administration Pharmacy Benefits Management Services and the Medical Advisory PanelNational PBM drug monograph: Nebivolol (Bystolic)20086 www.pbm.va.gov/monograph/Nebivolol.doc. Accessed Feb 18, 2009
- Agabiti RoseiERizzoniDMetabolic profile of nebivolol, a beta-adrenoceptor antagonist with unique characteristicsDrugs200767810971107
- SimonGJohnsonMLComparison of antihypertensive and beta 1-adrenoceptor antagonist effect of nebivolol and atenolol in essential hypertensionClin Exp Hypertens19931535015098098243
- KampOSieswerdaGTVisserCAComparison of effects on systolic and diastolic left ventricular function of nebivolol versus atenolol in patients with uncomplicated essential hypertensionAm J Cardiol2003923344348
- StoschitzkyKStoschitzkyGBrusseeHBonelliCDobnigHComparing beta-blocking effects of bisoprolol, carvedilol and nebivololCardiology20061064199206
- PatrianakosAPParthenakisFIMavrakisHEDiakakisGFChlouverakisGIVardasPEComparative efficacy of nebivolol versus carvedilol on left ventricular function and exercise capacity in patients with nonischemic dilated cardiomyopathy. A 12-month studyAm Heart J20051505985
- NesslerJNesslerBKitlinskiMGackowskiAPiwowarskaWStepniewskiMConcentration of BNP, endothelin 1, pro-inflammatory cytokines (TNF-alpha, IL-6) and exercise capacity in patients with heart failure treated with carvedilolKardiol Pol2008662144151discussion 152–15318344152
- OlssonLGSwedbergKClarkALWitteKKClelandJGSix minute corridor walk test as an outcome measure for the assessment of treatment in randomized, blinded intervention trials of chronic heart failure: A systematic reviewEur Heart J2005268778793
- JafriSMThe effects of beta blockers on morbidity and mortality in heart failureHeart Fail Rev200492115121
- ShibataMCFlatherMDWangDSystematic review of the impact of beta blockers on mortality and hospital admissions in heart failureEur J Heart Fail20013335135711378007
- KitzmanDWExercise intoleranceProg Cardiovasc Dis2005476367379
- JordeUPVittorioTJKasperMEChronotropic incompetence, beta-blockers, and functional capacity in advanced congestive heart failure: Time to pace?Eur J Heart Fail200810196101
- LauerMSLarsonMGEvansJCLevyDAssociation of left ventricular dilatation and hypertrophy with chronotropic incompetence in the Framingham Heart StudyAm Heart J1999137590390910220640
- LauerMSOkinPMLarsonMGEvansJCLevyDImpaired heart rate response to graded exercise. Prognostic implications of chronotropic incompetence in the Framingham Heart StudyCirculation1996938152015268608620
- WitteKKClarkALChronotropic incompetence in heart failureJ Am Coll Cardiol2006483595author reply 595–596
- KhanMNPothierCELauerMSChronotropic incompetence as a predictor of death among patients with normal electrograms taking beta blockers (metoprolol or atenolol)Am J Cardiol20059691328133316253608
- MyersJTanSYAbellaJAletiVFroelicherVFComparison of the chronotropic response to exercise and heart rate recovery in predicting cardiovascular mortalityEur J Cardiovasc Prev Rehabil2007142215221
- WeissRNebivolol: A novel beta-blocker with nitric oxide-induced vasodilatationVasc Health Risk Manag200623303308
- CarvalhoVORodrigues AlvesRXBocchiEAGuimaraesGVHeart rate dynamic during an exercise test in heart failure patients with different sensibilities of the carvedilol therapy Heart rate dynamic during exercise testInt J Cardiol2009118[Epub ahead of print]
- VittorioTJZoltyRKasperMEDifferential effects of carvedilol and metoprolol succinate on plasma norepinephrine release and peak exercise heart rate in subjects with chronic heart failureJ Cardiovasc Pharmacol Ther20081315157
- SteckerECFendrickAMKnightBPAaronsonKDProphylactic pacemaker use to allow beta-blocker therapy in patients with chronic heart failure with bradycardiaAm Heart J20061514820828
- HeidlandUEStrauerBELeft ventricular muscle mass and elevated heart rate are associated with coronary plaque disruptionCirculation20011041314771482
- HjalmarsonAGilpinEAKjekshusJInfluence of heart rate on mortality after acute myocardial infarctionAm J Cardiol19906595475531968702
- AbildstromSZJensenBTAgnerEHeart rate versus heart rate variability in risk prediction after myocardial infarctionJ Cardiovasc Electrophysiol2003142168173
- SteinPKDomitrovichPPHuikuriHVKleigerRETraditional and nonlinear heart rate variability are each independently associated with mortality after myocardial infarctionJ Cardiovasc Electrophysiol20051611320
- ZuanettiGHernndes-BernalFRossiAComerioGPaolucciGMaggioniAPRelevance of heart rate as a prognostic factor in myocardial infarction: The GISSI experienceEur Heart J Suppl19991Suppl HH52H57
- KjekshusJKImportance of heart rate in determining beta-blocker efficacy in acute and long-term acute myocardial infarction intervention trialsAm J Cardiol1986571243F49F
