Abstract
Of particular concern to India is not only the high burden of cardiovascular diseases (CVDs), but also the effects of these diseases on the productive workforce aged 35–65 years. Heart diseases are rising in Asian Indians 5–10 years earlier than in other populations around the world. The mean age for first presentation of acute myocardial infarction in Indians is 53 years. Coronary artery disease (CAD) that manifests at a younger age can have devastating consequences for an individual, the family, and society. Prevention of these deaths in young people is a nation's moral responsibility. A strategy involving prevention of CVDs long before their onset will be more cost-effective than providing interventions at a stage when the disease is well established. We review the rising trends in CAD with particular emphasis on prevalence of premature CAD and the associated risk factors in young Indian CAD patients. Action strategies to reduce the risk are suggested.
Keywords:
Introduction
Persistent health inequalities are a worldwide problem. Alleviation of preventable human suffering caused by inequitable access to healthcare facilities is being advocated globally. But what are the prospects for human health in developing countries where there is an increased threat of adult chronic diseases against a backdrop of the relentless crisis of infectious diseases, environmental degradation, and political indifference? It is time for these developing countries to review and reset their health priorities. Globally, these health priorities are set not only by consideration of health issues pertaining to a particular region but also by selection of information by political and scientific bodies. There are health problems afflicting large numbers of families and communities, but these remain invisible to better-off and protected communities. As a result, some vital health issues find no place in a country's health agenda. A prominent example is that of cardiovascular disease (CVD). Projections show that CVD has reached epidemic proportions in many developing countries. In India, mortality attributable to CVD is expected to rise by 103% in men and by 90% in women from 1985 to 2015 (CitationBulatao and Stephens 1992). More importantly, the disease catches Indians young. Therefore, to stop the ruthless assault of CVD in developing countries, there is an urgent need to represent the disease in the health agenda of these countries.
A cost-effective preventive strategy will need to focus on reducing risk factors both in the individual and in the population at large. However, a key factor that hampers the development of such preventive strategies in developing countries such as India is the meager amount (8%) of published literature on CVD research available from these countries (CitationMackay and Mensah 2004). Much of the knowledge of risk factors for coronary artery disease (CAD) has been acquired from studies conducted in the Western population. It is widely believed that the association of these risk factors with CAD in other populations needs to be ascertained, and there is speculation that differences might range from the frequency of presence of classical risk factors to their total absence or irrelevance in these populations. Therefore it is imperative to undertake large population-based, prospective studies in developing countries such as India to identify CAD risk factors, both conventional and novel. However, careful scrutiny of available scientific evidence for modifiable CAD risk factors (elevated serum total and low-density lipoprotein cholesterol [LDL-C], low high-density lipoprotein cholesterol [HDL-C], smoking, diabetes, hypertension, low level of physical activity, and obesity) in this population may be helpful in formulating a more immediate CAD prevention strategy.
In this article, the word Indian refers to the entire population of India. We review the rising mortality rates due to CAD and premature CAD in this population. Through a review of studies carried out in resident Indians, we discuss the conventional risk factors prevalent in young Indian CAD patients. We have restricted ourselves to well established CAD-associated risk factors, as these are the immediate targets for cardiac event risk reduction worldwide (CitationPearson 2002). To make up the deficiencies in data, we have tried to supplement the information from India with studies from other Asian countries. We suggest that by using the available data, a preventive strategy can be developed for the Indian population.
Rising prevalence of cardiovascular diseases globally
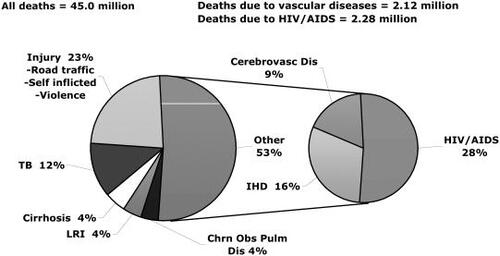
CVDs are no longer confined by geographical area or by age, sex, or socioeconomic boundaries. Heart disease has already reached epidemic proportions in poorer countries. Of the 45.0 million adult deaths reported worldwide in 2002, three-quarters (32 million) were due to noncommunicable diseases (CitationWHO 2003). Except in Africa, noncommunicable diseases outnumbered communicable diseases in all WHO regions worldwide. In Southeast Asia alone, 7 423 000 deaths were due to noncommunicable diseases as compared with 5 730 000 deaths related to communicable diseases in the year 2002. Globally, ischemic heart disease (IHD) was the leading killer in the age group ≥60 years, and, with 1 332 000 deaths in adults aged 15–59 years, IHD was ranked behind HIV/AIDS only ().
