Abstract
Cardiovascular disease is the leading cause of death in patients with diabetes therefore prompt diagnosis and treatment of high risk groups is essential. Dobutamine stress echocardiography is a safe, cheap and reliable method for coronary artery disease diagnosis and provides important long term prognostic information. The diagnostic accuracy and prognostic power of this technique has been validated by a number of studies on patients with and without diabetes. This article discusses the application, interpretation, and accuracy of stress echocardiography both in the general population and in patients with diabetes. The role of advanced imaging modalites such as myocardial contrast agents and tissue Doppler imaging is also explored.
Introduction
Patients with diabetes mellitus have a significantly increased risk of ischemic cardiovascular mortality and morbidity.Citation1–Citation3 Diagnosis can be difficult as the symptoms are often atypical and significant obstructive coronary disease clinically silent. This is thought to be in part due to abnormal perception of angina caused by autonomic neuropathy. Dobutamine stress echocardiography (DSE) is a widely used tool for both ischemic heart disease diagnosis and risk stratification in different clinical settings. This article highlights the principles and practice of this technique and its efficacy in diabetic patients.
Pathophysiology: The ischemic cascade
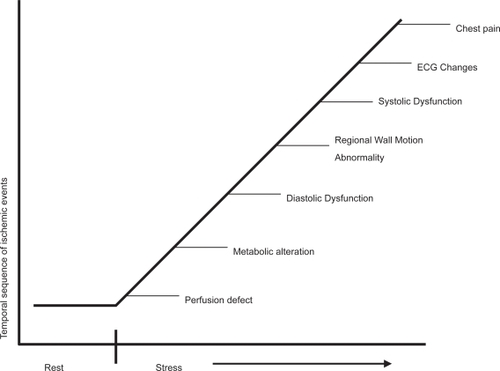
Myocardial ischemia is caused by a transient imbalance between oxygen supply and demand, the signs and symptoms of which can be used as a diagnostic tool. A typical cascade of events in a well defined time sequence will occur after the onset of ischemia.Citation4 The forerunner is abnormal myocardial perfusion and endothelial dysfunction, followed by regional wall motion dyssynergy, and only at a later stage by electrocardiography (ECG) changes and pain. DSE aims to detect regional wall motion abnormalities under ischemic conditions and thus allows diagnosis at an earlier stage of the cascade than would be achieved by symptoms or ECG changes ().
Figure 1 The ischemic cascade.
Methodology
The stress agent
Exercise, either via bicycle or treadmill, is the most attractive stress agent as it also provides important physiological data. However, this mode of stress is limited in patients unable to exercise and requires very rapid acquisition of the echo images. Consequently, pharmacological stress is often preferred. Coronary vasodilators such as adenosine and dipridamole cause a relative hyperemia with coronary steal to induce ischemia. However, they cause relatively less effects on wall motion during stress and are less accurate than inotropic agents such as dobutamine. Thus dobutamine remains the pharmacological stress agent of choice in most institutions. Pacing induces ischemia by increasing myocardial oxygen consumption (due to increased heart rate) and reducing myocardial subendocardial perfusion. However, the technique is invasive and involves atrial stimulation via the transvenous or transoesophageal route so is rarely used.
Image acquisition
Dobutamine is the most often used stress agent as discussed above. Ischemia is provoked mainly via the enhanced chronotropic and inotropic response to stimulation. Transthoracic echo images of the heart are acquired in standard parasternal long-and short-axis and apical 2-, 3-, 4-chamber views at baseline and during stepwise infusion of dobutamine. This is given according to a protocol based on 3 minute stages of 5, 10, 20, 30, 40 μg/kg/min. Atropine can be administered up to a total of 1.0 mg intravenously if the target heart rate is not achieved with dobutamine alone. Blood pressure and 12-lead ECG are recorded at baseline and at each infusion stage. Baseline, low-dose (heart 10–15 beats above baseline), peak and recovery (10 minutes after drug infusion terminated) stage images are acquired as digital loops in a quad screen format and stored for off-line analysis. The test is stopped if: target heart rate is achieved ([220–age] × 0.85), ST depression >2 mm, significant tacharrhythmia, symptomatic severe hypotension, blood pressure >240 mmHg systolic or 140 mmHg diastolic. Serious side effects are rare (1:1000 patients).Citation5 Common minor side effects include headache, nausea, shivering, urgency, hypotension. Because of the short half life of dobutamine (2 minutes,) there is rapid resolution of its effects once the infusion has been stopped.
