Abstract
Coronary bifurcations represent a challenging lesions subset and account for up to 15% of all current PCI. Regardless of the stenting technique used, however, restenosis rate after bare metal stent (BMS) is high, especially at the ostium of the side branch (SB). The introduction of drug-eluting stent (DES) has remarkably improved the outcome in bifurcation lesions compared to BMS, resulting in lower adverse events and main branch (MB) restenosis rates. Furthermore, although the “provisional” stenting technique (second stent on the SB placed, after the MB stenting, only in case of suboptimal or inadequate result) remained the prevailing approach, several two-stent techniques emerged (crush) or were re-introduced (V, T, culottes) to allow stenting in both branches when needed. At the present time, only few randomized studies and some observational reports specifically addressed the issue of bifurcation lesion treatment with sirolimus-eluting stents (SES). It is still not clear yet which is the better strategy between the provisional approach and stenting both branches when dealing with a bifurcation lesion which has a stenosis in the SB suitable for stenting. Moreover, no study has so far addressed which is the best strategy to use among the several techniques reported in the literature when both branches are intentionally stented from the outset. Finally, the introduction of dedicated stents for different types of bifurcations, with specific stent designs to provide good deliverability, secured access to the side branch, complete coverage of the lesion site without double/triple layers of stent struts, thus incorporating the benefits of drug elution and ensuring drug availability to all diseased surfaces, may further facilitate the conquest of one of the most challenging areas in interventional cardiology.
Introduction
Following the introduction of drug eluting stents (DES), there has been a major shift in the management of complex lesions from surgery to percutaneous coronary intervention (PCI). (CitationColombo and Iakovou 2004a, Citation2004b; CitationKastrati et al 2004) Coronary bifurcations account for up to 15% of all current PCI (CitationMelikian et al 2004) and still represent a challenging lesion subset for the interventional cardiologist. In the stent era, despite improved and more predictable acute angiographic results and procedural outcomes, (CitationAliabadi et al 1997; CitationAl Suwaidi et al 2000; CitationSheiban et al 2000) bifurcation treatment was still associated with lower procedural success and higher in-hospital major adverse cardiac event (MACE) and restenosis rate, when compared with non bifurcation interventions (Lefevre et al 2000; CitationAl Suwaidi et al 2001). Several stenting techniques have been proposed for the treatment of bifurcations (CitationColombo et al 1993; CitationSchampaert et al 1996; CitationChevalier et al 1998; CitationKobayashi et al 1998; CitationYamashita et al 2000; Lefevre et al 2001; CitationPan et al 2002). However, regardless of the technique used, the restenosis rate after bare metal stent (BMS) implantation was high (40% to 60%), especially at the ostium of the side branch (SB) (CitationAl Suwaidi et al 2000; CitationYamashita et al 2000; CitationCervinka et al 2002; CitationGobeil et al 2002). Moreover, regardless of a superior immediate angiographic result, BMS implantation in both branches offered no additional advantage over main branch (MB) stenting alone, in terms of restenosis and re-intervention, and was associated with an increase in the occurrence of in-hospital MACE (13% vs 0% in the study by Yamashita et al) (CitationAl Suwaidi et al 2000; CitationSheiban et al 2000; CitationYamashita et al 2000; CitationCervinka et al 2002; CitationGobeil et al 2002).
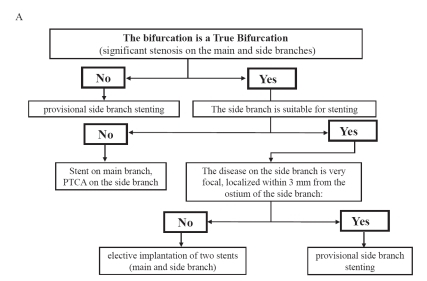
The introduction of DES has markedly improved the outcome in bifurcation lesions as compared to BMS, resulting in lower adverse events and restenosis rates (CitationColombo et al 2004; CitationPan et al 2004; CitationGe et al 2005b; CitationTanabe et al 2004). Furthermore, although the “provisional” stenting technique (second stent on the SB placed after the MB stenting, only in case of suboptimal result or complication in side branch) remained the prevailing approach, several two-stent techniques emerged (crush) or were re-introduced (V, T, culottes) (CitationIakovou et al 2005a). In our experience () the provisional stent approach is in general the preferred one when the SB diameter is less than 2.25 mm and it is not diffusely diseased (CitationIakovou et al 2005a). Conversely, stenting of both branches as intention-to-treat, is preferred in true bifurcations with a diffusely diseased SB ≥2.25 mm in diameter.
Figure 1 Current practise in the treatment of bifurcation lesions in our Center.
Sirolimus-eluting stent in the treatment of bifurcation lesions
At the present time, only few randomized studies and some observational reports specifically addressed the issue of bifurcation lesion treatment with sirolimus-eluting stents (SES).
Randomized studies evaluating SES in bifurcation lesions
The safety and efficacy of SES for the treatment of de novo true bifurcation lesions has been evaluated in three randomized studies. All compared the systematic use of two stents versus a provisional side-branch stenting strategy.