Figure 1 Leading causes of death worldwide in 2002 (age 15–59 years). Source: CitationWHO 2003. Abbreviations: Cerebrovasc Dis, cerebrovascular disease; Chrn Obs Pulm Dis, chronic obstructive pulmonary disease; IHD, ischemic heart disease; LRI, lower respiratory infections; TB, tuberculosis.
With 6.8% and 5.0% of disability-adjusted life-years (DALYs) lost, CAD and stroke were globally the second and third largest causes of disease burden in men aged 15 years and older in 2002 (CitationMackay and Mensah 2004). Even in women, CAD and stroke were the third and fourth main causes of DALYs lost worldwide.
Trends of cardiovascular diseases in India
It is well known that the demographic transition in Western countries was accompanied by a decrease in deaths due to infectious diseases and increased mortality due to noncommunicable diseases. India is in the midst of such demographic transition. The average life expectancy at birth in India is 63.7 years, being 63.1 for males and 64.4 for females (CitationIndia – Human Development Fact Sheet 2003), compared with the national average of 41.2 years in 1951–1961 (CitationWorld Bank 1993). There has been a decline in death rate from 1941 to 1971, followed by a sharp decline in birth rate from 1971 onwards (CitationGowarikar 1995). This rise in life expectancy in India is attributed to a decrease in infectious, parasitic, and nutritional disorders and, in itself, is a remarkable achievement. However, this demographic transition has also led to an increase in the number of older people (aged ≥60 years), from 19.61 million in 1950 to 75.93 million in 2000 (CitationSharma and Xenos 1992). The increase in life expectancy has brought a large section of the population to an age where CVD starts manifesting itself.
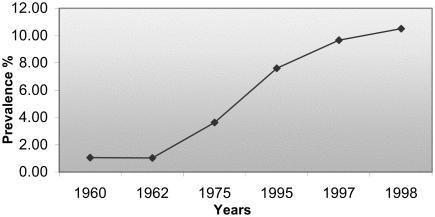
In India, CAD rates have increased during the last 30 years, whereas declining trends have been noticed in developed Western countries (CitationEnas and Senthilkumar 2001). Reports on CAD in Indians from different parts of the world have shown that Asian Indians are at 3–4 times higher risk of CAD than white Americans, 6 times higher than Chinese, and 20 times higher than Japanese (CitationEnas, Garg, et al 1996; CitationGupta 1997; CitationEnas and Yusuf 1999; CitationGhaffar et al 2004). The exact prevalence of CAD in India is difficult to estimate owing to the lack of a large prospective study. Absence of a centralized death registry for CVDs and irregularities in completion of death certificates also hamper estimation of the actual burden of CVD (CitationReddy 1993). However, various independent epidemiological studies (CitationMathur 1960; CitationPadmavati 1962; CitationGupta and Malhotra 1975; CitationGupta et al 1995; CitationChadha et al 1997; CitationReddy 1998) conducted in North India suggest that the prevalence of CAD has increased from 1% in 1960 to 10.5% in 1998 in the urban population (). A higher prevalence of CAD, ranging from 11.0% to 14.2%, has been reported from South India (CitationBegom and Singh 1995; CitationRamachandran et al 1998; CitationMohan et al 2001). In rural India, a twofold increase has been reported in the northern states (CitationDewan et al 1974; CitationHarris and Weissfield 1991; CitationGupta R, Gupta HP, et al 1994; CitationWander et al 1994; CitationSingh et al 1995; CitationGupta R and Gupta VP 1996; CitationReddy 1998). A higher prevalence of 7.4% was observed in some parts of rural South India as long ago as in 1993 (CitationKutty et al 1993). Taking into account the size of the Indian population, these prevalence rates, translated into figures, indicate that a large number of deaths can be attributed to CAD.
Figure 2 Rising trends of cardiovascular disease prevalence in North India. Source: CitationMathur 1960; CitationPadnavati 1962; CitationGupta and Malhotra 1975; CitationGupta et al 1995; CitationChadha et al 1997; CitationReddy 1998.
In view of the trends witnessed in Western countries, it appears inevitable for the initial increase of CAD-related risks in more affluent sections of society to soon permeate all class barriers. Community and case control studies in India are already suggesting an increasing association between lower education or lower income and CAD (CitationGupta R, Gupta VP, et al 1994; CitationPais et al 1996). Compounded by the lower economic status of these socioeconomic groups, the number of CVD-related deaths may rise even above the projected figures. As the existing health infrastructure lacks the capacity to bear the immense burden that CVD will exert, there is an urgent need to stop the progress of this epidemic.