Interpretation of stress echocardiography
Interpretation is usually by visual assessment based on analysis of thickening and inward systolic motion before, during and after stress. The heart is typically divided into a 17 segment modelCitation6 () and a score assigned to each segment at baseline and during stress based on the degree of thickening as shown in .Citation7 The presence of a new or worsening regional wall motion abnormality in 1 or more segments identifies an ischemic response. The site of this response gives a clue as to the artery affected (). The extent of ischemia is based on the number of affected segments, the occurrence of ischemia at an early stage of the test,Citation8 the wall motion score index at rest and peak stress,Citation9 and a slow recovery time.Citation10 Global left ventricular (LV) ejection fraction and end systolic volumes may also be calculated at baseline and at peak stress. A fall in either of these parameters is an indicator of significant ischemia.
Figure 2 17-segment cardiac model.
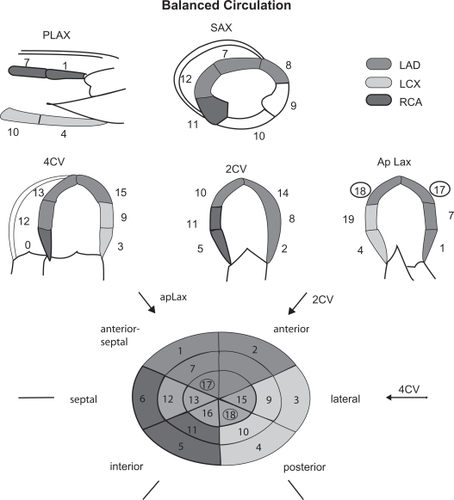
Table 1 The segmental scoring system
This qualitative approach requires significant trainingCitation11 and there are problems with reproducibility in inexperienced hands.Citation12 Five percent to 10% of patients will have poor acoustic windows such that insufficient cardiac segments can be analyzed.
Accuracy of stress echocardiography
The accuracy of this technique is consistently reported to be good with sensitivity and specificity averaging 82% and 81%, respectively.Citation13 This is comparable to perfusion imaging and superior to exercise ECG. As with other forms of stress testing, the accuracy is lower in those with single vessel disease.Citation14 Accuracy is also reduced in patients taking beta blockers although this can be overcome by administration of atropine to achieve the target heart rate. Advances in image acquisition, analysis, and interpretation have enhanced the accuracy and prognostic value of the test. Nevertheless, the technique is subjective and interinstitutional observer agreement remains suboptimal despite these advances.Citation15 In assessing the relative merits of which test to select for coronary artery disease (CAD) diagnosis in any given institution, the overriding consideration must always be local expertise.
Prognostic evaluation
A normal stress echo carries a very low risk (<1% per year) of major cardiac events in the subsequent 5 years.Citation16 A positive stress test carries a 10%–30% risk of further cardiac events, with risk being greatest in those with the highest ischemic burden.Citation17 The prognostic value of DSE is independent and additive to resting echo and exercise ECG.Citation18
Clinical application
lists the major uses of DSE in clinical cardiology. In all of the above settings the test gives diagnostic and prognostic information. A detailed account of its role in viability and valvar heart disease is outside the scope of this review article. It is being increasingly used to risk stratify patients with no cardiac symptoms awaiting high risk non cardiac surgery. This is especially true of patients awaiting major vascular surgeryCitation19 and in renal transplant candidates,Citation20 where there is a high probability of underlying CAD.
Table 2 Indications for dobutamine stress echo
New technologies in stress echocardiography
Myocardial contrast agents
Left ventricular opacification with contrast agents injected peripherally greatly enhances endocardial border definition.Citation21 This now allows an accurate diagnosis in patients previously considered not suitable for DSE due to poor image quality.Citation22 Assessment of myocardial perfusion using contrast at rest and under stress is also now possible.Citation23 This technique is promising because a perfusion abnormality would be expected to occur before a regional wall motion abnormality in the ischemic cascade However, at present its use is limited to a few centers only and further standardization of the methodology is required before the technique is established.
