Abstract
The phenomenon of ischemic preconditioning has been recognized as one of the most potent mechanisms to protect against myocardial ischemic injury. In experimental animals and humans, a brief period of ischemia has been shown to protect the heart from more prolonged episodes of ischemia, reducing infarct size, attenuating the incidence, and severity of reperfusion-induced arrhythmias, and preventing endothelial cell dysfunction. Although the exact mechanism of ischemic preconditioning remains obscure, several reports indicate that this phenomenon may be a form of receptor-mediated cardiac protection and that the underlying intracellular signal transduction pathways involve activation of a number of protein kinases, including protein kinase C, and mitochondrial KATP channels. Apoptosis, a genetically programmed form of cell death, has been associated with cardiomyocyte cell loss in a variety of cardiac pathologies, including cardiac failure and those related to ischemia/reperfusion injury. While ischemic preconditioning significantly reduces DNA fragmentation and apoptotic myocyte death associated with ischemia-reperfusion, the potential mechanisms underlying this effect have not been fully clarified. A comprehensive understanding of these mechanisms and application to clinical scenarios will provide new directions in research and translate this information into new treatment approaches for reducing the extent of ischemia/reperfusion injury.
Preconditioning in experimental studies
In 1986, a group of investigators studying the intracellular changes of glycolytic products at different time points of myocardial ischemia in a canine model, observed that four cycles of 5 minutes ischemia and reperfusion prior to a more sustained episode of 40 min ischemia reduced considerably myocardial infarction compared with the control (CitationMurry et al 1986). This was the first description of an endogenous protective phenomenon called ischemic preconditioning. The same beneficial effect was since then confirmed in every species that was studied, independently of the presence of collaterals in the coronary circulation and independently of the size of the animal model (CitationSchott et al 1990; CitationLiu et al 1991; CitationLiu and Downey 1992). Early studies mostly focused on the investigation of the natural history of preconditioning in terms of the number of brief ischemic episodes, the duration of each ischemic insult, the duration of the reperfusion interval that would separate the last cycle of preconditioning from the following sustained episode of ischemia and finally the duration of the prolonged ischemia in order the preconditioning to be effective (Citationvan Winkle et al 1991; CitationIliodromitis et al 1996). Species differences were observed regarding the number of brief episodes of ischemia: increased number of ischemic bursts was effective in protecting the dog heart (CitationLi et al 1990) whereas protection was lost after a certain number of ischemic-reperfusion stimuli in the rabbit heart (CitationCohen et al 1994; CitationIliodromitis et al 1997).
The preconditioned state is very transient following a preconditioning protocol and lasts for only 1–2 h in anesthetized animals (Citationvan Winkle et al 1991; CitationJenkins et al 1995; CitationIliodromitis et al 1996). This constitutes the classic preconditioning or first window of myocardial protection. Of note, later experimental studies revealed that, while the provided protection is lost after this reperfusion interval and the heart remains unprotected for several hours, the protective effect re-appears after 24 hours and lasts up to 72 hours (CitationYellon and Baxter 1995; CitationYang et al 1996). This is the delayed phase of preconditioning or the second window of protection, which starts with no additional intervention, it is more prolonged although less robust.
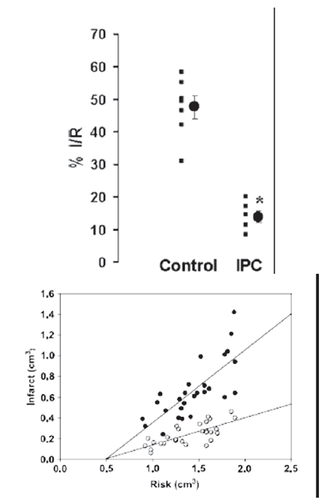
The golden standard of the effectiveness of preconditioning is the reduction of the infarct size (). However, there is a series of other benefits obtained from preconditioning and among these are the reduction of lethal arrhythmias and the better recovery of post-ischemic left ventricular function (CitationShiki and Hearse 1987; CitationPrzyklenk 2000; CitationYellon and Downey 2003).
Figure 1 The effect of ischemic preconditioning on infarct size after ischemia/reperfusion. Upper panel:infarct size expressed as percent of risk zone size in control and preconditioned (IPC) rabbit hearts (from CitationIliodromitis et al 2006); lower panel: the absolute infarct volume plotted against absolute risk zone volume from control (closed symbols) and preconditioned (open symbols) hearts (from CitationIliodromitis et al 2004).
After the initial studies that elucidated the natural history of preconditioning in terms of the proper ischemic stimuli and time intervals, later experimental studies investigated the mechanisms that are involved in the protection mediated by preconditioning. The first breakthrough in this direction was the report by Downey and colleagues (CitationLiu et al 1991) that the adenosine A1 receptor acts to trigger ischemic preconditioning’s protection in the rabbit heart, revealing that ischemic preconditioning is receptor mediated. It has now become established that the protection is receptor mediated, and a major objective in recent years has been the identification of the triggers, mediators and end effectors in the myocyte that are activated during ischemic preconditioning.