Premature CAD in Indians
Of particular concern to India is not only the high burden of CVDs, but also the effects of CVD on the productive workforce aged 35–65 years. The salient features of the CAD epidemic in India are listed in . The incidence of CAD in the young has been reported to be 12%–16% in Indians (CitationMammi et al 1991; CitationNegus et al 1994). Half of the CVD-related deaths (ie, 52% of CVDs) in India occur below the age of 50 years, and about 25% of acute myocardial infarction (MI) in India occurs under the age of 40 years (CitationMurray and Lopez 1994; CitationEnas and Senthilkumar 2001).
Table 1 Salient features of the coronary artery disease (CAD) epidemic in India
Heart diseases are occurring in Indians 5 to 10 years earlier than in other populations around the world (CitationHughes et al 1989; CitationEnas, Dhawan, et al 1996). According to the INTERHEART study, the median age for first presentation of acute MI in the South Asian (Bangladesh, India, Nepal, Pakistan, Sri Lanka) population is 53 years, whereas that in Western Europe, China, and Hong Kong is 63 years, with more men than women affected (CitationYusuf et al 2004). Data from the Singapore Myocardial Infarction Registry from 1988 to 1997 for acute MI cases aged between 20 and 64 years also showed that men were four times more prone to these events than women (CitationKam et al 2002). The median age for presentation of first MI was higher in Asian women than in Asian men (58 and 54 years, respectively), a finding similar to that of the INTERHEART study (CitationYusuf et al 2004). Among the three Asian populations, Chinese, Malay, and Indian, the highest age-standardized incidence rates in both sexes are in Indians. The first MI attack occurs in 4.4% of Asian women and 9.7% of men at age less than 40 years, which is 2- to 3.5-fold higher than in the West European population and is third highest of all the regions studied worldwide (CitationYusuf et al 2004). These studies carried out in India and other places suggest that Asians in general and Indians in particular are at increased risk of MI at a younger age (<40 years), irrespective of whether they have migrated to other countries or are resident Asians.
It must be emphasized that although the median age of presentation is higher in women, they are known worldwide to have poor prognosis compared with men (CitationMosca et al 1997; CitationMarrugat et al 1998; CitationMarrugat et al 2001; CitationVaccarino et al 2001; CitationKam et al 2002; CitationMak et al 2004). Younger Asian women have worse survival at 28 days after acute MI (CitationJenkins et al 1994; CitationKam et al 2002). The reasons for higher mortality in younger women are poorly understood and may be related to the presence of different risk factors in women, comorbidities, severity of infarction, and response to treatment. In view of the above discussion, it is imperative to ascertain the causes of the rising prevalence and emergence of CAD earlier in the life of Indians.
Risk factors for premature CAD in Indians
Most of the knowledge on CAD risk factors in different age groups is from studies carried out in the migrant Indian population (CitationDavidson et al 1991; CitationEnas et al 1991; CitationJha et al 1993; CitationBhalodkar et al 2004; CitationLiao et al 2004), and these have their limitations. It has been suggested that the results of these studies cannot be generalized, as there is either overrepresentation of certain communities or under-representation or absence of other communities. Furthermore, Indians who have migrated to affluent countries are at a higher demographic transition state than those residing in India. For these reasons, it has been widely speculated that the observations in the migrant population may not hold true for the Indian population. Therefore, we review here only those studies that were carried out in resident Indians, as this provides the true status of the prevalence of conventional CAD risk factors in this population.
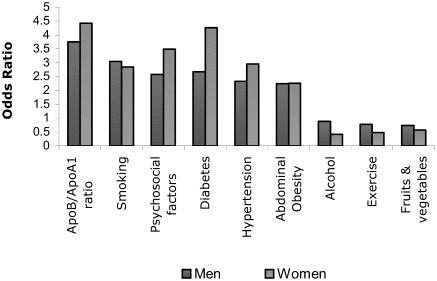
Recently, the INTERHEART study (CitationYusuf et al 2004), involving 52 countries, established an association between conventional modifiable risk factors for MI in all regions of the world, including South Asia, and in both sexes and at all ages ( and ). In South Asians, apolipoprotein (Apo)B/ApoA1 (odds ratio [OR] 3.81) and smoking (OR 2.43) were the important risk factors, as in the rest of the world. However, hypertension (OR 2.89), abdominal obesity (OR 2.43), and diabetes (OR 2.48) had more severe effects in South Asia, whereas psychosocial factors had an OR of 2.15, compared with 2.67 worldwide. The INTERHEART study also showed that hypertension and diabetes were more important risk factors in younger Indian women than men. Earlier studies, mostly in Western populations, have also found an association of the above-mentioned risk factors with the development of CAD. For example, in the Prospective Cardiovascular Münster Heart Study (PROCAM), a large prospective study in men aged 35–65 years, eight variables that made an independent contribution to risk of CAD were age, systolic blood pressure, LDL-C, HDL-C, triglycerides, diabetes mellitus, smoking, and family history of MI (CitationAssmann et al 2002).