Coronary flow reserve
Doppler echocardiographic-derived coronary flow reserve (CFR) has been studied in diabetic and nondiabetic patients. The technique is especially reproducible for the left anterior descending artery. Using a CFR cut off value of < or = 2, CFR provides independent prognostic information in diabetic patients with CAD and a negative dipyridamole stress echocardiogram.Citation24
Tissue Doppler and strain rate imaging
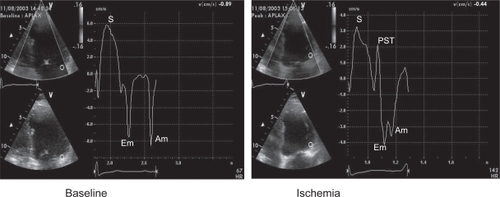
Tissue Doppler imaging allows assessment of myocardial motion in preference to blood flow. Global and regional systolic and diastolic velocities can be displayed at rest and under stress. The study can thus be quantified. During ischemia, systolic and diastolic velocities are reduced in amplitude with a delayed timing of peak contraction after aortic valve closure: post systolic thickening ().Citation25 However, this technique remains angle-dependent and velocities in a given segment of the heart are influenced by tethering to adjacent segments and rotational motion of the myocardium under stress. This problem can be overcome by assessing deformation of the myocardium between 2 segments: strain rate imaging.Citation26 While these techniques may improve the diagnostic accuracy of stress echo and reduce interobserver variability, their use requires considerable expertise and machines with high frame rates.
Figure 3 Typical regional velocity response to ischemia seen with tissue doppler imaging. In this example the basal lateral wall velocities are analyzed. At peak stress the systolic(s) and diastolic (Em and Am) are reduced. There is also a delayed contraction seen after aortic valve closure (PST).
Dobutamine stress echocardiography in diabetes
Approximately 50% of mortality in diabetic patients is related to CAD.Citation27 Risk of death from cardiovascular disease in this population is equivalent to nondiabetics after myocardial infarction.Citation28 Assessing cardiovascular risk in diabetic patients is therefore crucial. Sex, lipid levels,Citation29 resting ST segment changes are less predictive in diabetes and silent ischemia is more common.Citation30 Associated peripheral vascular disease and poor exercise capacity make standard exercise ECG testing in this group less effective. DSE is therefore an attractive method of assessing cardiovascular risk in diabetics.
Prognostic evaluation of dobutamine stress echo in diabetes
Several studies have shown stress echo is a feasible and safe in diabetic patients.Citation31–Citation34 The accuracy is the same as for nondiabetics. The presence of inducible regional wall motion abnormality under stress is an independent predictor of death, incremental to other factors, especially resting LV function.Citation32,Citation34 A negative stress echo result is associated with a higher mortality (4% per year) than a similar result in nondiabetics (1% per year). The diabetics who die despite a normal stress echo tend to be older, have poorer exercise capacity, and have poorer LV function at rest. A positive stress echo result in a diabetic is associated with a much higher annual mortality (10% per year) than a similar result in a nondiabetic (5% per year). Those with impaired LV systolic function at rest and a high ischemic burden are at greatest risk.Citation32,Citation34
A positive stress ECG is a marker of adverse outcome in asymptomatic diabetics. It is also a useful tool for identifying high cardiac risk renal transplant candidates.Citation35 In patients undergoing major vascular surgery, unrecognized myocardial infarction and silent myocardial ischemia, detected by stress echocardiography, are highly prevalent (23% and 28% respectively) and are associated with increased long term cardiovascular events.Citation36
The timing of serial stress studies in diabetic patients with an initial normal stress test is also uncertain. Elhendy and colleaguesCitation33 have suggested that the cardiac event rate is low within 2 years after a stress echo, but after this events may occur.
Other techniques for detection of coronary disease in diabetics
Nonspecific ST and T wave changes on the 12 lead ECG are strong predictors of inducible ischemia in asymptomatic diabetic patients. A high coronary calcium score (>400 Agaston units) from cardiac computed tomography (CT) is associated with a high incidence of inducible ischemia in diabetic patients.Citation37 Myocardial perfusion imaging also has excellent accuracy for CAD diagnosis and event prediction in diabetics.Citation38 A normal study is associated with a low event rate within the next 2 years. Multislice CT coronary angiography, stress magnetic resonance imaging (MRI) and MRI perfusion are emerging techniques for CAD detection, but have not been extensively investigated in the diabetic population.
Screening for cardiovascular disease in diabetes
Advocating which diabetic patients should be investigated for cardiovascular disease remains difficult. Only 5%–10% of asymptomatic diabetics will have obstructive CAD so a universal screening programme for this group cannot be justified, particularly as revascularization is associated with higher risk than in nondiabetics.Citation39,Citation40 However, certain patients may benefit such as those needing renal transplantationCitation20 or major noncardiac surgery.Citation19 In these groups coronary revascularization may reduce the procedural risk.Citation41 However, diabetics with cardiac symptoms, even if atypical, and those with known or suspected CAD warrant screening and prognostic evaluation. The presence of ischemia during stress echo, especially in those with LV dysfunction at rest, permits the identification of a high risk subgroup who should be further investigated and treated accordingly. The combination of stress echocardiography and a disease specific diabetic cardiac risk score may optimize the detection of CAD and cardiac events in asymptomatic patients.Citation42
Key messages
Cardiovascular disease is the leading cause of death in patients with diabetes.