Activation of specific receptors on the cardiomyocyte cell membrane such as adenosine A1 and A3, bradykinin B2, α1-adrenergic, δ-opioid, and others, initiate a series of signal transduction cascades that carry the signal for protection and those presumably terminate on one or more end-effectors (CitationLiu et al 1991; CitationCohen et al 2001; CitationSchulz et al 2001). In recent years, much research has focused on the key role of the mitochondrial KATP channel as both a trigger and distal effector in preconditioning with equivocal results (CitationPain et al 2000; CitationFryer et al 2000; CitationSato et al 2000; CitationIliodromitis et al 2003; CitationO’Rourke 2004). The signal transduction pathways downstream of the trigger are complex and a detailed description is beyond the scope of this review. However, it is clear that multiple protein kinases are involved, notably one or more isoforms of protein kinase C, at least two tyrosine kinases (eg, Src and PI3 kinase), as well as mitogen-activated protein kinases (CitationBaines et al 1998; CitationIliodromitis et al 1998; CitationHarada et al 2004; CitationArmstrong 2004; CitationHausenloy et al 2005). Reperfusion injury salvage kinase (RISK) pathway has emerged as a concept and describes a group of survival protein kinases, which include Akt and Erk1/2 that confer powerful cardioprotection against lethal reperfusion injury when specifically activated at the time of reperfusion (CitationHausenloy and Yellon 2007). The cardioprotective effect of ischemic preconditioning is completely aborted by inhibiting RISK pathway (CitationHausenloy et al 2005).
More recently another endogenous mechanism of protection, called postconditioning, was described. In brief, a series of very short-lived episodes of ischemia and reperfusion applied at the onset of reperfusion after an index ischemic event reduce the infarct size. Postconditioning is more easily applicable and does not require fore-knowledge of a potentially lethal ischemic event. RISK pathway is also involved in the cardioprotective mechanism of postconditioning and the inhibition of PI3 kinase abrogates protection conferred by postconditioning (CitationTsang et al 2004). It has been suggested that the RISK pathway “unites” both ischemic preconditioning and postconditioning at the time of reperfusion (CitationHausenloy and Yellon 2007).
Preconditioning in humans
The acquired experience from the experimental studies was transferred to humans and the protective effect of preconditioning was examined using direct or indirect observations (CitationKloner et al 1995a, Citation1995b; CitationAndreotti et al 1996; CitationKobayashi et al 1997; CitationKarbanda et al 2001). It is difficult to transfer the strict laboratory conditions regarding the number and the duration of episodes of ischemia and reperfusion, into the clinical reality, so much for practical reasons as well as for ethical reasons. Thus, the final end points for the assessment of protection in humans are more or less indirect. Furthermore, the precise estimation of the infarct size and the area at risk is not very easy to be determined in humans and therefore the beneficial effect of preconditioning is difficult to be assessed. However, as in the experimental models, other surrogate end-points are used for the expression of the salutary effect of preconditioning and among these are the reduction of the episodes of angina after an initial episode, the reduction of ST deviation on the electrocardiogram, the reduction of lethal arrhythmias, a smaller peri-operative infarction, a better survival of the patients with pre-infarction angina and others (CitationTomai et al 1996, Citation1997; CitationIshihara et al 1997; CitationGheeraert et al 2001).
The preconditioning studies can be divided into observational, provocative, and pharmacological. In the first category belong those studies where the patients describe alleviation of their symptoms or there is an objective method which can confirm the benefit of preconditioning. In fact, many patients report an episode of angina early in the morning, called walk-through or warm up angina and they remain free of symptoms later and for the rest of the day (CitationPrzyklenk and Kloner 1999; CitationSchwarz et al 1999). There are a large number of clinical studies which have shown that pre-infarction angina acts as preconditioning stimulus and the patients develop smaller CK-determined myocardial infarction in comparison to the patients without pre-infarction angina. In the objective studies, it is feasible to describe the effect of an intervention that may act as a preconditioning analogue. In this regard, less ST segment shift, less extent of angina and less lactate production at the second balloon inflation compared to the first are some surrogate end-points attributed to an effect called coronary angioplasty-related preconditioning (CitationTomai et al 1996, Citation1997). Furthermore, there is evidence that the second exercise treadmill test becomes better in comparison to the first and this may express an early or delayed preconditioning effect (CitationParaskevaidis et al 2005). Objective description of preconditioning has been also obtained from histological studies of tissue samples like atrial trabeculae or ventricular tissue taken at the time of operation or by the peripheral markers that have been used for the expression of preconditioning (CitationYellon et al 1993; CitationJenkins et al 1997).
Another interesting issue is the pharmacological stimulation of preconditioning and the expectation that several agents involved in the mechanism of protection could become safe and easily applicable preconditioning mimetics. Adenosine, acadesine, ACE inhibitors which prevent bradykinin degradation, nicorandil, and others have been used in clinical studies. In the AMISTAD study, adenosine has been used in parallel with thrombolysis in patients with evolving myocardial infarction and resulted in reduction of the infarct size in anterior myocardial infarction despite the fact that it was administered after the onset of chest pain (CitationMahaffey et al 1999). In the AMISTAD II study, the adenosine was given in anterior myocardial infarctions only at two different doses and again it was shown that at a dose of 70 μg/kg min for 3 hours and in parallel with thrombolysis, it reduced the infarct size especially if the thrombolysis started within the first 3 hours (CitationRoss et al 2005). Acadesine, which is an agent that facilitates the effect of adenosine, was used in patients who underwent CABG. Patients treated with acadesine had fewer postoperative myocardial infarctions and better clinical outcome (CitationMangano et al 2006). Nicorandil, which opens the mitochondrial KATP channels, has been used in two multicenter clinical trials, CEASAR-2 and IONA, with very promising results (CitationPatel et al 1999; Citationthe IONA study group 2002). These clinical results suggest that the cardioprotective effects of preconditioning, well described in animal studies, do appear to translate to clinical setting. However, direct translation of experimental observations to therapeutic intervention is hampered by factors encountered in clinical practice such as the necessity of proper time of intervention, the proper duration of the treatment and of course the appropriate dosage of drugs.