Figure 3 Odds ratio for myocardial infarction risk factors worldwide; old (>53 years) versus young (<53 years). Data sourced from CitationYusuf et al 2004.
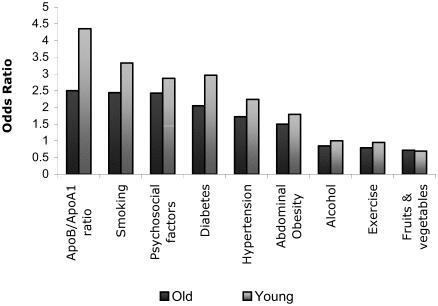
Figure 4 Odds ratio for myocardial infarction risk factors worldwide; men versus women. Data sourced from CitationYusuf et al 2004.
To find out if there are differences between the results obtained by the INTERHEART study and by the studies conducted independently in India, we reviewed the data obtained by the latter studies. The Jaipur Heart Watch-2 study is a prospective study from North India that found a high prevalence of classical risk factors for CAD, namely smoking, low physical activity, hypertension, hypercholesterolemia, diabetes, and obesity, in urban men and women of Jaipur (CitationGupta et al 2002). Factors peculiar to the South Asian population, such as truncal obesity, low HDL-C, and high triglycerides, were also prevalent. A significant increase in people with obesity, diabetes, and dyslipidemias was observed as compared with those reported in the Jaipur Heart Watch-1 study carried out in the early 1990s in the same population. An increasing prevalence of impaired glucose tolerance and diabetes in urban residents of Chennai has also been reported (CitationRamachandran et al 2001).
Fewer studies on epidemiological data from angiographically proven cases of premature CAD (≤40 years) in native Indians are available (CitationKaul et al 1986; CitationMaity et al 1989; CitationDave et al 1991; CitationUsha et al 1991; CitationPinto et al 1992; CitationBiswas et al 1995; CitationMohan et al 2001; CitationGupta et al 2002; CitationGoel et al 2003). Hyperlipidemia was found to be prevalent in young Indians with CAD in these studies. However, differences appear to exist between the lipid levels present in North and South Indian CAD patients and individuals without CAD. It appears that North Indians manifest the disease at lower levels of total cholesterol (CitationMohan et al 2001; CitationRamachandran et al 2001; CitationGoel et al 2003). Also, a greater role can be attributed to total cholesterol and LDL-C in atherogenesis in the younger Indian population (≤40 years) with angiographically proven CAD. The lower HDL-C and higher triglyceride levels in both younger and older cases appear to be a hallmark of the Indian population (CitationMohan et al 2001; CitationGoel et al 2003). In the INTERHEART study (CitationYusuf et al 2004) also, the highest population attributable risk (PAR) was abnormal lipids (ApoB/ApoA1 ratio) in both sexes. These studies indicate that abnormalities in lipid metabolism play an important role in development of CAD in young Indians. Also, compared with women (CitationDave et al 1991; CitationPinto et al 1992), young Indian male patients have a slightly lower prevalence of hypertension and diabetes (CitationKaul et al 1986; CitationMaity et al 1989; CitationGoel et al 2003).
Smoking and low physical activity in Indians have been found to be prevalent in 20–39-year-old urban adults (CitationGupta et al 2002). The INTERHEART study also observed that smoking was a greater risk factor in younger men than in women (CitationYusuf et al 2004). The risk of CAD increased incrementally with smoking. The OR was 9.16 in individuals who smoked more than 40 cigarettes per day, compared with 1.38 in those smoking 1–5 cigarettes per day, indicating that there is no safe limit for smoking. Other epidemiological studies from India also suggest a greater association of smoking with CAD in younger individuals (CitationKaul et al 1986; CitationSewdarsen 1987; CitationMaity et al 1989; CitationUsha et al 1991; CitationGoel et al 2003). Furthermore, the prevalence of smoking in South Indian males (44.6%) and passive smoking in South Indian females (45.3%) has been reported to be significantly higher than in North Indians (CitationBegom and Singh 1995). Interestingly, smoking has not been found to be a significant risk factor in acute MI patients from rural parts of India. The patients from rural India, however, have elevated blood glucose and abnormal waist/hip ratio (CitationPatil et al 2004).