In the first prospective multicenter study, (CitationColombo et al 2004) 85 patients with 86 bifurcation lesions were randomly assigned to Cypher (Cordis Corp, a Johnson & Johnson Company, Warren, New Jersey) stent implantation either in both branches as intention to treat (group A) or in the MB only, with provisional SB stenting (group B). Twenty-two patients crossed over from group B to group A (51.2%) due to suboptimal result after balloon dilatation of the SB, and 2 patients crossed over from group A to group B (4.7%) due to lack of successful stent delivery in the SB. Analysis was performed according to the actual treatment received (not by intention-to-treat) and because of the high crossover rate more lesions were treated with stenting of both branches (n = 63) than with MB stent/SB balloon (n = 22). One patient died suddenly 4.5 months after the procedure; three (3.5%) had stent thrombosis (in 2 cases involving the SB and both branches in the other). All patients with stent thrombosis, as well as the patient that died suddenly, had undergone stenting of both branches. The total 6-month in-segment restenosis rate per lesion (either SB or MB or both) was 25.7%, not significantly different between groups A (28.0%) and B (18.7%). Most restenoses were focal and occurred at the SB ostium. Target lesion revascularization (TLR) was performed in 7 cases overall. Three of the 4 intravascular ultrasound (IVUS) examinations performed at follow-up among the 11 cases of SB in-stent restenosis demonstrated incomplete ostium coverage by the stent struts.
The main findings of this study were: 1) the remarkably lower restenosis rate in the MB with the use of Cypher™ stent (6.1%) as compared with historical BMS controls; 2) the frequent residual stenosis at the SB ostium after balloon angioplasty, leading to a high rate (51.2%) of cross over to additional SB stenting; 3) the absence of a clear superiority of systematic SB stenting as compared to MB stenting only; 4) the relatively high angiographic restenosis rates occurring at SB (mostly located at the ostium) when an additional Cypher stent was implanted there, and, conversely, the low TLR rate (7 of 17 cases), probably reflecting a limited clinical importance of many cases of angiographic SB restenosis; 5) the 3.5% stent thrombosis rate, higher than previously experienced with Cypher stent in less complex lesions. Because of the high crossover rate in this study, no conclusions could be drawn regarding the most appropriate bifurcation stenting technique. However, the study highlighted the persistent limitations of routine SB stenting that although results are improved compared with historical BMS data; SB restenosis albeit focal continues to remain a problem.
In the study by Pan et al (CitationPan et al 2004) 91 patients with true bifurcation lesions, all receiving a SES in the MB, were randomly assigned to either balloon dilation of the involved SB (group A; n = 47) or a second stent in the SB (group B; n = 44). Crossover was allowed only in patients with severe persistent stenosis and/or major flow-limiting dissections; local dissections with TIMI 3 flow were left without additional treatment. According to this predefined criteria for additional stenting, crossover rates were relatively low: only 1 patient from group A to SB stenting and 4 patients from group B to A. Primary success was obtained in 44 patients of group A (94%) and 43 of group B (97%). At 6 month follow-up, MACE occurred in 3 patients in group A: 2 had in-hospital non-Q–wave myocardial infarction (MI) and 1 TLR and in 3 patients in group B: 1 experienced a 15 day post-procedure sub-acute stent thrombosis, followed by MI and eventual death, and 2 TLR. Six-month angiographic follow-up was performed in 80 (88%) patients. MB restenosis occurred in 1 (2%) patient in group A and 4 (10%) in group B; SB restenosis occurred in 2 (5%) patients in group A and 6 (15%) in group B. Therefore, similar to the Sirius bifurcation study,(CitationColombo et al 2004) stenting both branches seemed to provide no advantage over a provisional strategy and once again was associated with a higher SB restenosis rate.
Steigen et al (CitationSteigen et al 2006) recently published the results of the Nordic Bifurcation Study which included 413 patients with a bifurcation lesion randomized to stenting of both branches (n = 206), with “crush”, “culottes”, “Y” or other techniques, or provisional SB stenting (n = 207) with SES implantation. The crossover from provisional to double branch stenting was allowed only if following SB dilation TIMI flow was 0. However, SB dilation was only performed if TIMI <3 flow in the SB. Procedural success was achieved in 97% of cases in the provisional and 95% in the both branches stenting group. The SB was stented only in 4.3% of cases in the provisional stenting group. Final kissing balloon inflation (FKB) was performed in 32% of the cases in the provisional group and 74% of double stenting group (p < 0.001). At 6 months, no statistical difference between the two groups was found in the primary end-point of MACE (2.9% in the MV group and 3.4% in the MV + SB group). No differences were also detected in any of the primary end-point components (death, MI, TVR, or stent thrombosis). Procedure-related biomarker release could be evaluated in 279 patients (126 patients in the MV + SB group and 153 in the MV group). Marker elevation of >3 times the upper limit of normal was seen in 18% of MV + SB and in 8% of MV group (p = 0.011). At randomization, only 358 out of 413 patients enrolled in this trial, were scheduled for 8-month follow-up angiography. Complete angiographic evaluation was available, indeed, in 307 patients (86%) of these, 151 patients were randomized to the MV group and 156 to the MV + SB group. The combined angiographic end point of diameter stenosis >50% of main vessel and/or occlusion of the side branch after 8 months was found in 8 patients (5.3%) in the MV group and 8 patients (5.1%) in the MV + SB group (p = 0.96). The main limitation of this study was the lack of systematic angiographic follow-up (only 76% of the total number of patients randomized did angiographic follow-up). It is well known that most restenoses occurring at the SB ostium are clinically silent and thus not detected, unless identified at follow-up angiography. The effective clinical value of these silent restenosis is currently unknown.