- GundersenTGrottumPPedersenTKjekshusJKEffect of timolol on mortality and reinfarction after acute myocardial infarction: Prognostic importance of heart rate at restAm J Cardiol19865812024
- TuiningaYSCrijnsHJBrouwerJEvaluation of importance of central effects of atenolol and metoprolol measured by heart rate variability during mental performance tasks, physical exercise, and daily life in stable postinfarct patientsCirculation19959212341534238521562
- LampertRIckovicsJRViscoliCJHorwitzRILeeFAEffects of propranolol on recovery of heart rate variability following acute myocardial infarction and relation to outcome in the Beta-Blocker Heart Attack TrialAm J Cardiol2003912137142
- BasuSSeniorRRavalUvan der DoesRBrucknerTLahiriABeneficial effects of intravenous and oral carvedilol treatment in acute myocardial infarction. A placebo-controlled, randomized trialCirculation1997961183191
- LouisWJMcNeilJJDrummerOHPharmacology of combined alpha-beta-blockade. IDrugs198428Suppl 21634
- PedersenMECockcroftJRThe vasodilatory beta-blockersCurr Hypertens Rep200794269277
- MacCarthyEPBloomfieldSSLabetalol: A review of its pharmacology, pharmacokinetics, clinical uses and adverse effectsPharmacotherapy1983341932196310529
- VermaSPSilkeBHussainMSympathetic (alpha-beta) or calcium channel blockade for hypertensive myocardial infarction? A haemodynamic comparison of labetalol and nifedipineJ Hypertens1988611897904
- StoleruLWijnsWvan EyllCBouvyTVan NuetenLPouleurHEffects of D-nebivolol and L-nebivolol on left ventricular systolic and diastolic function: Comparison with D-L-nebivolol and atenololJ Cardiovasc Pharmacol1993222183190
- PalatiniPGranieroGRMorminoPRelation between physical training and ambulatory blood pressure in stage I hypertensive subjects. Results of the HARVEST Trial. Hypertension and Ambulatory Recording Venetia StudyCirculation199490628702876
- BohmMReilJCDanchinNThoenesMBramlagePVolpeMAssociation of heart rate with microalbuminuria in cardiovascular risk patients: Data from I-SEARCHJ Hypertens2008261182518090536
- MadsenLBRasmussenJKMollerDSNyvadOPedersenEBHeart rate variability in white-coat hypertensionBlood Press Monit20081326571
- GillmanMWKannelWBBelangerAD’AgostinoRBInfluence of heart rate on mortality among persons with hypertension: The Framingham StudyAm Heart J1993125411481154
- LevyBImportance of improving tissue perfusion during treatment of hypertensionJ Hypertens Suppl2006245S6S9
- LevyBI[The importance of microcirculation and tissue perfusion in hypertension]Curr Med Res Opin200521Suppl 5S1S6
- CampeloMPoloniaJSerraoPCerqueira-GomesMEvaluation of the sympathetic nervous system using heart rate variability and plasma hormones in hypertensive patients treated with cilazapril and atenololCardiology1996875402408
- ChernCMHsuHYHuHHChenYYHsuLCChaoACEffects of atenolol and losartan on baroreflex sensitivity and heart rate variability in uncomplicated essential hypertensionJ Cardiovasc Pharmacol2006472169174
- Lund-JohansenPHemodynamic consequences of long-term beta-blocker therapy: A 5-year follow-up study of atenololJ Cardiovasc Pharmacol197915487495
- BangaloreSParkarSGrossmanEMesserliFHA meta-analysis of 94,492 patients with hypertension treated with beta blockers to determine the risk of new-onset diabetes mellitusAm J Cardiol200710081254126217920367
- BradleyHAWiysongeCSVolminkJAMayosiBMOpieLHHow strong is the evidence for use of beta-blockers as first-line therapy for hypertension? Systematic review and meta-analysisJ Hypertens200624112131214117053529
- CruickshankJMAre we misunderstanding beta-blockersInt J Cardiol200712011027
- SarafidisPABakrisGLDo the metabolic effects of beta blockers make them leading or supporting antihypertensive agents in the treatment of hypertension?J Clin Hypertens (Greenwich)200685351356quiz 357–35816687944
- StafylasPCSarafidisPACarvedilol in hypertension treatmentVasc Health Risk Manag200841233018629377
- WeberMABakrisGLTarkaEAIyengarMFleckRSicaDAEfficacy of a once-daily formulation of carvedilol for the treatment of hypertensionJ Clin Hypertens (Greenwich)2006812840849
- BakrisGLFonsecaVKatholiREMetabolic effects of carvedilol vs metoprolol in patients with type 2 diabetes mellitus and hypertension: A randomized controlled trialJAMA2004292182227223615536109
- von FalloisJFaulhaberHD[Nebivolol, a third generation beta blocker: the modern treatment of hypertension. Results of a multicentric observational study]Fortschr Med Orig2000118Suppl 2778215700490
- MunzelTGoriTNebivolol: The somewhat-different beta-adrenergic receptor blockerJ Am Coll Cardiol2009541614911499
- SchmidtACFlickBJahnEBramlagePEffects of the vasodilating beta-blocker nebivolol on smoking-induced endothelial dysfunction in young healthy volunteersVasc Health Risk Manag20084490991519066009
- BangaloreSSawhneySMesserliFHRelation of beta-blocker-induced heart rate lowering and cardioprotection in hypertensionJ Am Coll Cardiol2008521814821489