Abstract
Background:
Abdominal aortic aneurysm (AAA) is considered a manifestation of atherosclerosis, however there are epidemiologic, biochemical, and structural differences between occlusive atherosclerosis and AAA. The pathogenesis of AAA involves several factors, first of all destruction of collagen and elastin in the aortic wall. Classical risk factors may influence the evolution and development of AAA, though no consistent association has been found. Aims of the study were to evaluate associations between risk factors and to establish the prevalence of carotid, peripheral vascular and coronary atherosclerosis in patients with AAA.
Methods:
We studied 98 patients with AAA (Group 1) awaiting surgery compared with high cardiovascular risk population having two or more risk factors (n = 82 Group 2). We evaluated traditional risk factors and we studied by eco-doppler and echocardiography the presence of carotid peripheral and coronaric atherosclerosis in two groups.
Results:
We found a higher incidence of AAA in males (p < 0.01). The prevalence of infrarenal AAA was significantly higher than suprarenal AAA (81 vs 17 p < 0.001). No differences in total cholesterol (199 ± 20 vs. 197 ± 25 mg/dl), low-density lipoprotein (142 ± 16 vs. 140 ± 18 mg/dl), triglycerides (138 ± 45 vs. 144 ± 56 mg/dl), glycemia (119 ± 15 vs. 122 ± 20 mg/dl), and fibrinogen (388 ± 154 vs. 362 ± 92 mg/dl) were found between groups. We demonstrated significant differences for cigarette smoking (p < 0.002), systolic and diastolic blood pressure (150 ± 15 vs. 143 ± 14 mmHg and 88 ± 6 vs. 85 ± 7 mmHg, p < 0.0001 and p < 0.05, respectively) and high sensititivity C reactive protein (2.8 ± 1.3 vs. 1.3 ± 0.7 mg/dl, p < 0.001). High-density lipoprotein (HDL) cholesterol levels were significant greater in Group 1 than Group 2 (p < 0.003). Subgroups of patients with AAA and luminal thrombus showed higher fibrinogen levels (564 ± 235 vs. 341 ± 83 mg/dl, p < 0.001) and lower HDL than in controls (46.6 ± 6.5 vs. 52.1 ± 7.8 mg/dl, p < 0.01). We did not find any difference in body mass index, or prevalence of coronary and peripheral atherosclerosis between groups. Conversely, we found higher prevalence of carotid atherosclerosis in Group 2 (9% vs. 25%, p < 0.004).
Conclusion:
Our AAA patients had fewer and different risk factors respect to patients with atherosclerosis. Only elevated blood pressure, C reactive protein, and smoking showed a significant association with AAA. Atherosclerosis in other arterial districts did not differ respect to subjects with high cardiovascular risk. Our results confirm the hypothesis that AAA and atherosclerosis are two different pathological entities with different risk profiles.
Introduction
Abdominal aortic aneurysm (AAA) has high prevalence in the cardiovascular disease and it is considered a manifestation of atherosclerosis. This view has been increasingly questioned in recent years. Although many AAA are associated with conventional risk factors, a causal relation with atherosclerosis has not been confirmed. Most patients with cardiovascular disease do not develop AAA, and many AAA patients do not have peripheral carotid or coronary disease (CitationReed et al 1992).
Though atherosclerosis plays some role in the pathogenesis of AAA, additional processes respect to occlusive atherosclerosis are probably involved, as suggested by histological and macroscopic differences. In comparison to atherosclerosis, vascular tissue in AAA is characterized by high proteolytic activity and greater infiltration of inflammatory cells. Family histories of AAA indicate that genetic factors are also involved (CitationBrophy et al 1991; CitationMac Sweeney et al 1994).
Several studies have shown that AAA and atherosclerosis have got risk factors such as age, hypertension, smoking, and hypercholesterolemia (CitationVardulaki et al 2000). Others reports revealed epidemiological differences among coronary and carotid disease and AAA (CitationAlcorn et al 1996; CitationCoggon et al 1996). In line with this, many authors did not found any association with common risk factors except for smoking (CitationBlanchard et al 2000; CitationVardulaki et al 2000; CitationSingh et al 2001). However, these studies are limited by the short duration of follow-up, small sample size, different inclusion criteria, and little information on risk factors, and epidemiology (CitationLilenfeld et al 1987). Identification of risk indicators is important to improve stratification, to prevent aortic dilation, and to select appropriate medical or surgical therapy (CitationAlcorn et al 1996; CitationBengtsson et al 1996). The aims of this study were to investigate the prevalence of AAA in high cardiovascular risk patients, the prevalence of risk factors and AAA, the distribution of infrarenal/suprarenal AAA in patients awaiting surgical treatment. A further aim was to compare cardiovascular risk pattern between AAA population and asymptomatic age-matched subjects having two or more high cardiovascular risk factors.