Apoptosis in the heart
While ischemic injury has long been considered to result in necrotic tissue damage, studies over the past 15 years have focused attention on apoptosis as a significant component of cell loss during reperfusion injury following myocardial infarction (CitationGottlieb et al 1994; CitationFliss and Gattinger 1996; CitationGottlieb and Engler 1999; CitationElsasser et al 2001). Myocardial apoptosis has also been documented in response to a variety of other cardiac stresses including pressure or volume overload, heart failure, diabetic cardiomyopathy, atherosclerosis and anti-cancer agents (CitationHaunstetter and Izumo 1998; CitationFeuerstein and Young 2000; CitationValen 2003; CitationSingal et al 2000).
Cardiomyocytes undergoing necrosis and apoptosis show characteristic but morphologically and biologically distinct features. Necrosis, also called oncosis in the setting of ischemia/reperfusion, is an uncontrolled, irreversible process characterized by severe cell swelling, ATP depletion, denaturation and coagulation of cytoplasmic proteins, breakdown of cell organelles and disruption of cell membrane (CitationSearle et al 1982; CitationMajno and Joris 1995). It is a destructive process as release of cellular content into the surrounding environment provokes inflammation and can cause further damage or death to neighboring cells. In contrast, apoptosis is a genetically controlled, highly regulated process whereby the cell commits suicide without inducing inflammatory response. Apoptosis usually requires energy and it is characterized by cell shrinkage, chromatin condensation, DNA fragmentation, membrane blebbing and formation of apoptotic bodies (CitationMajno and Joris 1995; CitationSaraste and Pulkki 2000; CitationBuja 2005). The hallmark of apoptosis in intact cells is endonucleolytic digestion of nuclear DNA into oligonucleosome-sized fragments (200 bp), in contrast to nonspecific degradation of DNA into pieces of random size after loss of membrane integrity.
The regulated disassembling of cellular contents, which is a feature of apoptosis, is largely conducted by a family of cysteine dependent aspartate-directed proteases, the caspases (CitationWang and Lenardo 2000). Fourteen members of this family have been identified in mammals. Caspases-2, -9, -8, and -10 are considered apoptosis initiators, and serve to cleave and activate apoptosis effectors (caspases-3, -6, and -7). All caspases are synthesized as zymogens that contain a prodomain, a large subunit and a small subunit, and activation of these enzymes is by proteolytic cleavage. Once activated, initiator caspases cleave and activate effector caspases and a proteolytic cascade is initiated.
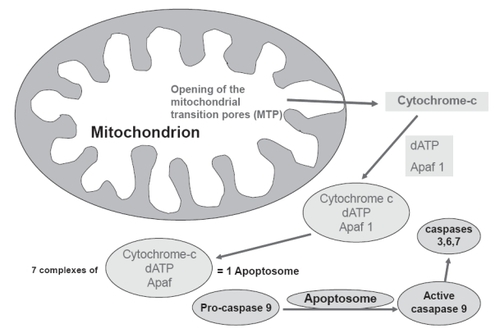
There are two principal pathways that lead to caspase activation: the extrinsic and intrinsic cell death pathways (CitationDanial and Korshmeyer 2004). The extrinsic pathway requires the activation of cell surface death receptors (DRs) by specific ligands, and allows the cell to respond directly to the immediate environment (). The vast majority of death receptors belong to the tumor necrosis factor receptor (TNFR) superfamily, which includes Fas, TNFR1, and DR3–DR6. The binding of death ligands, such as Fas ligand or TNF-α, to their cognate receptors at the plasma membrane causes homotrimerization of the receptor and recruitment of specific adaptor proteins, such as Fas-associated death domain and procaspase-8, into a death-inducing signaling complex (DISC). This, in turn, leads to activation of initiator caspase-8, which subsequently activates effector caspases 3, 6, and 7 (CitationHirata et al 1998; CitationDanial and Korshmeyer 2004). In contrast, in the intrinsic pathway (), the mitochondria detect and respond to unfavorable changes in the internal environment and play a central role in the integration and execution of a wide variety of apoptotic signals. The mitochondria provide the energy required for execution of the apoptotic program and release of pro-apoptotic proteins such as cytochrome c, endonuclease G, and apoptosis-inducing factor. Release of these substances occurs during opening of the mitochondrial permeability transition (MPT) pore, a large non-selective ion channel in the outer mitochondrial membrane. Gating of the MPT pore is controlled by a combination of calcium, redox potential, pH and transmembrane voltage; when the MPT is opened, the normally impervious mitochondrial membrane undergoes a reversible transition to permeability (CitationZoratti and Szab’o 1995; CitationChelli et al 2001). Either brief or sustained MPT opening can lead to apoptosis (CitationBishopric et al 2001). On release from mitochondria, cytochrome c forms a complex with procaspase-9 and a cytosolic cofactor, Apaf-1 (CitationLi et al 1997; CitationZou et al 1999). In the presence of sufficient ATP, caspase-9 undergoes autocatalytic cleavage to create an active ‘apoptosome’ that cleaves caspase-3 and initiates the apoptotic program. Thus, the extrinsic and intrinsic pathways have different initiator caspases but converge at the level of the effector caspases.
