Abstract
Inhibition of dipeptidyl peptidase-4 (DPP-4) as a novel therapy for type 2 diabetes is based on prevention of the inactivation process of bioactive peptides, the most important in the context of treatment of diabetes of which is glucagon-like peptide-1(GLP-1). Most clinical experience with DPP-4 inhibition is based on vildagliptin (GalvusR, Novartis) and sitagliptin (JanuviaR, Merck). These compounds improve glycemic control both in monotherapy and in combination with other oral hyperglycemic agents. Both have also been shown to efficiently improve glycemic control when added to ongoing metformin therapy in patients with inadequate glycemic control. Under that condition, they reduce HbA1c levels by 0.65%–1.1% (baseline HbA1c 7.2–8.7%) in studies up to 52 weeks of duration in combination versus continuous therapy with metformin alone. Sitagliptin has also been examined in initial combination therapy with metformin have; HbA1c was reduced by this combination by 2.1% (baseline HbA1c 8.8%) after 24 weeks of treatment. Both fasting and prandial glucose are reduced by DPP-4 inhibition in combination with metformin in association with improvement of insulin secretion and insulin resistance and increase in concentrations of active GLP-1. The combination of DPP-4 inhibition and metformin has been shown to be highly tolerable with very low risk of hypoglycemia. Hence, DPP-4 inhibition in combination with metformin is an efficient, safland tolerable combination therapy for type 2 diabetes.
Introduction
It is known that both the level and the duration of hyperglycemia in type 2 diabetes are closely related to the risk of developing diabetic complications (CitationStratton et al 2000). Therefore, achieving glycemic control is a prerequisite for prevention of cardiovascular and microvascular complications in type 2 diabetes. Liflstyle interventions, including dietary adjustments and increased physical activity, are cornerstones of the therapy. For most patients, however, pharmacological intervention is required and present guidelines suggest metformin to be a first line treatment (Inzucchi 2000; CitationNathan et al 2006). Metformin is an inexpensive compound with documented glucose-lowering effect in both obese and non-obese subjects with type 2 diabetes (CitationInzucchi 2002; CitationHundal and Inzucchi 2003; CitationSetter et al 2003; CitationConsoli et al 2004; CitationDonnelly et al 2006). Metformin reduces glycemic levels primarily by inhibiting hepatic glucose output (CitationBailey and Turner 1996; CitationLeverve et al 2003; CitationStumvoll et al 1995). Metformin has also been shown to improve insulin sensitivity in liver and muscle (CitationGinnarelli et al 2003). Additional suggested mechanistic effects of metformin are inhibition of glucose absorption in the gut (CitationIkeda et al 2000) and increase in plasma levels of GLP-1 (CitationMannucci et al 2001). As has been reviewed (CitationBailey and Turner 1996), metformin reduces HbA1c levels in the range of 1%–1.5%, depending on the baseline HbA1c levels and the compound is well tolerated, although gastrointestinal adverse events are quite common during the initiation of the therapy. Hypoglycemia is rarely seen during metformin therapy, and the potential fatal adverse event of lactic acidosis is uncommon; nevertheless cautious should always be exercised when treating subjects with renal insufficiency with metformin.
Add-on treatment to metformin often required
In spite of the beneficial effects of metformin in improving glycemic control, very often, however, metformin alone is insufficient for achievement of good metabolic control. Often, also, glycemic control deteriorates in metformin-treated patients. This necessitates combination therapy by adding a secondary compound to metformin. Most often, sulphonylureas are added (CitationInzucchi 2002; CitationNathan et al 2006). The rationale for this combination is that sulphonylureas stimulate insulin secretion, which is a complimentary mechanism to the improvement in insulin sensitivity by metformin. Other combinations with metformin include thiazolidinediones and insulin (CitationHundal and Inzucchi 2003; CitationSetter et al 2003; CitationCharbonnel et al 2005; CitationDerosa et al 2006; CitationUmpierrez et al 2006). However, the combinations with sulphonylureas and thiazolidinediones have faced problems, in that sulphonylureas increase the risk of hypoglycemia (CitationDel Prato and Pulizzi 2006; CitationGreen and feinglos 2007) and thiazolidinediones result in weight gain and potential problems of cardiovascular adverse events and increase in the risk of bone fractures in women (CitationKahn et al 2006; CitationLevetran 2007; CitationNissen and Wolski 2007). Also the novel GLP-1 based therapy has been found to be successful in combination with metformin. This applies both to the strategy of activating the GLP-1 receptors by exenatide (CitationDeFronzo et al 2005) or liraglutide (Feinglos et al 2005), and by the strategy of preventing the inactivation of endogenous GLP-1 by inhibiting dipeptidyl peptidase-4 (DPP-4) (CitationAhrén et al 2004; CitationCharbonnel et al 2006; CitationBosi et al 2007; CitationBrazg et al 2007; CitationGoldstein et al 2007). This review summarizes the experience of combining metformin and a DPP-4 inhibitor in the treatment.
GLP-1 as a target for treatment of type 2 diabetes
The rationale for the development of DPP-4 inhibition in the treatment of type 2 diabetes relies on augmentation of the incretin effect (CitationHolst and Deacon 1998). The incretin effect is the exaggerated insulin secretion that follows oral glucose administration when compared to intravenous glucose administration and it is attributed to gut hormones augmenting glucose-stimulated insulin secretion (CitationDrucker and Nauck 2006). The two most important incretin hormones are glucose-dependent insulinotropic polypeptide (GIP) and glucagon-like peptide-1 (GLP-1) (CitationDrucker and Nauck 2006). GLP-1 is produced in L-cells, which are located mainly in the distal portion of the ileum. GLP-1 is released during meal ingestion and stimulates insulin secretion in a glucose-dependent manner (CitationDrucker and Nauck 2006). GLP-1 also inhibits glucagon secretion (CitationDunning et al 2005), delays gastric emptying (CitationNauck et al 1997) and induces satiety (CitationGutzwiller et al 1999). In addition, animal studies have presented evidence that GLP-1 increases beta cell mass by stimulating proliferation and inhibiting apoptosis (CitationPerfetti and Hui 2004), although it should be emphasized that such an effect has not been demonstrated in humans. Because all these effects would be important in the treatment of type 2 diabetes, GLP-1 has been developed as a novel therapy (CitationAhrén and Schmitz 2004). The development of GLP-1 as a therapy has, however, been complicated by its rapid inactivation, which is due to removal of the N-terminal dipeptide end through DPP-4, which inactivates GLP-1 (CitationMentlein 1999). To overcome this, two strategies have been used. One strategy is the development of GLP-1 receptor (GLP-1 mimetics such as exenatide and liraglutide), which are resistant to DPP-4 (CitationAhrén and Schmitz 2004). The other strategy is the development of inhibitors of DPP-4, which prevent the inactivation of GLP-1 and thereby enhance and prolong the action of the endogenous incretin hormone (CitationAhrén and Schmitz 2004; CitationMari et al 2005; CitationAhrén 2007a, Citation2007b). DPP-4 inhibition also prevents the inactivation of the other incretin hormone, GIP, and therefore the concentrations of the active form also of this hormone are increased during DPP-4 inhibition (CitationMari et al 2005). However, since the action of GIP to stimulate insulin secretion is almost entirely lost in type 2 diabetes (CitationVilsbøll et al 2002), this raise of GIP concentrations is of less importance.