Materials and methods
A case-control study was performed at Siena University Hospital between June 2003 and December 2006. We recruited 98 patients with AAA (group 1) and 82 control subjects (group 2). The two groups were matched for age, race, and sex. All patients underwent cardiologic examination with electrocardiogram, weight and height measurement, X-ray, and routine blood chemistry including glucose, low-density lipoprotein (LDL) and high-density lipoprotein (HDL) cholesterol, liver and renal function parameters, electrolytes, fibrinogen, hemochrome, and high sensitivity C-reactive protein (hsCRP). They underwent ultrasonographic examination of the abdominal, peripheral, and carotid arterial segments. To assess coronary disease subjects underwent echocardiography stress examination with dipyridamol (CitationPicano 2004) Patients with AAA also underwent computed tomography (CT) examination to assess intraluminal thrombosis and aortic transverse diameter.
Biochemical laboratory assessment
All blood samples were taken after a minimum 4-hour fast. Venous blood was taken in ethylenediaminetetraacetic acid (EDTA) tubes. The plasma samples were snap-frozen within 1 hour to –20° C and stored at –80° C within a week. All EDTA plasma for analyses were thawed and analyzed at the same time. LDL and HDL cholesterol concentrations were measured by direct, homogeneous assays based on detergent treatment of the serum (N-geneous HDL-c and N-geneous LDL reagents, respectively, from Genzyme Corp, Cambridge, MA, USA). hsCRP was measured by a latex-enhanced immunoturbidimetry assay (Tinaquant CRP [Latex] HS, Roche Diagnostics GmbH, Mannheim, Germany). Plasma fibrinogen levels was measured by the Clauss modified method with coagulomether (Behring Diagnostics, Marburg, Germany).
Cardiovascular risk factors
Body mass index (BMI) was calculated as weight divided by the square of height (kg/m2). Blood pressure was recorded during cardiological examination in a quiet room after five minutes rest in sitting position; three measures were made at 2 minute intervals (oscillometric method, Colin Meter, Germany). Hypertension was defined as systolic blood pressure 140 mmHg or higher and/or diastolic blood pressure 90 mmHg or higher in the absence of self-reported use of antihypertensive therapy, and treated hypertension was defined as self-reported physician-diagnosed hypertension under treatment.
Hyperlipidemia was defined as cholesterol total higher than 240 mg/dl; LDL cholesterol higher than 140 mg/dl, and HDL cholesterol lower than 35 mg/dl.
Diabetes mellitus was defined as nonfasting plasma glucose levels higher than 126 mg/dl or use of oral antidiabetic drug or insulin.
Smoking history was defined as greater than or equal to 100 cigarettes/year. Patients were considered to have hypertension, hypercholesterolemia, or diabetes if they had been given these diagnoses by a physician or were treated for these conditions.
Examinations
Abdominal ultrasonographic examination of the abdominal aorta was performed by two blinded physicians. Subjects lay in supine position and/or in their left side if necessary. A 3.5 MHz sector probe (5500 SONOS Hewlett-Packard) was used. The abdominal aorta was first visualized in the longitudinal plane from the diaphragm to the iliac bifurcation. The aorta was studied in the axial plane with scans perpendicular to the previous ones. Longitudinal and transverse aortic diameter was measured at the renal arteries, 5 cm distally, and at the bifurcation. Transverse wall thickness and endoluminal diameter were measured. In the case of AAA with mural thrombus true and false lumen diameter were also measured. All AAA patients were also submitted to abdominal CT to evaluate vessel lumen and parietal thining.