Figure 2 Schematic representation of the death receptor (extrinsic) pathway of caspase activation to provoke the mechanism of apoptosis.
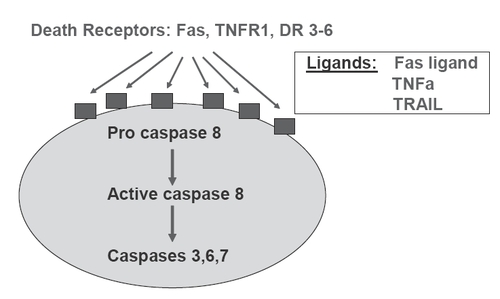
Figure 3 Schematic representation of the mitochondrial death (intrinsic) pathway leading to the formation of apoptosome, activation of caspases and apoptosis.
The intrinsic pathway of apoptosis is regulated by members of the Bcl-2 family. This family is composed of anti-apoptotic eg, Bcl2, Bcl-xL, Bcl-w, A1, and Mcl-1 and pro-apoptotic proteins eg, Bax, Bad, Bak, Bid, Bim, Bnip3, Bnip3L (Nix), and Bik. All of these proteins possess up to four conserved regions known as Bcl-homology (BH) domains (CitationCory et al 2003). The principal site of action of the Bcl-2 family proteins is at the mitochondria, where they regulate cytochrome c release and caspase activation. The exact mechanisms by which Bcl-2 proteins modulate apoptosis are still subject to much debate and controversy. One hypothesis is that both pro-apoptotic and anti-apoptotic Bcl-2 proteins bind directly to components of the mitochondrial pore, leading to either its opening or closure, respectively (CitationGross et al 1999; CitationMattson and Kroemer 2003). A second hypothesis is that upon activation, pro-apoptotic members such as Bax and Bak are inserted into the outer mitochondrial membrane where they oligomerize to form a protein-permeant pore of their own (CitationMattson and Kroemer 2003).
The most clinical relevant stimulants, which initiate the process of apoptosis apart from ischemia/reperfusion, include pressure or volume overload, cellular calcium overload, oxygen derived free radicals, increased levels of catecholamines and angiotensin II, Fas ligand, TNF-α, as well as decreased coronary flow reserve (CitationKhoynezhad et al 2004; CitationScarabelli et al 2006). It is obvious that there is a complex interrelation between all the above factors. Decreased coronary flow reserve, for example, results in periods of ischemia and reperfusion and in generation of oxygen-derived free radicals. Angiotensin II may cause pressure overload and heart failure results in increased circulating catecholamine levels. All the above mentioned conditions may lead to contractile dysfunction of the heart, to dysrhythmias and to cell death because of apoptosis or necrosis. The rationale of current therapy is mainly to modify myocyte dysfunction and to minimize the intensity of the lethal injury acting on the heart. Well documented clinical interventions such as restoration of ischemia by pharmacological or interventional means, valve replacement or surgical correction of any anatomic abnormalities which may be considered responsible for pressure or volume overload, use of beta blockers, ACE inhibitors or angiotensin II receptor antagonists may prevent, suppress or restore cardiac dysfunction. However, preservation of cells subjected to lethal injury remains an attractive goal and inhibition of cardiac myocyte apoptosis may represent a novel approach for treatment of cardiac disease. For this reason, a better understanding of the pathways of apoptosis and their regulation is required. Therapeutic approaches such as the use of inhibitors of TNF-α, caspases and sodium-hydrogen exchanger, upregulation of insulin like growth factor-1, antioxidants, ischemic preconditioning, which will be discussed in the next section, and others are currently under investigation (CitationGill et al 2002; CitationKhoynezhad et al 2004).
Preconditioning and apoptosis
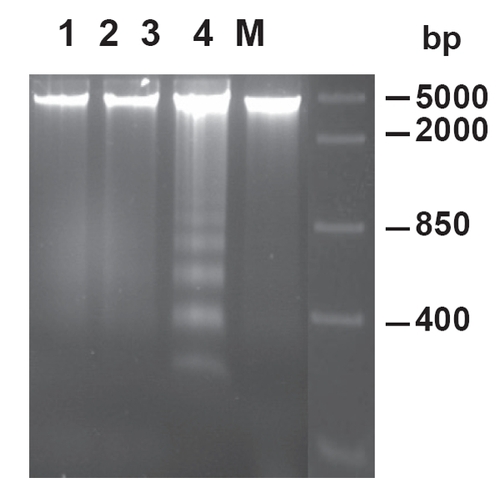
Accumulating evidence from in vivo and in vitro studies suggests that ischemic preconditioning significantly reduces DNA fragmentation () and apoptotic myocyte death that is associated with ischemia/reperfusion in isolated rabbit and rat heart (CitationGottlieb et al 1996; CitationMaulik et al 1999; CitationNakamura et al 2000; CitationZhao and Vinten-Johansen 2002; CitationLazou et al 2006). In addition, activation of receptors that are involved in the initiation of the mechanism of preconditioning, such as δ-opioid and bradykinin, also results in reduced apoptosis after ischemia/reperfusion (Okubo et al 2004; CitationFeng et al 2005). It is clear from these studies that attenuation of apoptosis by ischemic preconditioning is associated with a reduction in infarct size analysed early at reperfusion. It is not known, however, whether a reduction in infarct size measured days after reperfusion is achieved by inhibiting apoptosis since apoptosis progresses after reperfusion over a number of days. The potential mechanisms underlying preconditioning attenuated myocardial apoptosis have not been fully clarified and they are under intense investigation. However, a number of mediators have been implicated.