Another important independent risk factor for CAD in younger cases emerging out of Indian studies is family history of CAD (CitationKaul et al 1986; CitationMaity et al 1989; CitationGoel et al 2003). The INTERHEART study showed a PAR of 14.8% in younger versus 10.45% in older patients (CitationYusuf et al 2004). Though addition of family history of CAD to other risk factors causes only a modest increase in PAR by 1% (CitationYusuf et al 2004), it must be emphasized that modifiable physiological variables such as blood pressure, ApoB/ApoA1 ratio, serum cholesterol, and abdominal obesity are also partially under genetic control. As family history of CAD emerged as the second most important risk factor in young Indian patients (CitationGoel et al 2003), analysis of potential genetic factors such as variance of genes involved in vascular homeostasis, hemostatic factors, lipid metabolism, and other metabolic factors is warranted.
Evidence from studies carried out in South Asians (CitationYusuf et al 2004) suggests that conventional risk factors account for 90% of the PAR in men and 94% in women (hypertension, smoking, diabetes, ApoB/ApoA1 ratio, and abdominal obesity accounted for 80.2% of the PAR). As these risk factors were also established by Indian studies to be involved in premature CAD, there are now enough data for establishment of health policies to counteract the threat posed by the epidemic of CVDs in India. Modification of environmental triggers for these risk factors is likely to reduce the speed of this advancing epidemic. The benefits of genetic research in this area can in future be reaped in economic terms.
What needs to be done?
In view of the above discussion, we propose an action plan to tackle CAD in India, salient features of which are given in .
Table 2 Action plan to tackle coronary artery disease (CAD) in India
Defining the cut-offs for CAD risk factors
A cause of concern to developing countries such as India is the incomplete detection, treatment, and control of CAD risk factors. The non-availability of guidelines for various risk factors such as cholesterol, triglycerides, HDL-C, and systolic and diastolic blood pressure with particular reference to Indians hampers treatment. In the absence of population-specific upper and lower extreme values for a risk factor, a clinician is left with an “action level” for a risk factor that is perhaps more appropriate for Western populations. The result is that treatment at lower levels of the risk factor is denied. According to the available data in native Indians, it is likely that some of the cut-offs for parameters such as total cholesterol, triglycerides, LDL-C, HDL-C, blood pressure, and body mass index (BMI) are different from those in Western populations. The lower BMI (<23) cut-off value for Asians is one such example (CitationSnehalatha et al 2003; CitationPan et al 2004).
The benefit of treating patients with myocardial ischemia and cholesterol levels within normal limits have been shown by several studies (CitationOng 2002), including the Cholesterol and Recurrent Events (CARE) study, the Long-term Intervention with Pravastatin in Ischemic Disease (LIPID) study, and the Heart Protection Study (HPS). The beneficial effects of statins in bringing down mortality rates due to CAD can be obtained only if appropriate guidelines for a population are available. The occurrence of CAD in North Indians (CitationGoel et al 2003) at lower cholesterol levels (∼170 mg/dL) indicates the need for lowering the upper safe limits for this parameter.
Once the guidelines for cut-off values for Asians for different risk factors at different ages and BMI for the two sexes are available, a true picture of the prevalence of these risk factors in this population will be available. Appropriate guidelines for identifying an individual at risk of developing CAD could then be established. Beneficial effects of therapies for reducing risk factors in the Indian population can subsequently be achieved.
Thus the key to finding a solution to the CAD epidemic in Asians in general and Indians in particular lies in getting accurate data for CAD risk factors in native populations using guideline values relevant to these populations.
Preventing the unhealthy demographic transition
Empowering the community to determine what works best for them may make a difference as far as CAD prevention is concerned.
Wider debate on complex issues like use of “polypills” for prevention of CAD in the asymptomatic population is needed.