Echocardiographic examination was performed under baseline conditions and during infusion of dipyridamol, atropine according to American Society of Echocardiography criteria (CitationSchiller et al 1989). Stress echocardiography was performed by dypiridamol and atropine infusion at standard doses with electrocardiogram (ECG) recording; it was stopped if clinical, echographic, or electrocardiographic alterations occurred. All scans were evaluated in apical, four and two chambers, and longitudinal and short parasternal views by two experienced physicians.
The vascular and carotid ultrasonographic examinations were performed using either an ATL HDI 3000 or 5000 (Philips Medical Systems, Monza, Italy). Information obtained from color-flow/B-mode imaging and Doppler spectral waveform analysis from the distal aorta to the pedal arteries was used to draw a schematic color-coded map of the arterial tree. The arteries were scanned in cross and longitudinal sections using scanheads of 3–2, 5–2, 7–4, and 10–5 MHz extended operating frequency range. The arterial segments evaluated were classified as normal or mildly diseased (less than 50% narrowing), significantly stenosed (greater than 50%), occluded, or not visualized. Focal stenosis was graded based on B-mode imaging of the plaque and residual lumen in cross section, whenever applicable, presence of color flow disturbances, and velocity spectral waveform analysis. A peak systolic velocity (PSV) ratio greater than 2 was used to tell hemodynamically significant (>50%) from hemo-dynamically insignificant stenosis. Long arterial narrowing (residual lumen <50% of the actual artery diameter) in diffusely diseased arterial segments was also observed based on B-mode/color-flow imaging. Presence of intraluminal echoes and absence of color flow confirmed artery occlusion. Iliac disease was assessed by direct ultrasonographic visualization and by observation of common femoral artery (CFA) waveform abnormalities in the spectral window, number of phases, and acceleration time (>140 ms considered abnormal). For the scanning protocol, the test starts with femoral arteries scanning and is followed by the popliteal artery examination. The popliteal artery is scanned both from the medial and posterior approaches. The tibioperoneal trunk, peroneal, and anterior tibial arteries are examined in lateral decubitus. The aorta, iliac, posterior tibial, dorsalis pedis, and common plantar arteries are scanned after returning the patient to the supine position.
B-mode real-time ultrasound was performed in blind, evaluating the arterial stenosis in the carotid arteries with a probe of 7.5–10.0 MHz. Patients were examined in the supine position and each carotid wall or segment was examined. Each scan of the common carotid artery began just above the clavicle, and the transducer was moved until the carotid bifurcation and along the internal carotid artery. Three segments were identified and measured in antero and posterior planes on each side: the distal 1.0 cm of the common carotid proximal to the bifurcation, the bifurcation itself, and the proximal 1.0 cm of the internal carotid artery. At each of these sites we detected any possible plaque. Carotid lesions were considered pathological if they were higher than 50% of the vascular lumen or have peak velocity more than 100 cm/sec. Intra-observer coefficience of variance was 5% and inter-observer coefficience of variance was 10%.
Inclusion criteria
AAA subjects were enrolled if they had transverse aortic dilation >4.5 cm and no history of cardiovascular disease. All were elegible for surgery due to aneurysm dimensions. This group also underwent computed tomography. The control group consisted of age-matched subjects referred to the Cardiology Laboratory of our Department with at least two risk factors but without clinical evidence of atherosclerosis diseases such as coronary heart disease, peripheral arterial disease. Subjects gave written informed consent and the study was approved by the Ethical Committee.
Exclusion criteria
Patients with previous vascular or cardiac events such as myocardial infarction, angina, claudicatio intermittens or stroke, aortic dissection or dissecting aneurysm were excluded. Subjects with neoplastic, immunological, liver, or kidney disease were also excluded. Patients with Marfan syndrome were excluded.
Results
Of the 98 patients in group 1, 76 were males and 22 females. Of these patients, 81 had infrarenal and 17 suprarenal AAA (p < 0.001). 45% had endoluminal thrombus. Mean transverse diameter of aneurysms was 5.4 cm (4.8 for suprarenal and 5.9 for infrarenal) (). Of the 82 patients in group 2, 50 were males and 32 females (mean age in both group 74 ± 8, range 62 to 87 years).