Figure 4 Effect of ischemic preconditioning on DNA fragmentation in rabbit hearts subjected to ischemia/reperfusion Lane 1 represents control non-ischemic tissue; lane 2 represents ischemic tissue after ischemia without reperfusion; lanes 3 and 4 represent ischemic tissue after ischemia/reperfusion in nonpreconditioned and preconditioned hearts, respectively. M, marker lane (from CitationLazou et al 2006).
Several studies have shown that preconditioning inhibits apoptosis by reducing the burst of reactive oxygen species generated from inflammatory cells (ie, PMNs and macrophages) and noninflammatory cell types (ie, endothelial cells and myocytes). In this regard, antioxidants and free radical scavengers have been reported to inhibit the appearance of apoptosis (CitationKarzelewski et al 1999; CitationZhao and Vinten-Johansen 2002). Other studies have implicated that preconditioning reduces myocardial apoptosis through altering the balance between anti-apoptotic and pro-apoptotic proteins, the release of cytochrome c from mitochondria, caspase activation, and activation of protein kinase C isozymes. Preconditioning causes a decrease in pro-apoptotic Bax and increase in the anti-apoptotic Bcl-2 proteins resulting in an altered Bcl-2/Bax ratio and attenuation of cytochrome c release from mitochondria (CitationMaulik et al 1999, Citation2000; CitationNakamura et al 2000). Inhibition of caspase activity, a key event in the development of apoptosis, has also been demonstrated in preconditioning (CitationPiot et al 1999). A reduction in ceramide production during sustained ischemia has been suggested to reduce apoptosis in rabbit hearts (CitationArgaud et al 2004). However, an interrelationship between changes in the expression of Bcl-2 family proteins, mitochondrial activity and reduction of apoptosis after ischemia/reperfusion by ischemic preconditioning needs to be further investigated in in vivo models.
As discussed above, PKC has a central role in ischemic preconditioning. In particular, activation of PKCε is important in the preservation of cell viability. Although the effect of ischemic preconditioning on necrosis through activation of PKC isoforms has been intensively investigated (CitationYellon and Downey 2003), only a few studies have shown that preconditioning reduces apoptosis by a PKC-dependent pathway. CitationOkamura et al (1999) showed that blockade of PKC may interrupt the protective effect of preconditioning and simultaneously it may promote the mechanism of apoptosis. Furthermore, PKCε but not PKCδ is involved in the inhibition of apoptosis by preconditioning after simulated ischemia and reoxygenation (CitationLiu et al 2001).
The mitochondrial KATP channels significantly contribute to the mechanism of protection in ischemic preconditioning by the generation of the oxygen-derived free radicals. Opening of these channels by pharmacological means like nicorandil or diazoxide, trigger the mechanism of protection while the addition of 5HD blunts this effect (CitationPain et al 2000; CitationSato et al 2000; CitationIliodromitis et al 2003; CitationO’Rourke 2004). It is of interest that diazoxide is also capable in preventing apoptosis and again the simultaneous use of 5HD abolishes this benefit (CitationArdehali et al 2005). In addition to direct effects on mitochondrial function, opening of mitochondrial KATP channels may have secondary effects on cell signaling such as activation of PKCε (CitationLiu et al 2002).
As mentioned above, activation of kinases of the RISC pathway has been implicated in mediating the cardioprotection associated with ischemic preconditioning (CitationHousenloy et al 2005; CitationHausenloy and Yellon 2007). Recent studies have shown that pharmacological activation of these kinases is associated with recruitment of anti-apoptotic signaling components such as the phosphorylation and inhibition of the proapoptotic proteins Bax and Bad, the inhibition of caspase 3 activation, the phosphorylation and activation of p70S6K (which acts to inhibit Bad) and the phosphorylation and activation of the antiapoptotic protein Bcl-2 (CitationHarada et al 2001; CitationHausenloy and Yellon 2007). In addition, the inhibition of the mitochondrial permeability transition pore (MTP), a mitochondrial channel which mediates cell death at the time of myocardial reperfusion by uncoupling oxidative phosphorylation and inducing mitochondrial swelling (CitationHausenloy and Yellon 2003), has been identified as a downstream target of the RISK pathway (CitationDavidson et al 2006; CitationBopassa et al 2006). Although it has been shown that ischemic preconditioning prevents the increased permeability of the transition pore by the activation of kinases, Akt, PI3 kinase, and ERK1/2, the mechanism through which the RISK pathway inhibits the opening of the MTP is unclear.
In conclusion, ischemic preconditioning is a protective mechanism in limiting the infarct size and there is a great body of evidence that it reduces both necrosis and apoptosis. We expect that in the future the acquired experience and the increased knowledge of the underlying mechanisms in preconditioning and apoptosis would allow a more appropriate use of the proper pharmacological agents that would mimic preconditioning and that confer reduction of both necrosis and apoptosis. However, the translation of the laboratory findings in the clinical practice should be performed very cautiously and with prudence.