Observational studies
Ge et al (CitationGe et al 2005b) evaluated the one vs. two stent approach in 174 consecutive patients with bifurcation lesions, treated with a SB provisional (group 1S; 57 patients with 58 bifurcation lesions) or both branches (group 2S; 117 patients with 126 bifurcation lesions) SES implantation strategy. In-hospital MACE were respectively 8.8% in the 1S and 10.3% in the 2S group (p = 0.97). At 9 months, no significant differences in terms of MB and SB restenosis, TLR (5.4% vs 8.9%, p = 0.76), target vessel revascularization (TVR, 5.4% vs 11.1%, p = 0.51) or cumulative MACE (18.9% vs 23.3%, p = 0.76) were found between the 2 groups. Confirming previous data, this study showed a high procedural success irrespective of the technique used, with marked improvement compared to historical controls with BMS.
At that time, the T- and modified T-stenting techniques were used as the default two-stent strategies. However, an important limitation of these approaches is represented by the inability to guarantee full SB ostium coverage, especially in cases with a narrow bifurcation angle. There is almost always a small gap left between the MB and the SB stents, as shown in 2/3 of the SB restenosis cases examined by IVUS in the sirolimus bifurcation study (CitationColombo et al 2004). Furthermore, when DES are implanted, incomplete SB ostium coverage with consequent lack of drug delivery could be a factor contributing to the occurrence of restenosis at this site.
Crush technique
The need for a 2-stent technique to overcome the limitations of T-stenting and guarantee full SB ostium coverage prompted our group to develop the “crush” technique. This strategy reproduces the same steps of the modified-T stenting, with the main difference being a slight (3–4 mm) protrusion of the proximal edge of the SB stent into the MB (CitationIakovou et al 2005a). The SB stent is then flattened against the MB stent. Our initial experience with the crush technique involved 20 patients with true bifurcation lesions treated with SES implantation (CitationColombo et al 2003) (CitationAiroldi et al 2003). In order to correct stent deformation and improve strut contact to the vessel wall, and thus better drug delivery to the SB ostium, (CitationOrmiston et al 2004) FKB was implemented as part of the crush technique, which was not routinely performed in our preliminary experience. FKB, which was not routinely performed in our preliminary experience, was implemented as part of the crush technique in order to correct stent deformation, improve strut contact to the vessel wall, and thus better drug delivery to the SB ostium.
Ge et al (CitationGe et al 2005a) evaluated the long-term outcome after SES or paclitaxel-eluting stent (PES) implantation in true bifurcations treated with the “crush” technique performed with or without FKB, according to operator’s discretion. SB restenosis and late lumen loss were significantly lower in lesions treated with FKB, as compared to those without (11.1% vs 37.9%, p < 0.001). The cumulative MACE rate was also lower in the FKB group (19.8% vs 38.5%, p = 0.008). The absence of FKB was identified as an independent predictor (HR 4.17, p = 0.02) of TLR. In this study, the “crush” stenting technique with FKB was associated with more favourable long-term outcomes, with a striking 49% reduction in SB restenosis rates as compared to the SES bifurcation study, (CitationColombo 2004) probably due to better strut coverage of and drug delivery to the vessel wall. Furthermore, whenever restenosis occurred, it was focal (<5 mm in length), located at the SB ostium (75.0%), and majority of the time was not associated with symptoms or ischemia. These results demonstrated that FKB is a mandatory step of the “crush” technique.
An important technical aspect that we recommend regarding the final dilation is the performance of a high-pressure SB inflation before the final kissing balloon inflation. This 2-step final kissing inflation results in improved opening of and less obstruction by stent struts at the side branch ostium.