Table 1 Clinical and structural characteristics of patients with abdominal aortic aneurysm (AAA) and controls
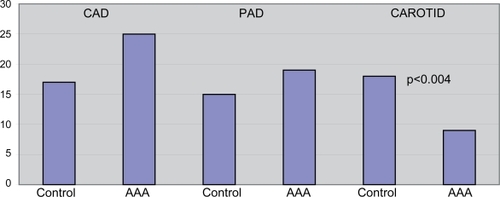
The frequency of peripheral vasculature disease was similar in the two groups: 15 (19%) controls and 19 (20%) AAA patients.
The incidence of coronary disease evaluated by stress-echo test was similar in both groups: 17 (23%) in controls, 25 (26%) in AAA patients (NS). Patients with AAA showed less evidence of carotid atherosclerosis than controls: Group 1 9 patients (9%), 18 controls (25%), (p < 0.004) (). Two patients in the control group had recruited AAA (mean diameter infrarenal 4.5 cm).
Figure 1 Prevalence of carotid disease (CAROTID), peripheral arterial disease (PAD), and coronary artery disease (CAD) in the two groups.
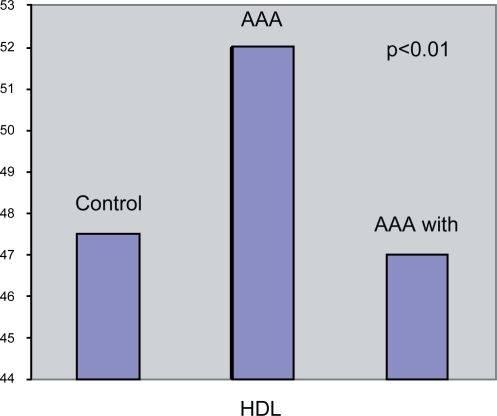
No significant differences in BMI was found, both groups showing high frequency of first degree obesity (Controls 28 ± 3.6, Group 1 29 ± 3.8 kg/m2). The percentage of patients with cholesterol over 200 mg/dl was 33% in Group 1 and 35% in controls (199 ± 20 and 197 ± 25 mg/dl, respectively NS). Likewise no differences were found for LDL cholesterol (Group 1 142 ± 16 vs. Group 2 140 ± 18 mg/dl NS), or blood glucose (Group 1 119 ± 15 vs. Group 2 122 ± 20 mg/dl NS). Significant differences regarding hsCPR were found: Group 1 2.8 ± 1.3 vs. Group 2 1.3 ± 0.7 mg/dl (p < 0.001).Triglyceride levels were not significantly different in the two groups (Group 1 138 ± 45 vs. Group 2 144 ± 56 mg/dl NS). HDL cholesterol levels were significantly greater in Group 1 than in controls (Group 1 52.1 ± 7.8 vs. Group 2 47.5 ± 6.5 mg/dl, p < 0.003). On the contrary HDL level was significantly less in AAA subgroup associated with wall thrombosis than in AAA without thrombosis (46.6 ± 6.5 vs. 52.1 ± 7.8 mg/dl, p < 0.01) ().
Figure 2 HDL cholesterol difference in AAA with and without thrombus and in controls.
Significant differences in systolic and diastolic blood pressure were found: Group 1 150 ± 15 vs. Group 2 143 ± 14 mmHg (p < 0.001) and Group 1 88 ± 6 vs. Group 2 85 ± 7 mmHg (p < 0.05). When patients were divided into two groups according to blood pressure cut-off of 140/90 mmHg, 42% of controls and 71% of AAA patients had hypertension (p < 0.0006). Past or present cigarette smoking was more frequent in AAA patients: Group 1 59(66%) Group 2 31 (40%) (p < 0.002) ().
Table 2 Association between classical risk factors in abdominal aortic aneurysm (AAA) subjects and in controls with two or more risk factors
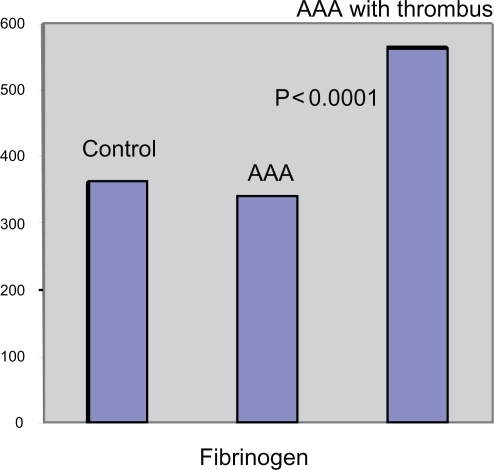
Fibrinogen levels was similar in both groups (Group 1 388 ± 154, Group 2 362 ± 92 mg/dl, NS). When Group 1 was divided into two subgroups, with wall thrombosis (n = 46) and without, the thrombosis subgroup demonstrated higher fibrinogen levels (564 ± 235 vs. 341 ± 83 mg/dl, p < 0.0001) ().