DSE is a safe and reproducible technique for CAD diagnosis and risk stratification.
Diabetic patients with a positive stress echocardiogram, especially if baseline LV systolic function is impaired, are at high cardiovascular risk.
High risk diabetics should be referred for further cardiac investigations and potential revascularization.
Disclosure
The authors report no conflicts of interest in this work.
References
- KannelWBMcGeeDLDiabetes and cardiovascular risk factors: the Framingham studyCirculation197959813758126
- StamlerJVaccaroONeatonJDDiabetes, other risk factors, and 12-yr cardiovascular mortality for men screened in the Multiple Risk Factor Intervention TrialDiabetes Care199316434448432214
- FullerJHShipleyMJRoseGMortality from coronary heart disease and stroke in relation to degree of glycaemia: the Whitehall studyBr Med J (Clin Res Ed)198328786770
- HeyndrickxCBaicHNelkinsPDepression of regional blood flow and wall thickening after brief coronary occlusionAm J Physiol1978234H65360665778
- PicanoEMathiasWJrPingitoreASafety and tolerability of dobutamine-atropine stress echocardiography: a prospective, multicentre study. Echo Dobutamine International Cooperative Study GroupLancet1994344119027934540
- CerqueiraMDWeissmanNJDilsizianVAmerican Heart Association Writing Group on Myocardial Segmentation and Registration for Cardiac Imaging. Standardized myocardial segmentation and nomenclature for tomographic imaging of the heart. A statement for healthcare professionals from the Cardiac Imaging Committee of the Council on Clinical Cardiology of the American Heart AssociationInt J Cardiovasc Imaging2002185394212135124
- ArmstrongWFPellikkaPARyanTStress echocardiography: recommendations for performance and interpretation of stress echocardiography. Stress Echocardiography Task Force of the Nomenclature and Standards Committee of the American Society of EchocardiographyJ Am Soc Echocardiogr199811971049487482
- SegarDSBrownSESawadaSGDobutamine stress echocardiography: correlation with coronary lesion severity as determined by quantitative angiographyJ Am Coll Cardiol19921911972021564220
- GunalpBDokumaciBUyanCValue of dobutamine technetium-99m-sestamibi SPECT and echocardiography in the detection of coronary artery disease compared with coronary angiographyJ Nucl Med199334889948509853
- PicanoELattanziFDistanteARole of myocardial oxygen consumption in dipyridamole-induced ischemiaAm Heart J198911831492750652
- PicanoELattanziFOrlandiniAStress echocardiography and the human factor: the importance of being expertJ Am Coll Cardiol19911766691993786
- HoffmannRLethenHMarwickTAnalysis of interinstitutional observer agreement in interpretation of dobutamine stress echocardiogramsJ Am Coll Cardiol19962733068557902
- PicanoEBedettiGVargaAThe comparable diagnostic accuracies of dobutamine-stress and dipyridamole-stress echocardiographies: a meta-analysisCoron Artery Dis200011151910758817
- SawadaSGSegarDSRyanTEchocardiographic detection of coronary artery disease during dobutamine infusionCirculation1991831605141673646
- PellerinDBreckerSA step further in inter–institutional agreement in interpretation of dobutamine stress echocardiogramsEur Heart J2002237687112009715
- McCullyRBRogerVLMahoneyDWOutcome after normal exercise echocardiography and predictors of subsequent cardiac events: follow-up of 1,325 patientsJ Am Coll Cardiol19983114499426033
- ChuahSCPellikkaPARogerVLRole of dobutamine stress echocardiography in predicting outcome in 860 patients with known or suspected coronary artery diseaseCirculation1998971474809576428
- PingitoreAPicanoEVargaAPrognostic value of pharmacological stress echocardiography in patients with known or suspected coronary artery disease: a prospective, large-scale, multicenter, head-to-head comparison between dipyridamole and dobutamine test. Echo-Persantine International Cooperative (EPIC) and Echo-Dobutamine International Cooperative (EDIC) Study GroupsJ Am Coll Cardiol19993417697710577568
- PoldermansDArneseMFiorettiPMImproved cardiac risk stratification in major vascular surgery with dobutamine-atropine stress echocardiographyJ Am Coll Cardiol199526648537642854
- SharmaRPellerinDGazeDCDobutamine stress echocardiography and the resting but not exercise electrocardiograph predict severe coronary artery disease in renal transplant candidatesNephrol Dial Transplant20052022071416030034