DPP-4 inhibition as a target for treatment of type 2 diabetes
The rational of DPP-4 inhibition for the treatment of type 2 diabetes was outlined already in 1998 (CitationHolst and Deacon 1998). The first proof-of-concept study of DPP-4 inhibition showed improved metabolic control with reduced fasting and prandial glucose levels and reduction of HbA1c after 4 weeks of treatment of the DPP-4 inhibitor, NVP-DPP728 (CitationAhrén et al 2002). Improved glycemic control by DPP-4 inhibition has been confirmed in many studies with other compounds and today several DPP-4 inhibitors are in the progress of development (CitationAhrén 2007a, Citation2007b). Most experience exists for vildagliptin (LAF237, GalvusR, Novartis) and (MK-0431, JanuviaR, Merck), which are orally active compounds, which efficiently inhibit DPP-4 activity (CitationAhrén 2006; CitationKim et al 2005). Both compounds inhibit plasma DPP-4 activity for more than 16 hours after a single administration and are therefore both possible to administer once daily. Furthermore, they have both been shown to improve glycemic control when used in monotherapy as well as in combination therapy with metformin and thiazodilidinedione (CitationAhrén 2006; CitationDeacon 2007; CitationGallwitz 2007). Sitagliptin has been approved for treatment of type 2 diabetes in the US and in Europe in combination with metformin and vildagliptin has been approved for treatment of type 2 diabetes in Europe. Of particular importance is that DPP-4 inhibitors are safeand tolerable and that this in combination with their efficiency allow them to be used in early stages of the disease. One such early indication would be to use DPP-4 inhibitors in combination with metformin.
Rationale for combining metformin with DPP-4 inhibition
Type 2 diabetes develops when insulin secretion is insufficiently raised to match insulin resistance (CitationKahn 2001; CitationDeFronzo 2004). In addition, glucagon levels are inappropriately elevated, which enhances hepatic glucose output and increases fasting glucose (CitationDunning et al 2005). Therefore, diabetes is a disease with at least three main defects, which need to be corrected: impaired insulin secretion, insulin resistance and hypersecretion of glucagon. The rationale for combining metformin with DPP-4 inhibitors is the complimentary mechanism of action of the two strategies. Thus, metformin acts primarily by reducing hepatic glucose output and improving insulin sensitivity in liver and muscle (CitationStumvoll et al 1995; CitationBailey and Turner 1996; CitationHundal and Inzucchi 2003; CitationLeverve et al 2003; CitationSetter 2003) whereas DPP-4 inhibitors act by increasing GLP-1 levels and thereby stimulating insulin secretion and inhibiting glucagon secretion (CitationAhrén 2007a; CitationAhrén 2007b). The two strategies therefore have the potential to improve different mechanisms, which are defective in type 2 diabetes and therefore an additive or synergistic action when used in combination is anticipated. In addition, metformin has been shown to increase GLP-1 levels (CitationMannucci et al 2001), which would be a potential for an additional synergistic action with DPP-4 inhibitors. The mechanism underlying the increase in GLP-1 levels by metformin remains to be finally established; it has been suggested to be caused by inhibition of DPP-4 (CitationLindsay et al 2005; CitationMannucci et al 2001), although there are also findings that metformin does not affect DPP-4 activity (CitationHinke et al 2002). Instead, more recent findings suggest that metformin stimulates the secretion of GLP-1 from the gut (CitationMigoya et al 2007). Hence, from a mechanistic point of view, there is a clear rationale for combining metformin with DPP-4 inhibitors. Another important information is that the pharmacokinetics of metformin and a DPP-4 inhibitor do not change by combining the two, as shown for sitagliptin, which further indicates the feasibility of the combination (CitationHerman et al 2006).
Vildagliptin and sitagliptin as monotherapy
Both vildagliptin and sitagliptin reduce fasting and prandial glucose as well as HbA1c when used in monotherapy for the treatment of type 2 diabetes; HbA1c has been shown to be reduced by these compounds by 0.65%–1.1% after study periods of 3–12 months from baseline levels of 7.2%–8.7% (CitationAhrén et al 2004b; CitationRistic et al 2005; CitationAschner et al 2006; CitationPratley et al 2006; CitationRaz et al 2006; CitationRosenstock et al 2007; CitationSchweizer et al 2007; CitationScott et al 2007). Furthermore, these studies have shown that both vildagliptin and sitagliptin are safeand tolerable with incidences of adverse events not different from what is seen after placebo treatment and that there is a very low rate of hypoglycemia during the treatment with the DPP-4 inhibitors. Recent reviews have summarized these monotherapy studies in more detail (CitationAhrén 2007a, Citation2007b).