It is well known that controlling the risk factors in patients with CAD risk equivalents is effective in reducing the rates of CAD. The benefits of addressing the root cause of CVD, such as smoking, threatening levels of body fat, cholesterol, and blood pressure, and low intake of fruits and vegetables, together with the use of affordable and accessible preventive combination medications will be immense in a country the size of India in terms of number of lives saved, mostly among middle-aged persons. The barriers to bringing about community and individual behavior changes also need to be addressed. These findings may then be translated into innovative preventive approaches targeting both the community and individuals to help reduce the risk of CAD. Simple solutions to seemingly complex problems may be available within the community. For example, low intake of fruits and vegetables may be related to low availability and affordability, which may be solved by regular or weekly neighborhood markets where farmers can sell their fresh produce themselves at a reasonable price; religious groups can help in promoting exercise, abstinence from smoking, and observance of a vegetarian diet; healthier ways of cooking traditional food can be demonstrated by local television stations, etc. Empowering the community to determine what works best for them may make a difference as far as CAD prevention is concerned.
Recently, CitationWald and Law (2003) proposed a strategy for simultaneously reducing four CVD risk factors (LDL-C, homocysteine, blood pressure, and platelet function) by providing a single pill containing aspirin, a statin, three blood pressure-lowering agents in half dose, and folic acid to people with vascular disease and those aged over 55 years. However, the complex issues of use of preventive medication among people without symptomatic disease require wider public debate.
Women: neglected victims of heart disease
Because coronary heart disease-related mortality is less in younger women than in men, it is widely believed that CAD is a men's disease. In fact, CAD is the leading cause of death in many parts of the world even in women younger than 65 years. summarizes the main points regarding heart disease in Indian women. In India, diseases of the circulatory system were among the top three causes of death in rural women in 1994 (CitationGopalan and Shiva 1999; CitationRamanakumar 2004). One of the leading causes of morbidity in urban Indian women in 1993 was high blood pressure and heart ailments (CitationRamanakumar 2004). As the prognosis in women is worse than that in men, these facts underline the need for giving special attention to women and heart disease.
Table 3 Heart disease in Indian women
Informing women about their risk factors will help them to respond in a better way to preventive health advice and will enable them to recognize symptoms themselves. Health professionals, on the other hand, need to improve diagnosis, referral, and treatment of women with symptoms of CAD.
Access to medicines
Advances in medicine and technology have provided a boost to health and life expectancy. However, the benefits of these advances have not infiltrated to the poorer developing countries. There is an urgent need to improve access to key medicines in countries such as India. Barriers exist in the form of lack of money to buy medicines, improper selection of drugs, poor health infrastructure, and lack of political will of governments. New regulations need to be drafted and adopted to enable essential medicines at reduced prices to reach the poorer sections of society.
Conclusions
Researchers worldwide consider there is a 20-year window of opportunity to make inroads against the ravages of CVD. To slow the momentum of CVD in countries such as India, particularly among the working-age population, major initiatives are needed to combat CVD, whether promotion of diet and physical activity, generation of awareness among both sexes, or development of guidelines for risk factors and therapeutic and surgical strategies.
References
- AssmannGCullenPSchulteHSimple scoring scheme for calculating the risk of acute coronary events based on the 10-year follow-up of the Prospective Cardiovascular Munster (PROCAM) studyCirculation20021053101511804985
- BegomRSinghRBPrevalence of coronary artery disease and its risk factors in the urban population of South and North IndiaActa Cardiol199550227407676762
- BhalodkarNCBlumSRanaTComparison of levels of large and small high-density lipoprotein cholesterol in Asian Indian men compared with Caucasian men in the Framingham Offspring StudyAm J Cardiol2004941561315589018
- BiswasPKDasbiswasARoySRisk factors and angiographic profile of coronary artery disease in youngJ Indian Med Assoc199593902948522821