Moussa et al (CitationMoussa 2006) reported in a prospective registry on the outcome of 120 patients with de novo or in-BMS restenotic bifurcation lesions, treated with SES using the “crush” technique. FKB was performed in 87.5% of cases. Procedural as well as device success was achieved in 97.5% (3 patients received a BMS in the SB because of SES inability to cross the lesion). No in-hospital MACE was reported. At 30 days, stent thrombosis occurred in 2 patients (1.7%), one was treated with repeat PCI and the other was referred for coronary artery bypass graft (CABG) surgery. At 6 months, no cardiac death, MI or stent thromboses were reported. TLR was required in 13 patients (11.3%): 10 (8.7%) underwent rePCI and 3 (2.6%) were referred to CABG. Restenosis was focal in all cases involving the MB only in 3 patients (23%), the SB ostium and the MB in 1 patient (8%), and limited to the SB ostium in 9 patients (69%). These findings confirmed that, when appropriately performed, the crush technique is safe and associated with a low incidence of early or late thrombosis. However, even if reduced following routine FKB, restenosis is still present, especially at the SB ostium.
Possible explanations of SB ostial restenosis might be the breakage of the polymer secondary to the overlap of multiple struts layers, stent deformation or stent under expansion.(CitationOrmiston et al 2004) IVUS studies have shown that stent dimensions are important predictors of restenosis even with DES (CitationSonoda et al 2004) and that imaging of both branches could reveal inadequate stent expansion in at least one branch even after kissing balloon inflation and regardless of the angiographic result (CitationTakebayashi et al 2003).
Costa et al (CitationCosta et al 2005) reported IVUS findings in 40 patients with bifurcation lesions treated with “crush” technique and SES. Post-intervention IVUS was performed in both branches in 25 lesions and only in the MB in 15 lesions. IVUS measurements were performed in the proximal stent, crush area and distal stent in the MB as well as in the ostium and distal stent in the SB. Overall; minimum stent area (MSA) was larger in the MB as compared to the SB (6.7 ± 1.7 mm2 vs 4.4 ± 1.4 mm2, p < 0.0001, respectively). When only the MB was considered, the MSA was smaller in the crush area (rather than in the proximal or distal stent segments) in 56% of the lesions. However, when both the MB and the SB were considered, the smallest MSA was calculated in the SB ostium in 68% of cases. In the lesions not involving the left main coronary artery (LMCA), stent expansion was significantly lower in the SB as compared to the MB (p = 0.02). The MB MSA measured <4 mm2 in 8% of lesions and <5 mm2 in 20%. For the SB, a MSA <4 mm2 was found in 44%, and a MSA <5 mm2 in 76%, typically at the ostium. “Incomplete crushing” (defined as incomplete apposition of SB or MB stent struts against the MB wall proximal to the carina) was observed in >60% of angiographically successful non-LMCA lesions and it was correlated with SB stent underexpansion (77.1 ± 7.6% vs 89.4 ± 13.1%, p = 0.04). The only patient with subacute stent thrombosis had incomplete crushing. Despite the wide (80% of cases) use of SB ostial predilation and FKB (performed in all but 2 cases), stent underexpansion and incomplete strut apposition in the “crush area” were detected by IVUS. The location of the smallest MSA at the SB ostium could explain the higher restenosis rate at this site. The results of this study emphasize the value of performing a full and complete high pressure post-dilation of the SB stent.
Different stenting techniques
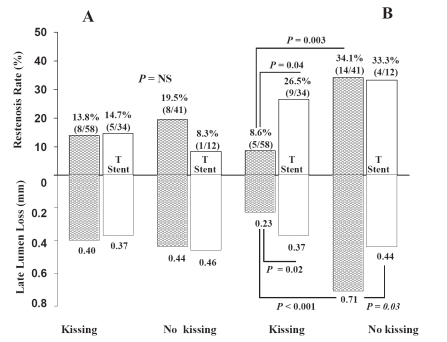
Tanabe et al (CitationTanabe et al 2004) reported on the outcome of a small series of 58 patients with 65 de novo bifurcations, part of the “Rapamycin-Eluting Stent Evaluation At Rotterdam Cardiology Hospital” (RESEARCH) registry, (CitationLemos et al 2004) treated with SES in both the main and the side branches with one of the following techniques: T (63%), culottes (8%), kissing stents (3%), or “crush” (26%). Kissing balloon inflation was performed in only 31% of cases. At 6 months, MACE occurred in 10.3% of cases, with a TLR rate of 8.6%, and no episodes of MI or stent thrombosis. Angiographic 6-month follow-up was performed in 44 lesions: restenosis occurred in 10 of them (22.7%), and in particular in 4 lesions in the MB (9.1%) and in 6 in the SB (13.6%). The restenosis rate for the SB was 16.7% following T-stenting vs 7.1% with all the other stent techniques. Once again after the use of the T-stenting technique SB restenosis were mostly located at the ostium (5 of the 6 cases of SB restenosis). In a report by our group, (CitationGe et al 2006) the “crush” technique with FKB was associated with a significant reduction of SB restenosis rate (8.6% vs 26.5%, p = 0.04) when compared to the T stenting technique ().