DPP-4 inhibition as add-on therapy to metformin
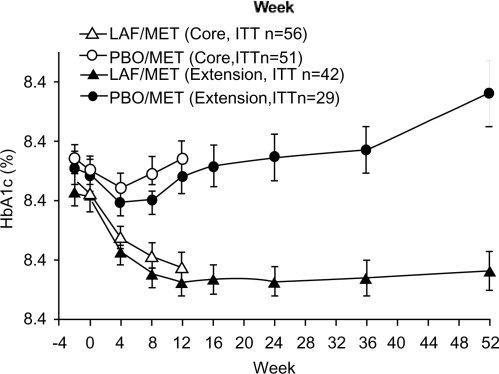
Several studies have reported the experience of treatment with a DPP-4 inhibitor in combination with metformin. The first combination study was a 52 week trial, in which vildagliptin at 50 mg daily or placebo was added to ongoing treatment with metformin (1.5–3 g daily) in patients with a mean baseline HbA1c of 7.8% (CitationAhrén et al 2004a). The patients had a mean diabetes duration of 5.5 years and they had been on metformin treatment for 29 months as a mean. The results are illustrated in and show that following the initial 12 week study period, HbA1c was reduced by 0.7% by vildagliptin in combination with metformin compared to metformin alone. After the first 12 weeks of study, patients were followed for another 40 weeks. During this period, HbA1c increased by 0.066%/month in patients given metformin alone versus only by 0.013%/month after vildagliptin plus metformin. The between-group difference in change of HbA1c after 52 week of treatment was 1.1%, showing a clinically important improvement of the glycemic control by adding vildagliptin to metformin. Furthermore, fasting glucose was also reduced by vildagliptin in combination with metformin compared to metformin alone. Thus, from a mean baseline fasting glucose of 9.8 mmol/l across all patients, the between-group difference in fasting glucose after 52 weeks of treatment was 1.1 mmol/l. The study therefore suggests that addition of vildagliptin to metformin prevents the deterioration of glycemic control seen in these patients when given metformin alone. The study also shows that the combination of vildagliptin and metformin is safeand highly tolerable with an overall incidence of any adverse event being similar in the two groups.
Figure 1 Time course of HbA1c in a 12 week core study and a 40 week extension study when vildagliptin (LAF; 50 mg once daily) was given as add-on to metformin (MET). PBO = placebo. Reproduced from CitationAhrén et al 2004a after permission from the American Diabetes Association.
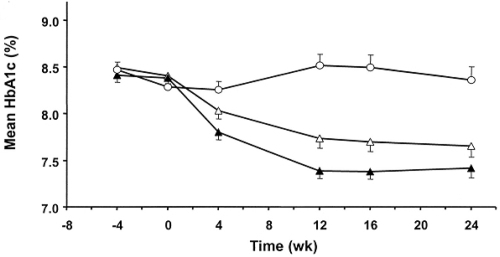
A second study in 416 patients added vildagliptin at 50 mg once or twice daily to on-going treatment with metformin for a study period of 24 weeks (CitationBosi et al 2007). The patients in this study had a mean diabetes duration of 6 years and had been treated with metformin for a mean of 16 months, their mean daily metformin dose was 2.1 g (inclusion criteria >1.5 g daily). They had a mean baseline HbA1c was 8.4%. shows the HbA1c levels in this study. It is seen that HbA1c was reduced by 0.5% in patients given vildagliptin at 50 mg daily and 0.9% in patients given vildagliptin at 100 mg daily, both in combination with metformin, versus an increase by 0.2% in patients given placebo with on-going metformin. The placebo-adjusted mean reduction in HbA1c was therefore 0.7% by vildagliptin at 50 mg and 1.1% by vildagliptin at 100 mg daily. The data were also analysed with respect to how many patients who experienced improved glycemic control or had a deterioration of glycemic control. The analysis revealed that in the group given metformin alone, 35% of patients had a deterioration of glycemic control and 31% had no meaningful change in glycemic control. In contrast, of the patients given vildagliptin at 50 mg in combination with metformin, 38% showed a meaningful improvement in glycemic control and 29% had a marked improvement in glycemic (defined as reduction in HbA1c by more than 1%). Also fasting plasma glucose was reduced by vildagliptin in combination with metformin. Baseline fasting glucose was 9.7 mmol/l across all groups. In the group given metformin alone, fasting glucose increased by 0.7 mmol/l and the placebo-adjusted reduction in fasting glucose was 0.8 mmol/l in subjects given vildagliptin at 50 mg daily and 1.7 mmol/l in subjects given vildagliptin at 100 mg in combination with metformin. Except for fasting triglycerides, lipid values were not significantly altered in any of the groups. However, fasting triglycerides increased from a mean value of 2.3 mmol/l by 19% in subjects given metformin alone but only by 1% in subjects given vildagliptin at 50 mg in combination with metformin and by 5% in the group given vildagliptin at 100 mg in combination with metformin. Mean body weight was 94 kg as a mean across all study groups and did not change significantly in the subjects given vildagliptin at either 50 or 100 mg daily in combination with metformin, whereas body weight was reduced by 1.0 kg in subjects given metformin alone. finally, total number of adverse events was not significantly different between the groups; the only difference was a reduction in gastrointestinal adverse events in the subjects given vildagliptin at 50 mg in combination with metformin (9.6%) versus in those given metformin (18.2%). In conclusion, this large study showed that vildagliptin is well tolerated when given as add-on to metformin for a study period of 24 weeks and that vildagliptin shows a clinically meaningful improvement in glycemic control as verified by dose-related reductions in HbA1c and fasting glucose.
Figure 2 Time course of mean HbA1c levels during 24 week treatment with vildagliptin at 50 mg daily (Δ) or 100 mg daily (▲) or placebo (○) in patients with type 2 diabetes continuing stable metformin treatment (≥1.5 g daily). Reproduced from Bosi et al 2007 after permission from the American Diabetes Association.
The first study on the effect of sitagliptin as add-on therapy to patients with inadequate glycaemic control on metformin monotherapy was a four week study in 28 patients (CitationBrazg et al 2007). The patients had a mean duration of diabetes of 6.6 years, the mean baseline HbA1c was 7.7% and the mean fasting plasma glucose was 8.4 mmol/l. The study showed that fasting glucose was reduced by 1.3 mmo/l by sitagliptin in combination with metformin versus only by 0.4 mmol/l by metformin alone. The study also included a 24 hr measurement of glucose after the four week treatment period, and this showed a reduction of glucose by approximately 1–1.5 mmol/l throughout the entire 24 h period. Both fasting and prandial glycemia were reduced by this degree. Furthermore, the number of adverse events was not different when sitagliptin was given in combination with metformin versus when metformin was given alone. Hence, this short-term study verified the efficient improvement in glycemic control by the addition of DPP-4 inhibition to on-going metformin therapy in association with safety and tolerability of the combination therapy.