- BulataoRAStephensPWGlobal estimates and projections of mortality by cause, 1970-2015. Preworking paper 10071992WashingtonPopulation Health and Nutrition Department, World Bank
- ChadhaSLGopinathNShekhawatSUrban-rural differences in the prevalence of coronary heart disease and its risk factors in DelhiBull World Health Organ1997753189141748
- DaveTHWasirHSPrabhakaranDProfile of coronary artery disease in Indian women: correlation of clinical, non-invasive and coronary angiographic findingsIndian Heart J1991432591894297
- DavidsonMEEnasEAThomasIHigh prevalence of low HDL-C levels and other dyslipidemic disorders in Asian Indians in the United States1991Proceedings of the National Conference on Cholesterol and High Blood Pressure ControlWashington
- DewanBDMalhotraKGuptaSEpidemiological study of coronary heart disease in a rural community in HaryanaIndian Heart J19742668784419665
- EnasEADavidsonMENairVPrevalence of coronary heart disease (CHD) and its risk factors in Asian Indian migrants to the United States19919th International Symposium on AtherosclerosisRosemont, ILInternational Atherosclerosis Society267
- EnasEADhawanJPetkarSCoronary artery disease in Asian Indians: lessons learnt and the role of lipoprotein-aIndian Heart J19964925349130422
- EnasEAGargADavidsonMACoronary heart disease and its risk factors in the first generation immigrant Asian Indians to the United States of AmericaIndian Heart J199648343548908818
- EnasEASenthilkumarACoronary artery disease in Asian Indians: an update and review [online]Internet J Cardiol20011 Accessed 15 Feb 2005. URL: http://www.ispub.com/ostia/index.php?xmlFilePath=journals/ijc/vol1n2/cadi.xml
- EnasEAYusufSThird Meeting of the International Working Group on Coronary Artery Disease in South AsiansIndian Heart J1999519910310327791
- GhaffarAReddyKSSinghiMBurden of non-communicable diseases in South AsiaBMJ20043288071015070638
- GoelPKBhartiBBPandeyCMA tertiary care hospital-based study of conventional risk factors including lipid profile in proven coronary artery diseaseIndian Heart J2003552344014560932
- GopalanSShivaMNational profile on women, health and development: India1999New DelhiVoluntary Health Association of India
- GowarikarVIndia has done it: demographic transition already underway in IndiaIIPS Newsl1995362812291348
- GuptaREpidemiological evolution and rise of coronary heart disease in IndiaSouth Asian J Prev Cardiol199711420
- GuptaRGuptaHPKeswaniPCoronary heart disease and coronary risk factor prevalence in rural RajasthanJ Assoc Physicians India1994422467836242
- GuptaRGuptaVPMeta-analysis of coronary heart disease prevalence in IndiaIndian Heart J19964824158755007
- GuptaRGuptaVPAhluwaliaNSEducational status, coronary heart disease and coronary risk factor prevalence in a rural population in IndiaBMJ1994307133267866081
- GuptaRGuptaVPSarnaMPrevalence of coronary heart disease and risk factors in an urban Indian population: Jaipur Heart Watch-2Indian Heart J200254596611999090
- GuptaRPrakashHMajumdarSPrevalence of coronary heart disease and coronary risk factors in an urban population of RajasthanIndian Heart J19954733188557274
- GuptaSPMalhotraKCUrban–rural trends in epidemiology of coronary heart diseaseJ Assoc Physicians India197523885921225892
- HarrisRBWeissfieldLAGender differences in the reliability of reporting symptoms of angina pectorisJ Clin Epidemiol199144107181941000
- HughesLORavalURafteryEBFirst myocardial infarctions in Asian and white menBMJ19892981345502502249
- India–Human Development Fact Sheet Accessed 23 Jun 2005. URL: http://hdrc.undp.org.in/APRI/hds/hdfct/India.htm
- JenkinsJSFlakerGCNolteBCauses of higher in-hospital mortality in women than in men after acute myocardial infarction: the Framingham studyAm J Cardiol199473319228109543
- JhaPEnasEAYusufSCoronary artery disease in Asian Indians: prevalence and risk factorsAsian Am Pacific Islander J Health1993116375
- KamRCutterJChewSKGender differences in outcome after an acute myocardial infarctionSingapore Med J200243243812188076
- KaulUDograBManchandaSCMyocardial infarction in young Indian patients: risk factors and coronary arteriographic profileAm Heart J19861127153728290
- KuttyRVBalakrishnanKJayasreeAPrevalence of coronary heart disease in the rural population of Thiruvananthapuram district, Kerala, IndiaInt J Cardiol19933959708407009
- LangTShettyPSMcPhersonKThe public health impact of globalization of food tradeDiet, nutrition and chronic disease: lessons from contrasting worlds1997Chichester, UKWiley17387
- LiaoYTuckerPGilesWHHealth status among REACH 2010 Communities, 2001-2002Ethn Dis200414S1-9S1-13
- MackayJMensahGThe atlas of heart disease and stroke2004World Health Organization, Centers for Disease Control and Prevention
- MaityAKDasMKChatterjeeSSPrognostic significance of risk factors in acute myocardial infarction in youngIndian Heart J198941288912599536