- Al-MansourHAMulvaghSLPumperGMUsefulness of harmonic imaging for left ventricular opacification and endocardial border delineation by OptisonAm J Cardiol2000857959A1012000067
- DolanMSRiadKEl-ShafeiAEffect of intravenous contrast for left ventricular opacification and border definition on sensitivity and specificity of dobutamine stress echocardiography compared with coronary angiography in technically difficult patientsAm Heart J20011429081511685180
- SpencerKTGrayburnPAMor-AviVMyocardial contrast echocardiography with power Doppler imagingAm J Cardiol2000864798110946053
- CortigianiLRigoFGherardiSAdditional prognostic value of coronary flow reserve in diabetic and non diabetic patients with negative dipyridamole stress echocardiography by wall motion criteriaJ Am Coll Cardiol20075013546117903635
- CainPBaglinTCaseCApplication of tissue Doppler to interpretation of dobutamine echocardiography and comparison with quantitative coronary angiographyAm J Cardiol2001875253111230833
- JamalFKukulskiTStrotmannJQuantification of the spectrum of changes in regional myocardial function during acute ischemia in closed chest pigs: an ultrasonic strain rate and strain studyJ Am Soc Echocardiogr2001148748411547273
- FordESDeStefanoFRisk factors for mortality from all causes and from coronary heart disease among persons with diabetes. Findings from the National Health and Nutrition Examination Survey I Epidemiologic Follow-up StudyAm J Epidemiol19911331220302063830
- HaffnerSMLehtoSRönnemaaTMortality from coronary heart disease in subjects with type 2 diabetes and in nondiabetic subjects with and without prior myocardial infarctionN Engl J Med1998339229349673301
- PanWHCedresLBLiuKRelationship of clinical diabetes and asymptomatic hyperglycemia to risk of coronary heart disease mortality in men and womenAm J Epidemiol1986123504163946397
- NakaMHiramatsuKAizawaTSilent myocardial ischemia in patients with non-insulin-dependent diabetes mellitus as judged by treadmill exercise testing and coronary angiographyAm Heart J199212346531729850
- BatesJRSawadaSGSegarDSEvaluation using dobutamine stress echocardiography in patients with insulin-dependent diabetes mellitus before kidney and/or pancreas transplantationAm J Cardiol19967717598546087
- D’AndreaASeverinoSCasoPPrognostic value of pharmacological stress echocardiography in diabetic patientsEur J Echocardiogr20034202812928024
- ElhendyAArrudaAMMahoneyDWPrognostic stratification of diabetic patients by exercise echocardiographyJ Am Coll Cardiol2001371551711345364
- MarwickTHCaseCSawadaSUse of stress echocardiography to predict mortality in patients with diabetes and known or suspected coronary artery diseaseDiabetes Care2002251042812032112
- SharmaRPellerinDGazeDCDobutamine stress echocardiography and the resting but not exercise electrocardiograph predict severe coronary artery disease in renal transplant candidatesNephrol Dial Transplant20052022071416030034
- FeringaHHKaragiannisSEVidakovicRThe prevalence and prognosis of unrecognised myocardial infarction and silent myocardial ischaemia in patients undergoing major vascular surgeryCoron Artery Dis200718571617925612
- AnandDVLimEHopkinsDRisk stratification in uncomplicated type 2 diabetes: prospective evaluation of the combined use of coronary artery calcium imaging and selective myocardial perfusion scintigraphyEur Heart J2006277132116497686
- De LorenzoALimaRSSiqueira-FilhoAGPrevalence and prognostic value of perfusion defects detected by stress technetium-99m sestamibi myocardial perfusion single-photon emission computed tomography in asymptomatic patients with diabetes mellitus and no known coronary artery diseaseAm J Cardiol2002908273212372568
- MickMJPiedmonteMRArnoldAMRisk stratification for long-term outcome after elective coronary angioplasty: a multivariate analysis of 5,000 patientsJ Am Coll Cardiol19942474808006285
- BarzilayJIKronmaLRABittnerVCoronary artery disease and coronary artery bypass grafting in diabetic patients aged ≥65 years (report from the Coronary Artery Surgery Study [CASS] Registry)Am J Cardiol19947433498059694
- ManskeCLWangYRectorTCoronary revascularisation in insulin-dependent diabetic patients with chronic renal failureLancet199234099810021357450
- RakhitDJDowneyMJeffriesLScreening for coronary artery disease in patients with diabetes: a Bayesian strategy of clinical risk evaluation and exercise echocardiographyAm Heart J200515010748016291001