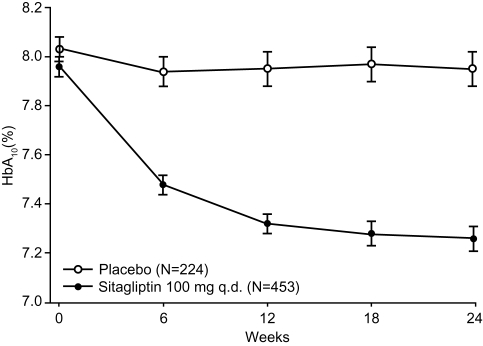
In a long-term study on the effect of sitagliptin as add-on to metformin in subjects with inadequate glycemic control, sitagliptin (100 mg once daily) was added to metformin (>1.5 g daily) for 24 weeks (CitationCharbonnel et al 2006). The study comprised a total of 701 patients who had a mean diabetes duration of 6.2 years, a mean baseline HbA1c of 8.0% and a mean baseline fasting glucose of 9.5 mmol/l. shows the HbA1c in this study. It is seen that addition of sitagliptin significantly reduced the HbA1c levels after the 24 week treatment period. The placebo-subtracted reduction in HbA1c by sitagliptin was 0.65%. A total of 47% of the patients treated with sitagliptin in combination with metformin reached the target of <7% in HbA1c while the target was reached by only 18% of the subjects given metformin alone. Also fasting glucose was reduced by sitagliptin in combination with metformin versus metformin alone; the placebo-subtracted reduction by sitagliptin was 1.4 mmol/l. The study also showed that sitagliptin in combination with metformin slightly, although significantly, reduced total cholesterol and triglycerides, whereas HDL-cholesterol was slightly increased. Body weight was slightly reduced in both groups, with no difference between the groups, and, similarly, the degree of adverse events did not differ between the groups. Hence, this 24 week trial in a large number of patients showed that sitagliptin when added to on-going therapy with metformin efficiently reduces HbA1c and fasting glucose in combination of being a safeand highly tolerable combination therapy. Following the end of the 24 week trial, patients who did not receive glycemic rescue medication continued to an extension study. During this extension, 387 patients continued with the combination of sitagliptin with metformin throughout a 54 week study period. It was found that the mean HbA1c remained stable at 7.1% during this entire period and, furthermore, the combination was well tolerated during the period (CitationKarasik et al 2007). Hence, combination of sitagliptin and metformin produced a durable reduction in HbA1c.
Figure 3 Time course of mean HbA1c levels during 24 week treatment with sitagliptin (100 mg once daily; ●) or placebo (○) in patients with type 2 diabetes with on-going treatment with (≥1.5 g daily). Reproduced from Charbonnel et al 2006 after permission from the American Diabetes Association.
Another study with sitagliptin the addition of the compound (100 mg once daily) with that of glipizide (dose-titration to a maximal doe of 20 mg daily) to the on-going treatment with metformin (>1.5 g daily) in a 52 week study comprising a total of 1,172 patients (CitationNauck et al 2007). The mean baseline HbA1c levels was 7.5% and this was reduced by 0.67% both by sitagliptin and by glipizide. The occurrence of hypoglycemia was higher in the group given glipizide (32% of patients exhibited one episode of hypoglycemia) than in the group receiving (5%). Furthermore, the mean body weight increased by 1.1 kg in the group given glimepiride versus a reduction by 1.5 kg in the group given sitagliptin. Hence, also this study showed a good improvement in glycemic control by the combination of a DPP-4 inhibitor with metformin.
Recently, it was also reported that the DPP-4 inhibitor, (Bristol-Myers-Squibb), improved glycemic control when added to metformin (CitationDeFronzo et al 2007). The study comprised a total of 743 patients with a mean HbA1c of 8.0% and a mean fasting glucose of 9.8 mmol/l when treated with metformin alone. Saxagliptin was added at 2.5, 5 or 10 mg daily and the study also included a placebo arm; all patients continued with metformin. It was found that after 24 weeks of treatment, saxagliptin had reduced HbA1c by 0.7 or 0.8% when adjusted for placebo in the three arms. Fasting glucose was reduced by 0.9–1.1 mmol/l. As for the other DPP-4 inhibitors, also saxagliptin was safeand tolerable and body weight neutral when added to metformin.
The studies thus presented sofar with DPP-4 inhibitors as add-on therapy to metformin show clinically important improvement in glycemic control. Mean HbA1c levels are reduced by approximately 0.65%–1% from a baseline of 7.8%–8.4%. Furthermore, the combination is tolerable and safewith similar adverse events profile as placebo-treated patients given metformin alone.
DPP-4 inhibition and metformin as initial combination therapy
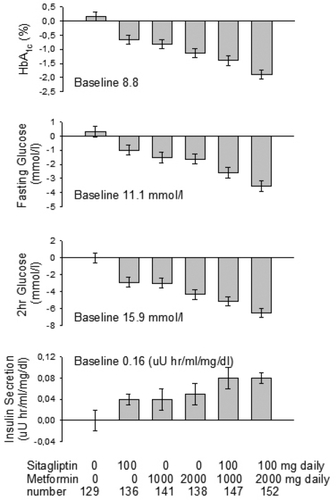
During recent years there has been a discussion of introducing initial combination therapy when pharmacological treatment is required for type 2 diabetes, in order to reach therapeutic goal at an earlier stage and to avoid or delay subsequent changes in therapy for the maintenance of therapeutic goal. One study has examined the possibility of combining DPP-4 inhibition with metformin as initial combination (CitationGoldstein et al 2007). The study was a 24-week randomized trial comprising 1,092 patients with type 2 diabetes having a mean baseline HbA1c value of 8.7% and a mean baseline fasting glucose of 11 mmol/l. The patients were assigned to one of six treatment arms with sitagliptin 50 mg + metformin 500 mg twice daily, sitagliptin 50 mg + metformin 1000 mg twice daily, metformin alone at 500 or 1000 twice daily, sitagliptin alone at 100 mg once daily or placebo. The results showed that in all treatment groups, except the placebo group, a significant reduction in HbA1c after the 24 week trial period occurred. The placebo-controlled reduction of HbA1c was in the range of 0.8%–2.1% in the different (), and when comparing monotherapy versus the initial combination therapy, it was found that combination therapy produced additive effects of improved glycemic control. Hence, the largest reduction in HbA1c (2.1%) was seen in the group given sitagliptin 50 mg + metformin 1000 mg twice daily. Similarly, fasting glucose was additively reduced by the combination therapy, and the placebo-adjusted reduction in fasting glucose in the group given sitagliptin 50 mg + metformin 1000 mg twice daily was 3.8 mmol/l. The percentage of subjects in each group who reached the treatment target of HbA1c <7.0% was 66% in the group given sitagliptin 50 mg + metformin 1000 mg twice daily versus only 38% in the group given metformin at 1000 mg twice daily alone or 20% in the group given sitagliptin at 100 mg daily alone and only 9% in the placebo group. Hence, the initial combination of sitagliptin and metformin efficiently improved glycemic control over a 24 week study period. The number of adverse events was low and the incidences of gastrointestinal adverse events were similar when sitagliptin was added to metformin as when metformin was given alone. Furthermore, the incidence of hypoglycemia was low (0.5%–2.2% in the different actively treated groups) and not significantly different from the placebo (0.6%). finally, in regard to body weight, there was a significant reduction in body weight after 24 weeks of treatment in all actively treated groups (0.6–1.3 kg) except in the group given sitagliptin alone as monotherapy.