Figure 3 Different levels of fibrinogen in AAA with and without thrombus and in controls.
Discussion
Occlusive vascular disease and AAA are considered manifestations of the same atherosclerotic process, however there are many differences in pathophysiology and morphology between the two diseases (CitationLouwrens et al 1993; CitationPatel et al 1995). Traditionally, atherosclerosis is characterized by increase in plaque volume due to growth of the lipid core into the vessel lumen and migration of smooth muscle cells and macrophages, leading to endothelial dysfunction, increase in intima-media thickness, and wall thickness. On the other hand, aneurysm involves dilation of all layers of the artery wall: parietal deterioration is due to loss of elastin and smooth muscle cells. Biochemical studies of possible genetic causes have focused on structural defects in aorta matrix proteins, overactive proteolysis and impaired homeostasis of collagen (CitationCannon and Read 1982; CitationBrophy et al 1991; CitationCohen et al 1992). CitationSteinberg and colleagues (2000) recently demonstrated different inflammatory responses in the two diseases with elevated cytokine levels in AAA. There have been large prospective studies about the relationships between cardiovascular disease risk factors and AAA, and most of them are limited by small statistical samples, short follow-up, different inclusion criteria, and different definitions of AAA (CitationLilienfeld et al 1987; CitationBlanchard et al 2000; CitationSingh et al 2001). All these problems could explain the different results reported by observational studies. Several population-based studies have established male gender, age, smoking, and a family history of AAA as independent risk factors for AAA (CitationLouwrens et al 1993; CitationBlanchard et al 2000; CitationJamrozik et al 2000; CitationSingh et al 2001). Although several studies revealed a strong association between AAA and atherosclerotic diseases (CitationSimoni et al 1995; CitationBlanchard et al 2000; CitationJamrozik et al 2000; CitationSingh et al 2001), reports on possible associations between AAA and established risk factors for atherosclerosis such as hypercholesterolemia and hypertension have shown different results (CitationPatel et al 1995; CitationSimoni et al 1995; CitationJamrozik et al 2000; CitationSingh et al 2001). Histological and epidemiological differences between AAA and atherosclerosis have further challenged the traditional theory that AAA is a manifestation of atherosclerosis (CitationLilienfeld et al 1987; CitationLouwrens et al 1993; CitationSatta et al 1998; CitationSingh et al 2001).
Data in the literature regarding the relationship between AAA and cholesterol levels are contradictory. In a large screening study, the ADAM study (CitationLederle et al 2000), high cholesterol levels were independently associated with AAA in a multivariate analysis including atherosclerosis. CitationSimoni and colleagues (1995) showed a relationship between lower HDL cholesterol levels and AAA, but no difference was observed in LDL cholesterol or total cholesterol levels. In the Tromso study, a highly significant relation between low HDL cholesterol and the risk of AAA was found (CitationSingh et al 2001). We did not show a significant association with serum lipids (LDL cholesterol and triglycerides), which may be due to the high risk comparison group: indeed, we analyzed AAA in a late stage when alterations in serum lipids could not be directly involved in the pathogenesis (CitationLee et al 1997). Curiously, low HDL levels were significantly associated to thrombotic aneurysms, probably due to elevated lipoprotein consumption and turnover. Our findings appear in accordance with CitationSimoni and colleagues (1995) and ADAM study data, which reveals an association with HDL cholesterol. Patients with AAA and parietal thrombus also had high fibrinogen levels in respect to controls groups. Both findings may explain at least in part the pathophysiological mechanism: fibrin binds to lipoproteins and sequesters more fibrinogen in the vascular intima, enhancing their accumulation. Fibrinogen is also an essential component of platelet aggregation, increasing plasma viscosity, and it is correlated with fibrin levels in clots (CitationHeinrich and Assmann 1995).Many studies found hypertension to be associated with AAA (CitationJamrozik et al 2000; CitationVardulaki et al 2000). In line with this data, we found a correlation with both elevated diastolic and systolic blood pressure. The mechanism leading to the development of aortic enlargement is related to increased wall tension according to Laplace’s law. Hypertension increases wall stress, altering elastin and collagen, causing wall thickening, and precipitating aneurysm formation (CitationNaydeck et al 1999; CitationRodin et al 2003).