References
- AndreottiFPasceriVHackettDRPreinfarction angina as a predictor of more rapid coronary thrombolysis in patients with acute myocardial infarctionN Engl J Med19963347127494588
- ArdehaliHO’RourkeBMitochondrial KATP channels in cell survival and deathJ Mol Cell Cardiol20053971615978901
- ArgaudLPrigentAFChalabreysseLCeramide in the antiapoptotic effect of ischemic preconditioningAm J Physiol2004286H24651
- ArmstrongSCProtein kinase activation and myocardial ischemia/reperfusion injuryCardiovasc Res2004614273614962474
- BainesCPWangLCohenMVProtein tyrosine kinase is downstream of protein kinase C for ischemic preconditioning’s anti-infarct effect in the rabbit heartJ Mol Cell Cardiol199830383929515015
- BishopricNHAndrekaPSlepakTIMolecular mechanisms of apoptosis in the cardiac myocyteCurr Opin Pharmacol200111415011714088
- BopassaJCFerreraRGateau-RoeschOPI 3-kinase regulates the mitochondrial transition pore in controlled reperfusion and postconditioningCardiovasc Res2006691788516216231
- BujaLMMyocardial ischemia and reperfusionCardiovasc Pathol200514170516009313
- ChelliBFalleniASalvettiFPeripheral-type benzodiazepine receptor ligands: mitochondrial permeability transition induction in rat cardiac tissueBiochem Pharmacol20016169570511266654
- CohenMVYangXMDowneyJMConscious rabbits become tolerant to multiple episodes of ischemic preconditioningCirc Res19947499810048156647
- CohenMVYangXMLiuGSAcetylcholine, bradykinin, opioids and phenylephrine, but not adenosine, trigger preconditioning by generating free radicals and opening mitochondrial KATP channelsCirc Res200189273811485978
- CorySHuangDCAdamsJMThe Bcl-2 family: roles in cell survival and oncogenesisOncogene200322859060714634621
- DanialNNKorsmeyerSJCell death: critical control pointsCell20041162051914744432
- DavidsonSMHausenloyDDuchenMRSignalling via the reperfusion injury signalling kinase (RISK) pathway links closure of the mitochondrial permeability transition pore to cardioprotectionInt J Biochem Cell Biol2006384141916280253
- EeftingFRensingBWigmanJRole of apoptosis in reperfusion injuryCardiovasc Res2004614142614962473
- ElsasserASuzukiKLorenz-MeyerSThe role of apoptosis in myocardial ischemia: a critical appraisalBasic Res Cardiol2001962192611403415
- FengJBianchiCSandmeyerJLBradykinin preconditioning improves the profile of cell survival proteins and limits apoptosis after cardioplegic arrestCirculation2005112Suppl II190516159814
- FeuersteinGZYoungPRApoptosis in cardiac diseases: Stress- and mitogen-activated signaling pathwaysCardiovasc Res200045560910728377
- FlissHGattingerDApoptosis in ischemic and reperfused rat myocardiumCirc Res199679949568888687
- FryerRMEellsJTHsuAKIschemic preconditioning in rats: role of mitochondrial KATP channel in preservation of mitochondrial functionAm J Physiol2000278H30512
- GheeraertPJHenriquesJPSDe BuyzereMLPreinfarction angina protects against out-of-hospital ventricular fibrillation in patients with acute occlusion of the left coronary arteryJ Am Coll Cardiol20013813697611691510
- GillCMestrilRSamaliALosing heart: the role of apoptosis in heart disease-a novel therapeutic target?FASEB J2002161354611818361
- GottliebRABurlesonKOKlonerRAReperfusion injury induces apoptosis in rabbit cardiomyocytesJ Clin Invest1994941621287929838
- GottliebRAGruolDLZhuJYPreconditioning rabbit cardiomyocytes: role of pH, vacuolar proton ATPase, and apoptosisJ Clin Invest199697239188636421
- GottliebRAEnglerRLApoptosis in myocardial ischemia-reperfusionAnn NY Acad Sci19998744122610415551
- GrossAMcDonnellJMKorsmeyerSJBcl-2 family members and the mitochondria in apoptosisGenes Dev19993189991110444588
- HaradaHAndersenJSMannMp70S6 kinase signals cell survival as well as growth, inactivating the pro-apoptotic molecule BADProc Natl Acad Sci USA20019896667011493700
- HaradaNMiuraTDairakuYNO donor-activated PKC delta plays a pivotal role in ischemic myocardial protection through accelerated opening of K-ATP mitochondrial channelsJ Cardiovasc Pharmacol200444354115175555
- HaunstetterAIzumoSApoptosis: basic mechanisms and implications for cardiovascular diseaseCirc Res1998821111299633912
- HausenloyDJYellonDMThe mitochondrial permeability transition pore: its fundamental role in mediating cell death during ischaemia and reperfusionJ Mol Cell Cardiol2003353394112689812
- HausenloyDJTsangAMocanuMIschemic preconditioning protects by activating prosurvival kinases at reperfusionAm J Physiol2005288H971H976
- HousenloyDJYellonDMReperfusion injury salvage kinase signalling:taking a RISK for cardioprotectionHeart Fail Rev2007122173417541822
- HirataHTakahashiAKobayashiSCaspases are activated in a branched protease cascade and control distinct downstream processes in Fas-induced apoptosisJ Exp Med19981875876009463409