Figure 4 Changes in HbA1c, fasting and 2 h prandial glucose and insulin secretion (as determined by 2 hr AUCinsulin divided by AUCglucose after a meal tolerance test) after 24 weeks treatment of sitagliptin and/or metformin, as indicated in bottom. Results reported are adjusted for changes after treatment with placebo. fig. is drawn after results reported in CitationGoldstein et al 2007.
Mechanisms of improved antidiabetic action by combining DPP-4 inhibitors with metformin
DPP-4 inhibitors have been shown to increase GLP-1 levels both under fasting conditions and following meal ingestion (CitationAhrén et al 2004b; CitationMari et al 2005). Furthermore, DPP-4 inhibition improves islet function by stimulating insulin secretion, by improving the glucose sensitivity of the beta cells, and by inhibiting glucagon secretion from the alpha cells (CitationBalas et al 2007; CitationDunning et al 2005). This reduces both fasting and prandial glucose which reduces HbA1c levels. In contrast to GLP-1, DPP-4 inhibition does not seem to inhibit gastric emptying (CitationVella et al 2007) and it does not reduce body weight (CitationAhrén et al 2004b; CitationAschner et al 2006; CitationPratley et al 2006; CitationRaz et al 2006; CitationRistic et al 2005; CitationRosenstock et al 2007; CitationSchweizer et al 2007; CitationScott et al 2007). Metformin, on the other hand, reduces hepatic glucose production and improves insulin sensitivity in muscle and liver cells, which improve overall insulin action and reduce mainly fasting glucose (CitationBailey and Turner 1996; Consoli et al 2994; CitationDonnelly et al 2006; CitationHundal and Inzucchi 2003; CitationLeverve et al 2003; CitationStumvoll et al 1995). The efficient improved glycemic control by combing DPP-4 inhibitors with metformin would rely on the complementary mechanism of the two treatments. It has therefore been of interest to mechanistically examine the combination of DPP-4 inhibition and metformin.
GLP-1 levels
One study has examined the effect of the combination of sitagliptin and metformin on concentrations of active and inactive GLP-1 after meal ingestion following 24 weeks of treatment (CitationMigoya et al 2007). It was found that both sitagliptin and metformin alone increased the postmeal concentration of active GLP-1. Furthermore, when given in combination, the increase in active GLP-1 was more than additive, suggesting a synergistic action of the two compounds.
Islet effects when DPP-4 inhibition is added to metformin
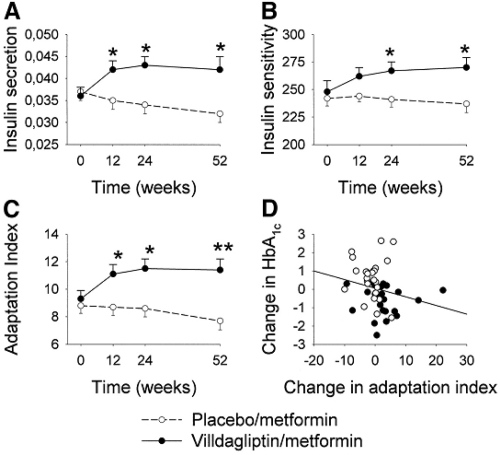
In the initial study on the add-on of vildagliptin to metformin treatment, in which vildagliptin and metformin in combination was compared with metformin alone for 52 weeks (CitationAhrén et al 2004a), a standardized breakfast meal comprising of 465 kcal was served at baseline and after 12, 24 and 52 weeks of treatment. The study evaluated insulin secretion by calculating the suprabasal 30 min area under the C-peptide curve divided by the 30 min increase in glucose after meal ingestion (CitationAhrén et al 2005). It was found that glucose tolerance was improved by the combination therapy versus metformin alone. Thus, the mean between-group difference in AUCglucose was 256 mmol/240 min compared to a baseline of 545 mmol/240 min. Furthermore, insulin secretion increased gradually during the first 24 weeks by the combination therapy and thereafter remained stable for the remaining period of the study (). This shows that the combination of vildagliptin with metformin improves beta cell function. The same study also evaluated insulin sensitivity after meal ingestion by calculating the OGIS (oral glucose insulin sensitivity index). This is a validated index which is based on a model of glucose clearance in relation to meal-derived insulin data (CitationMari et al 2001). It was found that OGIS gradually increased by the combination therapy (). The combined estimation of insulin secretion and insulin sensitivity allowed the estimation of the adaptation (the product of insulin secretion and sensitivity); the adaptation index gives a Figure of the ability of the beta-cell to adapt insulin secretion to the ambient insulin sensitivity (CitationAhrén and Pacini 1997). It was found (see also ) that the adaptation index increased by the combination of vildagliptin and metformin versus metformin alone. This change in adaptation index across the entire study group showed a negative correlation with the change in HbA1c (r = −0.39, p = 0.004) (see ). Hence, this analysis of potential mechanisms of action underlying the improved glycemic control by the combination of vildagliptin and metformin versus metformin alone showed a marked improvement in beta cell function and a slight improvement in insulin sensitivity which together results in improved beta cell adaptation ability to insulin resistance, a measure that correlated to the reduction in HbA1c. Furthermore, from this study, also baseline and prandial proinsulin levels have been carefully analyzed, and the results have shown a reduction in proinsulin levels in subjects given vildagliptin and metformin in combination versus metformin alone (CitationAhrén et al 2007), which further adds to the conclusion that vildagliptin improves beta cell function when added to metformin in subjects with type 2 diabetes.