Figure 2 Restenosis rates and late lumen loss at 6 month angiographic follow-up following double stenting with the “crush” (black bars) vs T stenting (white bars) techniques with and without kissing balloon post-dilatation in the main branch (Panel A) and in the side branch (Panel B). Values are expressed as number (%) or mean (SD). NS, not statistical significant 8 (adapted from Lee et al Heart 2006; 92(3): 371–376)
No major advantage of the “V” over the “Crush” technique was observed in the study by Sawhney et al. (CitationSawhney et al 2005) One hundred-fifty three consecutive patients were treated with SES implantation in true bifurcation lesions: 102 with “crush” (43 with and 59 without FKB) and 51 with the “V” technique. Procedural success was achieved in 100% of cases; 18 patients (12%) had an in-hospital MI, whereas no death, acute thrombosis or urgent TLR was reported. At 5 month follow-up the overall TLR rate was 13.1%. The restenosis rate was 13.7% in patients treated with “V” stenting, 16.9% in the crush group without FKB, and 7.0% in the crush group with FKB. Of the 13 TLR that occurred in the crush group, most were located at the SB. In the V group 7 TLRs occurred, 3 located in one branch and 4 in both branches. Three patients (1.9%) experienced subacute thrombosis at follow-up and the 9-month cumulative incidence of death, MI, TVR or thrombosis was 18%. Bifurcation stenting with SES using the “crush” or “V” technique was associated with very low procedural complications and acceptably low clinical restenosis rates at 5 months.
Sharma et al evaluated 200 patients who underwent SES implantation in 202 true de novo bifurcation lesions with the “simultaneous kissing stent” (SKS) technique (CitationSharma 2005). This technique involves implanting a stent simultaneously in the MB and SB, which overlap in the proximal segment of the MB, thus creating proximally a new carina. The SKS differs from the V-technique which has a very short or no carina. Procedural success was achieved in 100% of the MB and 99% of the SB. In-hospital and 30-day MACE were 3% and 5%, respectively. At a mean clinical follow-up of 9 ± 2 months, MI incidence was 4% and death rate was 2%. The TLR incidence was 4%: 6 cases occurred in the SB (3%) and 2 in both SB and MB (1%). The isolated SB in-stent restenosis were focal, while restenosis involving both SB and MB were diffuse. There were two cases (1%) of subacute stent thrombosis at day 5 and day 8 but no late stent thrombosis was reported.
Jim et al (CitationJim et al 2006)described the “sleeve technique”. This technique requires a double kissing balloon inflation, before and after MB stenting. The sleeve technique was used in 6 consecutive patients with 100% success rate and no MACE or stent thrombosis within 30 days.
Recently a new technique “T And small Protrusion” (TAP technique) has been proposed by our group. This technique has been used only in 10 cases without adverse cardiac events at 30 days; no data at long term are available so far. The TAP technique is mainly used when the operator decides to cross-over from 1 to 2 stents and consist in the deployment of a stent on the SB with a balloon simultaneously inflated inside the MB stent. The stent in the SB will protrude minimally in the MD in order to allow good coverage of the ostium. Crush is prevented by keeping SB and MB balloons inflated simultaneously.
ARTS II substudy
The efficacy of SES in bifurcation treatment in patients with multivessel coronary artery disease was evaluated in a substudy (CitationTsuchida et al 2007) of the “Arterial Revascularisation Therapies Study Part II” (ARTS II Trial) (CitationSerruys et al 2005).
Compared to non-bifurcation lesions (n = 283), bifurcation lesions (n = 324) were associated with more complex procedural characteristics (number of stents implanted, number of stented lesions, average and total stent length, GP IIb/IIIa inhibitor use, longer procedure times, and post-procedural CK elevation), but they were not associated with higher adverse event rates at 30 days, as well as at 1 year (Major Adverse Cardiac and Cerebral Event, MACCE free survival at 1 year 90.1% vs 89.2%; p = 0.79). Even the occurrence of stent thrombosis did not differ between the bifurcation and the non-bifurcation groups (1.2% vs 0.4%; p = 0.38).
Of 465 bifurcation lesions, only 68 lesions (14.6 %) in 61 patients were treated with a 2-stent strategy. Despite longer procedure duration and complexity, no differences were found in 30-day, or 1-year clinical outcomes (1-year MACCE free 91.8% vs 88.6%; p = 0.65) in the 2 stent group compared with the 1 stent group.
Despite more complex procedural characteristics and a higher use of 2 stents, no difference in 30-day or 1-year clinical outcome were reported between patients with true (Duke modified Type D, F and G; n = 244 lesions) bifurcations vs. other bifurcation lesion types (n = 221) (CitationSianos et al 2005). Freedom from MACCEs at 1 year was 88.3% vs 90.2% respectively (p = 0.60).
SES vs PES
In a study by Pan et al (CitationPan et al 2007) 205 consecutive patients with true bifurcation lesions were randomized to SES (n = 103) or PES (n = 102) implantation. At 30 days 1 patient in the PES group and 2 in the SES group experienced a Q-wave MI, and no deaths were reported. At 6 months restenosis (9% vs 29%, p = 0.05) and TLR (4% vs 13 %, p = 0.05) rates were significantly lower in the SES, as compared to the PES group. In both groups restenosis occurred mostly at SB ostium.