- IliodromitisEKPapadopoulosCParaskevaidisIAProtection from preconditioning can be reinstated at various reperfusion intervalsCardiovasc Drugs Ther19961034168877077
- IliodromitisEKKremastinosDTKatritsisDGMultiple cycles of preconditioning cause loss of protection in open-chest rabbitsJ Mol Cell Cardiol199729915209152852
- IliodromitisEKMikiTLiuGSThe PKC activator PMA preconditions rabbit heart in the presence of adenosine receptor blockade: is 5’-nucleotidase important?J Mol Cell Cardiol1998302201119925358
- IliodromitisEKCokkinosPZogaAOral nicorandil recaptures the waned protection from preconditioning in vivoBr J Pharmacol2003381101612684266
- IliodromitisEKTasouliAAndreadouIIntravenous atenolol and esmolol maintain the protective effect of ischemic preconditioning in vivoEur J Pharmacol2004499163915363963
- IliodromitisEKCaitanakiCLazouADifferential activation of mitogen-activated kinases in ischemic and nitroglycerin-induced preconditioningBasic Res Cardiol20061013273516612556
- IshiharaMSatoHTateishiHImplications of prodromal angina pectoris in anterior wall acute myocardial infarction: acute angiographic findings and long-term prognosisJ Am Coll Cardiol19973097059316526
- JenkinsDPBaxterGFYellonDMThe pathophysiology of ischemic preconditioningPharmacol Res1995843506
- JenkinsDPPugsleyWBAlkhulaifiAMIschemic preconditioning reduces troponin T release in patients undergoing coronary artery bypass surgeryHeart199777314189155608
- KurzelewskiMCzarnowskaEMaczewskiMEffect of ischemic preconditioning on endothelial dysfunction and granulocyte adhesion in isolated guinea-pig hearts subjected to ischemia / reperfusionJ Physiol Pharmacol1999506172810639012
- KharbandaRKPetersMWaltonBIshemic preconditioning prevents endothelial injury and systemic neutrophil activation during ischemia reperfusion in humans in vivoCirculation200110316243011273988
- KhoynezhadAJalaliZTortolaniAJApoptosis: Pathophysiology and therapeutic implications for the cardiac surgeonAnn Thorac Surg20047811091815337071
- KlonerRAMullerJDavisVEffects of previous angina pectoris in patients with first acute myocardial infarction not receiving thrombolyticsAm J Cardiol1995a75615177887389
- KlonerRAShookTPrzyklenkKPrevious angina alters in hospital outcome in TIMI 4. A clinical correlate to preconditioning?Circulation1995b9137457805217
- KobayashiYMiyazakiSMiyaoYEffect on survival of previous angina pectoris after acute myocardial infarctionAm J Cardiol199779153489185650
- LazouAIliodromitisEKCieslakDIschemic but not mechanical preconditioning attenuates ischemia/reperfusion induced myocardial apoptosis in anaesthetized rabbits: The role of Bcl-2 family proteins and ERK1/2Apoptosis200611219520417051325
- LesnefskyEJLunderganCFHodgsonJfor the IONA study groupEffect of nicorandil on coronary events in patients with stable angina: the impact of nicorandil in angina (IONA) randomized trialLancet200235912697511965271
- LiGCVasquezJAGallagherKPMyocardial protection with preconditioningCirculation199082609192372907
- LiPNijhawanDBudihardjoICytochrome c and dATP-dependent formation of Apaf-1/caspase-9 complex initiates an apoptotic protease cascadeCell199791479899390557
- LiuGSThorntonJVan WinkleDMProtection against infarction afforded by preconditioning is mediated by A1 adenosine receptors in rabbit heartCirculation19918435062060105
- LiuHMcPhersonBCYaoZPreconditioning attenuates apoptosis and necrosis: role of protein kinase Cε and -δ isoformsAm J Physiol2001281H40410
- LiuHZhangHYZhuXPreconditioning blocks cardiocyte apoptosis: role of K(ATP) channels and PKC-epsilonAm J Physiol2002282H3806
- LiuYDowneyJMIschemic preconditioning protects against infarction in rat heartAm J Physiol1992263H1107121415759
- MahaffeyKWPumaJABardagelataNAAdenosine as an adjunct to thrombolytic therapy for acute myocardial infarction: results of multicenter, randomized, placebo-controlled trial: the AMISTAD trialJ Am Coll Cardiol19993417112010577561
- MajnoGJorisIApoptosis, oncosis and necrosis: an overview of cell deathAm J Pathol19951463157856735
- ManganoDTMiaoYTudorICPost-reperfusion myocardial infarction. Long-term survival improvement using adenosine regulation with acadesineJ Am Coll Cardiol2006482061416814669
- MattsonMPKroemerGMitochondria in cell death: novel targets for neuroprotection and cardioprotectionTrends Mol Med2003919620512763524
- MaulikNEngelmanRMRousouJAIschemic preconditioning reduces apoptosis by upregulating anti-death gene Bcl-2Circulation1999100II3697510567332
- MaulikNSasakiHAddyaSRegulation of cardiomyocyte apoptosis by redox-sensitive transcription factorsFEBS Lett200048571211086156
- MurryCEJenningsRBReimerKAPreconditioning with ischemia: a delay of lethal cell injury in ischemic myocardiumCirculation1986741124363769170