Figure 5 Insulin secretion (evaluated as the 30 min suprabasal AUCC-peptide following meal ingestion divided by the 30 min increase in glucose), insulin sensitivity (evaluated by the OGIS estimation) and adaptation index (insulin secretion times insulin sensitivity) at baseline and after 12, 24 and 52 weeks of treatment with vildagliptin at 50 mg daily in combination with metformin (n = 31) versus treatment with metformin (n = 26). Low right panel shows the change in HbA1c after the 52 week treatment period as a function of change in adaptation index in the same study. Reproduced from CitationAhrén et al 2005 after permission from the American Diabetes Association.
Another study has examined glucose tolerance and indirect markers of beta cell function after meal ingestion following 24 weeks of addition of vildagliptin at 50 or 100 mg daily to on-going metformin (>1.5 g daily) (CitationBosi et al 2007). A standard breakfast consisting of 500 kcal was served after the 24 week treatment. Glucose tolerance was determined by prandial glucose levels. Insulin secretion was evaluated by calculating the total 2 h insulin secretion by deconvoluting plasma C-peptide levels and then dividing this Figure by the area under the 2 h glucose curve. It was found that following the 24 weeks of treatment, subjects given vildagliptin (either 50 or 100 mg daily) in combination with metformin had lower fasting and prandial glucose than subjects given metformin alone. For example, the placebo-adjusted mean 2 hr plasma glucose following meal ingestion was reduced by 1.9 mmol/l by vildagliptin at 50 mg daily and by 2.3 mmol/l by vildagliptin at 100 mg from a baseline of 13.5 mmol/l. Furthermore, beta cell function, was increased in subjects given vildagliptin in combination with metformin versus metformin alone.
Insulin secretion and insulin sensitivity were also determined in the four week study when sitagliptin at 50 mg twice daily was given to on-going metformin therapy (CitationBrazg et al 2007). Insulin secretion was evaluated by modeling C-peptide data after a standardized breakfast meal comprising 765 kcal (CitationBreda and Copbelli 2001) and insulin sensitivity was determined with a composite index, insulin sensitivity index (CitationMatsuda and DeFronzo 1999). It was found that insulin secretion, as evaluated by this model, was significantly improved after treatment with sitagliptin in combination with metformin versus with metformin alone (CitationBrazg et al 2007). Furthermore, insulin sensitivity was numerically increased, although this did not reach significance. finally, the authors also calculated the disposition index, which is insulin secretion (based on insulin levels) times insulin sensitivity, and it was substantially elevated by the combination therapy. Therefore, also this study showed a clear stimulation of insulin secretion by the combination of metformin with a DPP-4 inhibitor.
Beta cell function and insulin sensitivity were as well estimated in the 24 week study with sitagliptin at 100 mg once daily as add-on to metformin (CitationCharbonnel et al 2006). It was found that after 24 weeks of treatment, along with a reduction in HbA1c and fasting glucose, the combination of sitagliptin and metformin increased fasting insulin and glucose as well as the homeostasis model assessment of β-cell function (HOMA-β, CitationMatthews et al 1985) and the insulin sensitivity marker, quantitative insulin sensitivity (QUICKI, Katz et al 2000). Furthermore, the combination of sitagliptin and metformin also reduced the proinsulin to insulin ratio under fasting conditions, which is a sign of improved beta cell function. In contrast, in this study, fasting proinsulin levels per se were not altered and the homeostasis model assessment of insulin (HOMA-IR), which is based on the fasting levels of glucose and insulin (CitationMatthews et al 1985) was not altered. Furthermore, in this study, the subjects also received a standardized meal after 24 weeks treatment. It was found that sitagliptin in combination with metformin significantly reduced the post-meal glycemia in association with enhancement of postmeal insulin and C-peptide levels as well as the determination of insulin secretion by calculating the postmeal insulin to glucose ratio, all in comparison with treatment with metformin alone.
Islet function when DPP-4 inhibition and metformin are used in initial combination therapy
In the study in which sitagliptin and metformin are given as initial combination therapy (CitationGoldstein et al 2007), a standardized meal tolerance test was given after 24 weeks of treatment with analyses of glucose, insulin and C-peptide. It was found that along with the reduction in fasting glucose, the prandial glycemia was improved both by sitagliptin and metformin in monotherapy but an additive effect in reducing prandial glycemia was observed. Thus, the placebo-adjusted reduction in mean 2 h postmeal glucose was 6.5 mmol/l from the baseline 2 hr glucose of 15.9 mmol/l in the subjects given sitagliptin 50 mg + metformin 1000 mg twice daily. Also insulin secretion, as determined by the AUCinsulin divided by AUCglucose during the 2 hr postmeal period, was significantly increased by the combination therapy in an additive manner versus monotherapy. Thus, the placebo-adjusted increase in mean insulin secretion was 0.07 μU hr insulin/ml/mg h glucose/dl versus 0.16 at baseline, ie, an increase by 43%. The study also showed a significant reduction in fasting proinsulin and in fasting proinsulin to insulin ratios after 24 weeks treatment with the combination of sitagliptin and metformin, again reinforcing an improved beta-cell function by this combination therapy. Furthermore, when calculating the insulin resistance index, HOMA-IR, a marked improvement in insulin sensitivity was seen by the combination; the placebo-adjusted value of HOMA-IR was reduced by 2.7 from a baseline of 6.2, ie, by 41%.
To summarize, the mechanistic studies of combination treatment with DPP-4 inhibition and metformin show increased GLP-1 levels and increased insulin secretion and insulin sensitivity. Nevertheless, more studies are required to fully understand the benefits of this combination, including effects on glucagon secretion.