Hoye et al (CitationHoye et al 2005) evaluated outcomes of 144 patients treated with SES in 167 de novo bifurcations and 104 patients treated with PES in 113 bifurcations. At 6 month follow-up, MACE-free survival was 93.7% in the SES vs 85.8% in the PES group (p = 0.05). TLR-free survival was 95.7% vs. 86.8% (p = 0.01). Predictors of MACE were age, diabetes, previous CABG, multivessel disease, treatment for acute MI, and treatment with PES. Stent type was the only independent predictor of TLR. Neither the baseline bifurcation anatomy, nor the stenting technique utilized, were predictive of MACE or TLR.
Unanswered questions
1) Optimal treatment strategy for bifurcation lesions
At the present time, the optimal strategy for bifurcation treatment is still unclear. Current studies are mostly retrospective, involving different bifurcation types (true and non-true bifurcations) and several stenting techniques making any comparison not appropriate. In addition, the classification of bifurcations used (CitationPopma et al 1994; CitationSpokojny and Sanborn 1996; Lefevre et al 2000; Safian 2001) suffer limitations of coronary angiography in detection of different plaque distribution and extent of disease and do not take into account what happens to the SB during the dilatation of the MB (CitationFujii et al 2003).
Our current practise in bifurcation lesions is illustrated in . In general, in non-true bifurcations a provisional stenting approach is suggested. In the presence of a true bifurcation with a SB larger than 2.25 mm and SB disease localized extending more than 3 mm from the ostium, elective implantation of 2 stents is usually required. Conversely, if the SB is smaller than 2.25 mm with focal disease localized to within 3 mm from the ostium a provisional stenting approach is suggested.
Regarding the 2-stent techniques, there are currently no data favouring a specific technique. In general, the type of stenting technique is decided according to the bifurcation angle and extent of disease proximal to the bifurcation: V-stenting is preferred when there is no disease proximal to the bifurcation; T stenting when the disease extends proximal to the bifurcation and the SB has a 90° angle of origin from the MB; and finally a crush (or TAP) is suggested when the disease extends proximal to the bifurcation and the SB originates with a 60° or less angle.
2) Restenosis at the SB ostium
Even with DES, restenosis at the SB ostium remains an important issue, regardless of the stenting technique employed. The positive aspect is that when it occurs with DES, it is very focal (<5 mm in length) and most of the times not associated with signs or symptoms of ischemia.
Costa et al (CitationCosta et al 2005) showed that angiography has a the limited ability to detect underexpanded stents implanted in bifurcations; consequently, we cannot exclude that the impact of SB stent underexpansion is currently underestimated, especially in patients with good angiographic results of both branches.
In the IVUS substudy of the SIRIUS trial, a MSA >5 mm2 for the total cohort and a MSA >4.5 mm2 for vessels <2.8 mm were thresholds predicting an “adequate” IVUS lumen at follow-up (CitationSonoda et al 2004) with a positive predictive value of 90%. In the study by Costa (CitationCosta et al 2005), MSA <5.0 mm2 was found in 80% of non-LM bifurcation lesions, and MSA <4.5 mm2 in 69% of stents with an mean reference diameter <2.8 mm, in both cases mostly in the SB ostium. Thus, MSA was frequently below the threshold associated with restenosis, especially at the SB ostium. Sub-optimal coverage with stent struts and heterogeneous drug delivery are probably potential contributing factors to the increased SB ostial restenosis.
3) Stent thrombosis
The multiple layers of stent struts apposed to the vessel wall with some of the 2-stent techniques have raised concerns about a possible increased risk of stent thrombosis following DES implantation (CitationVirmani et al 2004). Conflicting data are presently reported in the literature. Bifurcation lesions has been reported to be independent predictors of stent thrombosis (CitationIakovou et al 2005b) (CitationAngiolillo et al 2005). Interestingly, in the substudy (CitationColombo et al 2005) from the ARTS 2 study, the occurrence of stent thrombosis did not differ between the bifurcation and non-bifurcation groups. In the SES bifurcation study (CitationColombo et al 2004) the overall stent thrombosis rate was 3.5%, increasing to 4.6% if the patient with sudden death is included and up to 6.3% if only the 2-stent group is considered. All thromboses occurred in patients taking double antiplatelet therapy, however, the 2 cases of early thrombosis at day 1 and 3 were associated with a clear suboptimal angiographic result (dissection distal to the SB stent) and with a lack of GP IIb/IIIa inhibitor treatment. However, it is reassuring that in the Nordic trial, only 1 episode of definite stent thrombosis occurred and this was in a patient treated with 1 stent only (CitationSteigen et al 2006).
Conclusions
The introduction of SES has markedly improved the outcomes after the treatment of bifurcation lesions as compared to historical BMS controls. However, this subset of lesions remains a challenge for the interventional cardiologist and is still associated with procedural complications due to plaque shift, suboptimal angiographic results, and difficulty in crossing the stent struts, incomplete coverage of the SB ostium and, despite DES use, persistence of restenosis, especially at the SB ostium.