Smoking has consistently been associated with AAA (CitationLee et al 1997; CitationJamrozik et al 2000; CitationLederle et al 2000; CitationTörnwall et al 2001) and several studies have found a dose-response relationship suggesting a causal role for smoking in the etiology of AAA. Smoking per se promotes atherosclerosis, and may also upset protease/antiprotease balance and occlude the vasa vasorum in this tract where the vascularization is reduced with respect to the district of the thoracic aorta (CitationCannon and Read 1982; CitationLouwrens et al 1993; CitationLee et al 1997; CitationLederle et al 2000). CitationLawlor and colleagues (2008) emphasized the role of smoking as a major risk factor for cardiovascular diseases in populations with low cholesterol levels.
HsCRP has recently emerged as a strong independent risk factor for atherosclerosis and atherosclerosis-related complications in apparently healthy individuals and patients with cardiovascular disease (CitationRidker et al 1997; Lagrand et al 1900). CitationPowell and colleagues (1987) showed that, among patients undergoing elective aortic reconstruction, serum hsCRP was elevated in AAA patients compared with patients with obstructive disease. The elevation of hsCRP was equally pronounced in small and large AAA, indicating an inflammatory process in the early pathophysiologic phase of AAA. These findings corroborate the notion that CRP up-regulation is a reaction to several types of tissue injury. Macrophages and smooth muscle cells might be the producers of ‘vascular’ CRP (CitationYasojima et al 2001).
No differences were found in carotid and peripheral atherosclerosis between groups: carotid disease seemed less frequent in the AAA group compared with the high risk group.
A similar study reveals that mean carotid intima-media thickness in AAA patients was similar to healthy subjects and significantly lower than patients affected to peripheral atherosclerosis. The findings support the notion that the formation of AAA is not fully atherosclerosis-dependent (CitationCheuk et al 2007).
These data appear consistent with those of SMART, which did not show a strict correlation between significant carotid stenosis in a large population study (CitationSimons et al 1999).
AAA patients had fewer and different risk factors respect to patients with atherosclerosis. Only elevated blood pressure and smoking showed a significant correlation with AAA. Atherosclerosis in other districts appears similar respect to high cardiovascular population.
Conclusions
In conclusion, the present study demonstrates that AAA and atherosclerosis differ in certain pathophysiological aspects and risk factors. However risk factors such as hypertension and cigarette smoking and hsCRP, could negatively promote further dilation. Cardiac, peripheral, and carotid vascular ultrasonography study demonstrated different risk profiles in the two diseases. Further studies into other potential risk factors, such as inflammation, autoimmunity, and genetics, may be warranted.