- MakKHKarkJDChiaKSEthnic variations in female vulnerability after an acute coronary eventHeart200490621615145860
- MammiMVIPavithranPRahmanPAAcute MI in North Kerala. A 20-year hospital based studyIndian Heart J1991439361752622
- MarrugatJGilMMasiáRMortality differences between men and women following first myocardial infarction. RESCATE InvestigatorsJAMA1998280140599800999
- MarrugatJGilMMasiaRRole of age and sex in short-term and long-term mortality after a first Q wave myocardial infarctionJ Epidemiol Commun Health20015548793
- MathurKSEnvironmental factors in coronary heart disease. An epidemiological study at Agra (India)Circulation1960216849
- MohanVDeepaRRaniSSPrevalence of coronary artery disease and its relationship to lipid in a selected population in South IndiaJ Am Coll Cardiol200138682711527617
- MoscaLMansonJESutherlandSECardiovascular disease in women: a statement for healthcare professionals from the American Heart AssociationCirculation1997962468829337227
- MurrayCJLLopezADGlobal comparative assessments in the health sector1994Geneva, SwitzerlandWorld Health Organization
- NegusBHWilliardJEGlamannDBCoronary anatomy and prognosis of young asymptomatic survivors of myocardial infarctionAm J Med19949635488166155
- OngHTProtecting the heart: a practical review of the statin studiesMed Gen Med2002441
- PadmavatiSEpidemiology of cardiovascular disease in India. II. Ischaemic heart diseaseCirculation1962257111714483097
- PaisPPogueJGersteinHRisk factors for acute myocardial infarction in Indians: a case-control studyLancet1996348358638709733
- PanWHFlegalKMChangHYBody mass index and obesityrelated metabolic disorders in Taiwanese and US whites and blacks: implications for definitions of overweight and obesity for AsiansAm J Clin Nutr20047931914684394
- PatilSSJoshiRGuptaGRisk factors for acute myocardial infarction in a rural population of central India: a hospital-based case-control studyNatl Med J India2004171899415372760
- PearsonTANew tools for coronary risk assessment. What are their advantages and limitations?Circulation20021058869211854132
- PintoRJBhagwatARLoyaYSCoronary artery disease in premenopausal Indian women: risk factors and angiographic profileIndian Heart J199244991011427940
- RamachandranASnehalathaCKapurAHigh prevalence of diabetes and impaired glucose tolerance in India: National Urban Diabetes SurveyDiabetologia200144109410111596662
- RamachandranASnehalathaCLathaEClustering of cardiovascular risk factors in urban Asian IndiansDiabetes Care199821967719614615
- RamachandranASnehalathaCVijayVLow risk threshold for acquired diabetogenic factors in Asian IndiansDiabetes Res Clin Pract2004651899515331198
- RamanakumarAVReviewing disease burden among rural Indian womenOnline J Health Allied Sci200421
- ReddyKSCardiovascular disease in IndiaWorld Health Stat Q19934610178303903
- ReddyKSSethiKKRising burden of cardiovascular disease in IndiaCoronary artery disease in Indians: a global perspective1998MumbaiCardiological Society of India6372
- ReddyKSYusufSEmerging epidemic of cardiovascular disease in developing countriesCirculation1998975966019494031
- SewdarsenMVythilingumSJialalIRisk factors in young Indian males with myocardial infarctionS Afr Med J19877126123824099
- SharmaSPXenosPAgeing in India: demographic background and analysis based on census materials. Occasional paper nr 2 of 19921992New DelhiOffice of the Registrar General and Census Commissioner
- SinghRBGhoshSNiazAMEpidemiological study of diet and coronary risk factors in relation to central obesity and insulin levels in rural and urban populations of north IndiaInt J Cardiol199547245557721501
- SnehalathaCViswanathanVRamachandranACutoff values for normal anthropometric variables in Asian Indian adultsDiabetes Care2003261380412716792
- UshaSShahCVSharmaSMyocardial infarction in the youngJ Assoc Physicians India19913952561800494
- VaccarinoVKrumholzHMYarzebskiJSex differences in 2-year mortality after hospital discharge for myocardial infarctionAnn Intern Med20011341738111177329
- WaldNJLawMRA strategy to reduce cardiovascular disease by more than 80%BMJ2003326141912829553
- WanderGSKhuranaSBGulatiREpidemiology of coronary heart disease in a rural Punjab population – prevalence and correlation with various risk factorsIndian Heart J199446319237797219
- WasirJSMisraAThe metabolic syndrome in Asian Indians: impact of nutritional and socio-economic transition in IndiaMetab Syndr Relat Dis200421423
- [WHO] World Health OrganizationFacts and figures. The World Health report 2003–shaping the future [online]2003 Accessed 14 Feb 2005. URL: http://www.who.int/whr/2003/en/Facts_and_Figures-en.pdf
- World BankWorld development report: investing in health1993New York, NYOxford Univ Pr
- YusufSHawkenSÔunpuuSEffect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control studyLancet20043649375215364185