It is not clear yet which is the optimal stent strategy in this subset of lesions. In addition, no study has addressed so far which among the different 2 stenting techniques should be the preferred when both branches DES implantation is chosen.
Additional information and insights on the efficacy and safety of the 1-stent versus a specific 2-stent approach in true bifurcation lesions will come from the “Coronary bifurcations: Application of the Crushing Technique Using Sirolimus-eluting stents” (CACTUS) study. This study has already randomized more than 350 patients with de novo bifurcations to either a provisional strategy or the crush technique, using Cypher™ stents. The primary endpoints of the study are in-segment restenosis and 6 and 12-month MACE rates.
Finally, the introduction of dedicated DES for different bifurcations types may further facilitate the conquest of one of the most challenging areas in interventional cardiology. These dedicated bifurcation stents are specifically designed to provide good deliverability, secured access to the side branch, complete coverage of the lesion site without double/triple layers of stent struts, and thereby ensuring drug availability to all diseased surfaces.
Acknowledgements
We thank Dr Azeem Latib for reviewing the syntax of the paper.
References
- AiroldiFStankovicGOrlicDThe modified T stenting technique with crushing for bifurcation lesions: immediate results and 6-month clinical outcomesAm J Cardiol200392Suppl64L12842250
- Al SuwaidiJBergerPBRihalCSImmediate and long-term outcome of intracoronary stent implantation for true bifurcation lesionsJ Am Coll Cardiol2000359293610732890
- Al SuwaidiJYehWCohenHAImmediate and one-year outcome in patients with coronary bifurcation lesions in the modern era (NHLBI dynamic registry)Am J Cardiol20018711394411356386
- AliabadiDTilliFVBowersTRIncidence and angiographic predictors of side branch occlusion following high-pressure intracoronary stentingAm J Cardiol19978099479352966
- AngiolilloDJFernandez-OrtizABernardoEIdentification of low responders to a 300-mg clopidogrel loading dose in patients undergoing coronary stentingThromb Res2005115101815567460
- CervinkaPStasekJPleskotMTreatment of coronary bifurcation lesions by stent implantation only in parent vessel and angioplasty in sidebranch: immediate and long-term outcomeJ Invasive Cardiol2002147354012454336
- ChevalierBGlattBRoyerTPlacement of coronary stents in bifurcation lesions by the “culotte” techniqueAm J Cardiol19988294399794349
- ColomboABifurcational lesions and the “crush” technique: understanding why it works and why it doesn’t-a kiss is not just a kissCatheter Cardiovasc Interv200463337815505834
- ColomboAGaglioneANakamuraS“Kissing” stents for bifurcational coronary lesionCathet Cardiovasc Diagn199330327308287462
- ColomboAIakovouIDrug-eluting stents: the new gold standard for percutaneous coronary revascularisationEur Heart J2004a25895715172459
- ColomboAIakovouITen years of advancements in interventional cardiologyJ Endovasc Ther2004b11Suppl 2II10815760258
- ColomboAMosesJWMoriceMCRandomized study to evaluate sirolimus-eluting stents implanted at coronary bifurcation lesionsCirculation20041091244914981005
- ColomboAStankovicGOrlicDModified T-stenting technique with crushing for bifurcation lesions: immediate results and 30-day outcomeCatheter Cardiovasc Interv2003601455114517916
- CostaRAMintzGSCarlierSGBifurcation coronary lesions treated with the “crush” technique: an intravascular ultrasound analysisJ Am Coll Cardiol20054659960516098422
- FujiiKKobayashiYMintzGSDominant contribution of negative remodeling to development of significant coronary bifurcation narrowingAm J Cardiol200392596112842248
- GeLAiroldiFIakovouIClinical and angiographic outcome after implantation of drug-eluting stents in bifurcation lesions with the crush stent technique: importance of final kissing balloon post-dilationJ Am Coll Cardiol2005a466132016098424
- GeLIakovouICosgraveJTreatment of bifurcation lesions with two stents: one year angiographic and clinical follow up of crush versus T stentingHeart200692371615964941
- GeLTsagalouEIakovouIIn-hospital and nine-month outcome of treatment of coronary bifurcational lesions with sirolimus-eluting stentAm J Cardiol2005b957576015757605
- GobeilFLefèvreTGuyonPStenting of bifurcation lesions using the Bestent: a prospective dual-center studyCatheter Cardiovasc Interv2002554273311948886
- HoyeAVan MieghemCOngATreatment of de novo bifurcation lesions: comparison of Sirolimus- and Paclitaxel-eluting stentsEuroIntervention200512430
- IakovouIGeLColomboAContemporary stent treatment of coronary bifurcationsJ Am Coll Cardiol2005a4614465516226167