Conclusions
DPP-4 inhibition has been shown to be antidiabetic when used both in monotherapy (CitationAhrén et al 2004b; CitationAschner et al 2006; CitationPratley et al 2006; CitationRaz et al 2006; CitationRistic et al 2005; CitationRosenstock et al 2007; CitationSchweizer et al 2007; CitationScott et al 2007) and in combination with metformin (CitationAhrén et al 2004a; CitationBosi et al 2007; CitationBrazg et al 2007; CitationCharbonnel et al 2006; CitationGoldstein et al 2007), thiazolidinediones (CitationGarber et al 2007; CitationRosenstock et al 2006; CitationRosenstock et al 2007) and insulin (CitationFonseca et al 2007). This novel strategy to treat type 2 diabetes is expected to be of increasing value in the future treatment of type 2 diabetes. The overall experience is that this novel strategy is efficient, highly tolerable and safewith a minimal risk for hypoglycemic events. A promising place in therapy for DPP-4 inhibition is in combination with metformin. This has been demonstrated in large studies with vildagliptin and sitagliptin, since these studies have shown that HbA1c is reduced by 0.65%–1.1% from baseline levels of 7.8%–8.4% in studies up to 52 weeks. This improvement in glycemic control is similar as in studies with sulphonylureas, thizolidinediones or exenatide when added to metformin treatment. Furthermore, DPP-4 inhibition in combination with metformin is safeand tolerable. Hence, a major indication for treatment with DPP-4 inhibition as add-on to metformin in subjects inadequately controlled with metformin and as first-line treatment in initial combination therapy with metformin. For future studies, the durability of effects of the combination of DPP-4 inhibition with metformin needs to be explored as well as more detailed mechanistic studies need to be undertaken, with particular to studies on glucagon secretion, prandial lipid levels and insulin sensitivity.
References
- AhrénBVildagliptin: an inhibitor of dipeptidyl peptidase-4 with antidiabetic propertiesExp Opin Invest Drugs20061543142
- AhrénBDipeptidyl peptidase-4 inhibitors – clinical data and clinical implicationsDiabetes Care2007a30134450
- AhrénBBarnettABaileyCDPP-4 inhibitorsBest practice and research: clinical endocrinology and metabolism; novel therapies of diabetes2007b
- AhrénBPaciniGImpaired adaptation of first-phase insulin secretion in postmenopausal women with glucose toleranceAm J Physiol1997273E70179357798
- AhrénBSimonssonELarssonHInhibition of dipeptidyl peptidase IV improves metabolic control over a 4 week study period in type 2 diabetesDiabetes Care2002258697511978683
- AhrénBSchmitzOGLP-1 receptor agonists and DPP-4 inhibitors in the treatment of type 2 diabetesHorm Metab Res2004368677615655721
- AhrénBGomisRStandlETwelve- and 52-week efficacy of the dipeptidyl peptidase IV inhibitor LAF237 in metformin-treated patients with type 2 diabetesDiabetes Care2004a27287480
- AhrénBLandin-OlssonMJanssonPAInhibition of dipeptidyl peptidase-4 reduces glycemia sustains insulin levels and reduces glucagon levels in type 2 diabetesJ Clin Endocrinol Metab2004b89207884
- AhrénBFoleyJEPaciniGImproved meal-related β-cell function and insulin sensitivity by the dipeptidyl peptidase-IV inhibitor vildagliptin in metformin-treated patients with type 2 diabetes over 1 yearDiabetes Care20052819364016043735
- AhrénBPaciniGTuraAImproved meal-related insulin processing contributes to the enhancement of B-cell function by the DPP-4 inhibitor vildagliptin in patients with type 2 diabetesHorm Metab Res200739826917992639
- AschnerPKipnesMSLuncefordJKEffect of the dipeptidyl peptidase-4 inhibitor sitagliptin as monotherapy on glycemic control in patients with type 2 diabetesDiabetes Care2006292632717130196
- BaileyCJTurnerRCMetforminN Engl J Med199633457498569826
- BalasBBaigMRWatsonCThe dipeptidyl peptidase IV inhibitor vildagliptin suppresses endogenous glucose production and enhances islet function after single-dose administration in type 2 diabetic patientsJ Clin Endocrinol Metab20079212495517244786
- BosiECamisascaRPColloberCEffects of vlidagliptin on glucose control over 24 weeks in patients with type 2 diabetes inadequately controlled with metforminDiabetes Care200730890517277036
- BrazgRXuLDalla ManCEffect of adding sitagliptin, a dipeptidyl peptidase-4 inhibitor, to metformin on 24-h glycaemic control and β-cell function in patients with type 2 diabetesDiabetes Obes Metab200791869317300594
- BredaECobelliCInsulin secretion rate during glucose stimuli: alternative analyses of C-peptide dataAnn Biomed Eng20012969270011556725
- CharbonnelBSchernthanerGBrunettiPLong-term efficacy and tolerability of add-on pioglitazone therapy to failing monotherapy compared with addition of gliclazide or metformin in patients with type 2 diabetesDiabetes2005481093104
- CharbonnelBWuMKarasikAEfficacy and safety of the dipeptidyl peptidase-4 inhibitor sitagliptin added to ongoing metformin therapy in patients with type 2 diabetes inadequately controlled with metformin aloneDiabetes Care20062926384317130197
- ConsoliAGomisRHalimiSInitiating oral glucose-lowering therapy with metformin in type 2 diabetic patients: an evidence-based strategy to reduce the burden of late-developing diabetes complicationsDiabetes Metab2004305091615671920
- DeaconCFDipeptidyl peptidase 4 inhibition with sitagliptin: a new therapy for type 2 diabetesExp Opin Invest Drugs20071653345
- DeFronzoRHissaMBlauwetMBSaxagliptin added to metformin improves glycemic control in patients with type 2 diabetesDiabetes200756Suppl 1A74
- DeFronzoRAPathogenesis of type 2 diabetes mellitusMed Clin North Am20048878783515308380
- DeFronzoRARatnerREHanJEffects of exenatide (exendin-4) on glycemic control and weight over 30 weeks in metformin-treated patients with type 2 diabetesDiabetes Care200528109210015855572
- Del PratoSPulizziNThe place of sulfonylureas in the therapy for type 2 diabetes mellitusMetabolism200655S20716631807