References
- AlcornHWolfsonSSutton-TyrrellK1996Risk factors for abdominal aortic aneurysms in older adults enrolled in the cardiovascular health studyArterioscler Thromb Vasc Biol16963708696960
- BengtssonHSonessonBBergqvistD1996Incidence and prevalence of abdominal aortic aneurysms, estimated by necropsy study and population screening by ultrasoundAnn NY Acad Sci800I24
- BlanchardJFArmenianHKPoulter FriesenP2000Risk factors for abdominal aortic aneurysm: result of a case-control studyAm J Epidemiol1515758310733039
- BrophyCMReillyJMSmithGJW1991The role of inflammation in non- specific abdominal aortic aneurysm diseaseAnn Vasc Surg5229332064915
- CannonDJReadRC1982Blood elastolytic activity in patients with aortic aneurysmAnn Thorac Surg3410156178380
- CheukBLLauSSChengSW2007Carotid intimamedia thickness in patients with abdominal aortic aneurysmsEur J Vasc Endovasc Surg331495317097902
- CoggonDWinterPMartynC1996Contrasting epidemiology of aortic aneurysm and peripheral vascular disease in England and WalesBMJ3129488616309
- CohenJRSarfatiIDannaD1992Smooth muscle cell elastase, atherosclerosis and abdominal aortic aneurysmsAnn Surg2163302
- HeinrichJAssmannG1995Fibrinogen and cardiovascular riskJ Cardiovasc Risk21972057584794
- JamrozikKNormanPSpencerC2000Screening for abdominal aortic aneurysm lessons from a population-based studyMJA1733455011062788
- LagrandWKVisserCAHermensWT1999C-reactive protein as a cardiovascular risk factor: more than an epiphenomenonCirculation1009610210393687
- LawlorDASongYMSungJ2008The association of smoking and cardiovascular disease in a population with low cholesterol levels. A study of 648,346 men from the Korean National Health System Prospective Cohort StudyStroke39760718239177
- LederleFJohnsonGWilsonSthe Aneurysm Detection and Management Veterans Affairs Cooperative Study Investigators2000The aneurysm detection and management study screening program. Validation cohort and final resultsArch Intern Med16014253010826454
- LeeAJFowkesFGRCarsonMN1997Smoking, atherosclerosis, and risk of abdominal aortic aneurysmEur Heart J1867169129900
- LilienfeldDEGundersonPDSprafkaJM1987Epidemiology of aortic aneurysm I. Mortality trends in the United States, 1951 to 1981Arteriosclerosis7637433689207
- LouwrensHDAdamsonJPowellJT1993Risk factors for atherosclerosis in men with stenosing and aneurysmal disease of the abdominal aortaInt Angiol122148376906
- Mac SweeneySTRPowellJTGreenhalghRM1994Pathogenesis of abdominal aortic aneurysmBr J Surg81935417922083
- NaydeckBLSutton-TyrrellKSchillerKD1999Prevalence and risk factors for abdominal aortic aneurysms in older adults with and without isolated sistolic hypertensionAm J Cardiol837596410080433
- PatelMIHardmanDTAFisherCM1995Current views on the pathogenesis of abdominal aortic aneurysmsJ Am Coll Surg185371827551334
- PicanoE2004Stress echocardiography4th EditionNew YorkSpringer13550
- PowellJTMullerBRGreenhalghRM1987Acute phase proteins in patients with abdominal aortic aneurysmsJ Cardiovasc Surg28528302443505
- ReedDReedCStemmermannG1992Are aortic aneurysms caused by atherosclerosis?Circulation85205111728451
- RidkerPMCushmanMStampferMJ1997Inflammation, aspirin, and the risk of cardiovascular disease in apparently healthy menN Engl J Med33697399077376
- RodinMBDaviglusMLWongGC2003Middle age cardiovascular risk factors and abdominal aortic aneurysm in older ageHypertension4261812796281
- SattaJLaurilaAPääkköP1998Chronic inflammation and elastin degradation in abdominal aortic aneurysm disease: an immunohistochemical and electron microscopic studyEur J Vasc Endovasc Surg15313199610343
- SchillerNBShahPNCrawfordM1989Reccomandations for quantification of the left ventricle by two-dimensional echocardiographyJ Am Soc Echocardiogr2358672698218
- SimoniGPastorinoCPerroneR1995Screening for abdominal aortic aneurysms and associated risk factors in a general populationEur J Vasc Endovasc Surg10207107655973
- SimonsPCGAlgraABotsML1999Common carotid intima-media thickness in patients with peripheral arterial disease or abdominal aortic aneurysm: the SMARTstudyAtherosclerosis146243810532680
- SinghKBonaaKJacobsenB2001Prevalence of and risk factors for abdominal aortic aneurysms in a population-based study The Tromso studyAm J Epidemiol1542364411479188
- SteinbergDHalakMShapiroS2000Abdominal aortic aneurysm and aortic occlusive disease: a comparison of risk factors and inflammatory responseEur J Vasc Endovasc Surg20462511112466
- TörnwallMVirtamoJHaukkaJ2001Life-style factors and risk for abdominal aortic aneurysm in a cohort of Finnish male smokersEpidemiology129410011138827
- VardulakiKWalkerNDayN2000Quantifying the risk of hypertension, age, sex and smoking in patients with abdominal aortic aneurysmBr J Surg8719520010671927
- YasojimaKSchwabCMcGeerEG2001Generation of C-reactive protein and complement components in atherosclerotic plaquesAm J Pathol15810395111238052