- IakovouISchmidtTBonizzoniEIncidence, predictors, and outcome of thrombosis after successful implantation of drug-eluting stentsJama2005b29321263015870416
- JimMHHoHHMiuRModified crush technique with double kissing balloon inflation (sleeve technique): a novel technique for coronary bifurcation lesionsCatheter Cardiovasc Interv200667403916489571
- KastratiAMehilliJSchuhlenHA clinical trial of abciximab in elective percutaneous coronary intervention after pretreatment with clopidogrelN Engl J Med2004350232814724302
- KobayashiYColomboAAkiyamaTModified “T” stenting: a technique for kissing stents in bifurcational coronary lesionCatheter Cardiovasc Diagn1998433236
- LefèvreTLouvardYMoriceMCStenting of bifurcation lesions: classification, treatments, and resultsCatheter Cardiovasc Interv2000492748310700058
- LefèvreTLouvardYMoriceMCStenting of bifurcation lesions: a rational approachJ Interv Cardiol2001145738512053378
- LemosPASerruysPWVan DomburgRTUnrestricted utilization of sirolimus-eluting stents compared with conventional bare stent implantation in the “real world”: the Rapamycin-Eluting Stent Evaluated At Rotterdam Cardiology Hospital (RESEARCH) registryCirculation2004109190514691037
- MelikianNAiroldiFDi MarioCCoronary Bifurcation Stenting: Current techniques outcome and possible future developmentsMinerva Cardioangiol2004523657815514572
- MoussaILLanskyAJLasicZA prospective registry to evaluate sirolimus-eluting stents implanted at coronary bifurcation lesions using the “crush techniqueAm J Cardiol20069713172116635603
- OrmistonJACurrieEWebsterMWDrug-eluting stents for coronary bifurcations: insights into the crush techniqueCatheter Cardiovasc Interv200463332615505853
- PanMSDe LezoJSMedinaADrug-eluting stents for the treatment of bifurcation lesions: a randomized comparison between paclitaxel and sirolimus stentsAm Heart J200715315e1717174630
- PanMDe LezoJSMedinaARapamycin-eluting stents for the treatment of bifurcated coronary lesions: a randomized comparison of a simple versus complex strategyAm Heart J20041488576415523318
- PanMSuarez De LezoJMedinaAA stepwise strategy for the stent treatment of bifurcated coronary lesionsCatheter Cardiovasc Interv20025550711793495
- PopmaJLeonMTopolEAtlas of Interventional Cardiology1994Philadelphia PASaunders
- SafianRSafianRDFreedMSBifurcation lesions2001222Royal Oak, MIPhysician’s Press
- SawhneyNDamaniSPriceMTreatment of Bifurcation Lesions With Sirolimus-Eluting Stents Using the “Crush” and “V” Techniques. Procedural and Clinical outcomesPresented at the Scientific Sessions of the Trans Catheter Therapeutics, Washington2005
- SchampaertEFortSAdelmanAGThe V-stent: a novel technique for coronary bifurcation stentingCathet Cardiovasc Diagn19963932068933984
- SerruysPWOngAMoriceMCArterial Revascularisation Therapies Study Part II - Sirolimus-eluting stents for the treatment of patients with multivessel de novo coronary artery lesionsEuroIntervention20051147156
- SharmaSKSimultaneous kissing drug-eluting stent technique for percutaneous treatment of bifurcation lesions in large-size vesselsCatheter Cardiovasc Interv20056510615810018
- SheibanIAlbieroRMarsicoFImmediate and long-term results of “T” stenting for bifurcation coronary lesionsAm J Cardiol20008511414A910781768
- SianosGMorelMAKappeteinAPThe SYNTAX score: an angiographic tool grading the complexity of coronary artery diseaseEurointervention200512
- SonodaSMorinoYAkoJImpact of final stent dimensions on long-term results following sirolimus-eluting stent implantation: serial intravascular ultrasound analysis from the sirius trialJ Am Coll Cardiol20044319596315172398
- SpokojnyASanbornTEllisSGHolmesDRJrThe bifurcation lesionStrategic Approaches in Coronary Intervention1996288Baltimore, MDWilliams and Wilkins
- SteigenTKMaengMWisethRRandomized study on simple versus complex stenting of coronary artery bifurcation lesions: the Nordic bifurcation studyCirculation200611419556117060387
- TakebayashiHKobayashiYDangasGRestenosis due to underexpansion of sirolimus-eluting stent in a bifurcation lesionCatheter Cardiovasc Interv200360496914624428
- TanabeKHoyeALemosPARestenosis rates following bifurcation stenting with sirolimus-eluting stents for de novo narrowingsAm J Cardiol200494115815219520
- TsuchidaKColomboALefèvreTThe clinical outcome of percutaneous treatment of bifurcation lesions in multivessel coronary artery disease: Insights from the Arterial Revascularization Therapies Study part II (ARTS II)Eur Heart J200728443542
- VirmaniRGuagliumiGFarbALocalized hypersensitivity and late coronary thrombosis secondary to a sirolimus-eluting stent: should we be cautious?Circulation2004109701514744976
- YamashitaTNishidaTAdamianMGBifurcation lesions: two stents versus one stent—immediate and follow-up resultsJ Am Coll Cardiol20003511455110758954