- NakanuraMWangNPZhaoZQPreconditioning decreases Bax expression, PMN accumulation and apoptosis in reperfused rat heartCardiovasc Res2000456617010728387
- O’RourkeBEvidence for mitochondrial K+ channels and their role in cardioprotectionCirc Res2004944203215001541
- OkamuraTMiuraTIwamotoHIschemic preconditioning attenuates apoptosis through protein kinas C in rat heartsAm J Physiol1999277H1997200110564156
- OkuboSTanabeYTakedaKIschemic preconditioning and morphine attenuate myocardial apoptosis and infarction after ischemia-reperfusion in rabbits: role of δ-opioid receptorAm J Physiol2003287H178691
- PainTYangXCritzSDOpening of mitochondrial KATP channels triggers the preconditioned state by generating free radicalsCirc Res200087460610988237
- ParaskevaidisIAIliodromitisEKMavrogeniSRepeated exercise test identifies early and late preconditioningInt J Cardiol200598221615686771
- PatelDJPucellHJFoxKMCardioprotection by opening of the KATP channel inn unsteable angina. Is this a clinical manifestation of myocardial preconditioning? Results of a randomized study with nicorandilEur Heart J19992051710075141
- PiotCAMartiniJFBuiSKIschemic preconditioning attenuates ischemia/reperfusion-induced activation of caspases and subsequent cleavage of poly(ADP-ribose) polymerase in rat hearts in vivoCardiovasc Res1999445364210690285
- PrzyklenkKKlonerRAIschemic preconditioning: exploring the paradoxProgress Cardiovasc Dis19994051747
- PrzyklenkKIschemic preconditioningJ Thromb Thrombolysis200099910310590197
- RossAMGibbonsRJStoneGWA randomized, double-blind, placebo-controlled multicenter trial of adenosine as an adjunct to reperfusion in the treatment of acute myocardial infarction (AMISTAD-II)J Am Coll Cardiol20054517758015936605
- SarasteAPulkkiKMorphologic and biochemical hallmarks of apoptosisCardiovasc Res2000455283710728374
- SatoTSasakiNO’RourkeBNicorandil, a potent cardioprotective agent, acts by opening mitochondrial ATP-dependent potassium channelsJ Am Coll Cardiol200035514810676702
- ScarabelliTMKnightRStephanouAClinical implications of apoptosis in ischemic myocardiumCurr Probl Cardiol20063118126416503249
- SchottRJRohmannSBraunERIschemic preconditioning reduces infarct size in swine myocardiumCirc Res1990661133422317890
- SchulzRCohenMVBehrensMSignal transduction of ischemic preconditioningCardiovasc Res2001521819811684066
- SchwarzERReffelmannTKlonerRAClinical effects of ischemic preconditioningCurr Opin Cardiol199914340810448615
- SearleJKerrJFBishopCJNecrosis and apoptosis: Distinct modes of cell death with fundamentally different significancePathol Annu198217229597182752
- ShikiKHearseDJPreconditioning of ischemic myocardium: reperfusion-induced arrhythmiasAm J Physiol1987253H147063425747
- SingalPKLiTKumarDAdriamycin induced heart failure: mechanism and modulationMol Cell Biochem2000207778610888230
- TomaiFCreaFGaspardoneAEffects of A1 adenosine receptor blockade by by bamiphylline on ischemic preconditioning during coronary angioplastyEur Heart J199617846538781823
- TomaiFCreaFGaspardoneAPhentolamine prevents adaptation to ischemia during coronary angioplasty. Role of a-adrenergic receptors in ischemic preconditioningCirculation199796217179337186
- TsangAHausenloyDJMocanuMMPostconditioning: a form of “modified reperfusion” protects the myocardium by activating the phosphatidylinositol 3-kinase-Akt pathwayCirc Res200495230215242972
- ValenGThe basic biology of apoptosis and its implications for cardiac function and viabilityAnn Thorac Surg200375S6566012607708
- Van WinkleDMThorntonJDDowneyDMThe natural history of preconditioning: Cardioprotection depends on duration of transient ischemia and time to subsequent ischemiaCoron Artery Dis1991261319
- WangJLenardoMJRoles of caspases in apoptosis, development, and cytokine maturation revealed by homozygous gene deficienciesJ Cell Sci2000113753710671365
- YangXMBaxterGFHeadsRJInfarct limitation of the second window of protection in conscious rabbit modelCardiovasc Res199631777838763407
- YellonDMAlkulaifiAMPugsleyWBPreconditioning the human myocardiumLancet199334227678101304
- YellonDMBaxterGFA “second window of protection” or delayed preconditioning phenomenon: future horizons for myocardial protection?J Mol Cell Cardiol1995271023347563099
- YellonDMDowneyJMPreconditioning the myocardium: from cellular physiology to clinical cardiologyPhysiol Rev200383113351
- ZhaoZQVinten-JohansenJMyocardial apoptosis and ischemic preconditioningCardiovasc Res2002554385512160941
- ZorattiMSzab’oIThe mitochondrial permeability transitionBiochim Biophys Acta19951241139767640294
- ZouHLiYLiuXAn APAF-1. cytochrome c multimeric complex is a functional apoptosome that activates procaspase-9J Biol Chem1999274115495610206961