- DerosaSGaddiAVPiccinniMNDifferential effect of glimepiride and rosiglitazone on metabolic control of type 2 diabetic patients treated with metformin: a randomized double-blind, clinical trialDiabetes Obes Metab2006819720516448524
- DonnellyLAFoneyASFHattersleyATThe effect of obesity on glycaemic response to metformin or sulphonylureas in type 2 diabetesDiabetic Med2006231283316433709
- DruckerDJNauckMAThe incretin system: glucagon-like peptide-1 receptor agonists and dipeptidyl peptidase-4 inhibitors in type 2 diabetesLancet2006368169670517098089
- DunningBEFoleyJAhrénBAlpha-cell function in health and disease: influence of GLP-1Diabetologia20054817001316132964
- fenglosMMSaadMFPi-SinyerFXEffects of liragflutide (NN2211) , a long-acting GLP-1 analogue, on glycaemic control and bodyweight in subjects with type 2 diabetesDiabet Med20052210162316026367
- FonsecaVSchweizerAAlbrechtDAddition of vildagliptin to insulin improves glycaemic control in type 2 diabetesDiabetologia20075011485517387446
- GallwitzBReview of sitagliptin phosphate: a novel treatment for type 2 diabetesVasc Health Risk Manag200732031017580730
- GarberAJSchweizerABaronMAVildagliptin in combination with pioglitazone improves glycaemic control in patients with type 2 diabetes failing thiazolidinedione monotherapy: a randomized, placebo-controlled studyDiabet Obes Metab2007916674
- GinnarelliRAragonaMCoppelliAReducing insulin resistance with metformin: the evidence todayDiabetes Metab2003296S283514502098
- GoldsteinBJFeinglosMNLuncefordJKEffect of initial combination therapy with sitagliptin, a dipeptidyl peptidase-4 inhibitor, and metformin on glycemic control in patients with type 2 diabetesDiabetes Care20073019798717485570
- GreenJBFeinglosMNAre sulphonylureas passé?Curr Diabet Rep200763737
- GutzwillerJPDreweJGökeBGlucagon-like peptide-1 promotes satiety and reduces food intake in patients with diabetes mellitus type 2Am J Physiol1999276R1541410233049
- HermanGABergmanAYiBTolerability and pharmacokinetics of metformin and the dipeptidyl peptidase 4 inhibitor sitagliptin when co-administered in patients with type 2 diabetesCurr Med Res Opin20062219394717022853
- HinkeSAKuhn-WacheKHoffmanTMetformin effects on dipeptidylpeptidase IV degradation of glucagon-like peptide-1Biochem Biophys Res Commun20022911302811883961
- HolstJJDeaconCFInhibition of the activity of dipeptidyl-peptidase IV as a treatment for type 2 diabetesDiabetes1998471663709792533
- HundalRSInzucchiSEMetformin: new understandings, new usesDrugs20036318799412930161
- IkedaTIwataKMurakamiHInhibitory effect of metformin on intestinal glucose absorption in the perfused rat intestineBiochem Biopharmacol20005988790
- InzucchiSEOral antihyperglycemic therapy for type 2 diabetes: scientific reviewJAMA20022873607211790216
- KahnSEThe importance of beta-cell failure in the development and progression of type 2 diabetesJ Clin Endocrinol Metab20018640475811549624
- KahnSEHaffnerSMHelseMAGlycemic durability of rosiglitazone, metformin, or glyburide monotherapyN Engl J Med200635524274317145742
- KarasikAWuMWilliams-HermanDSitagliptin added to ongoing metformin therapy provides sustained glycemic control over 54 weeks, with a low incidence of hypoglycaemia and with weight lossDiabetes200756Suppl 1A139
- KatzANambiSSMatherKQuantitative insulin sensitivity check index: a simple, accurate method for assessing insulin sensitivity in humansJ Clin Endocrinol Metab20078524021010902785
- KimDWangLBeconiM(2R)-4-oxo-4-[3-(trifluoromethyl)-5,6-dihydro[1,2,4]triazol[4,3,a]pyrazin-7(8H)-yl]-1-(2,4,5-trifluorophenyl)butan-2-amine: a potent, orally active dipeptidyl peptidase IV inhibitor for the treatment of type 2 diabetesJ Med Chem2005481415115634008
- LeverveKMGuigasBDetailleDMitochondrial metabolism and type-2 diabetes: a specific target of metforminDiabetes Metab2003296S889414502105
- LevetranCOral antidiabeti agents in type 2 diabetesCurr Med Res Opin2007239455217407651
- LindsayJRDuffyNAMcKillopAMInhibition of dipeptidyl peptidase IV activity by oral metformin in type 2 diabetesDiabet Med200522654715842525
- MannucciEPierazzuoliEOgnibeneAEffect of metformin on glucagon-like peptide 1 (GLP-1) and leptin levels in obese nondiabetic subjectsDiabetes Care2001244899411289473
- MariAPaciniGMurphyEA model-based method for assessing insulin sensitivity from the oral glucose tolerance testDiabetes Care2001245394811289482
- MariASallasWMHeYLVildagliptin, a dipeptidyl peptidase-IV inhibitor, improves model-assessed beta-cell function in patients with type 2 diabetesJ Clin Endocrinol Metab20059048889415886245
- MatsudaMDeFronzoRAInsulin sensitivity indices obtained from oral glucose tolerance testing: comparison with the euglycemic insulin clampDiabetes Care19992214627010480510
- MatthewsDRHoskerJPRudenskiASHomeostasis model assessment: insulin resistance and beta cell function from fasting plasma glucose and insulin concentrations in manDiabetologia198528412193899825
- MentleinRDipeptidyl-peptidase IV (CD26) – role in the inactivation of regulatory peptidesRegul Pept19998592410588446
- MigoyaEMMillerJLarsonPSitagliptin, a selective DPP-4 inhibitor, and metformin have complementary effects to increase active GLP-1 concentrationsDiabetes200756Suppl 1A74
- NathanDMBuseJBDavidsonMBManagement of hyperglycemia in type 2 diabetes: a consensus algorithm for the initiation and adjustment of therapy. A consensus statement from the American Diabetes Association and the European Association for the Study of DiabetesDiabetes Care20062919637216873813
- NauckMANiedereichholzUEttlerRGlucagon-like peptide-1 inhibition of gastric emptying outweighs its insulinotropic effects in healthy humansAm J Physiol199736E98189374685
- NauckMAMeiningerGShengDEfficacy and safety of the dipeptidyl peptidase-4 inhibitor, sitagliptin, compared with the sulfonylurea, glipizide, in patients with type 2 diabetes inadequately controlled on metformin alone: a randomized double-blind, non-inferiority trialDiabet Obes Metab20079194205
- NissenSEWolskiKEffect of rosiglitazoine on the risk of myocardial infarction and death from cardiovascular causesN Engl J Med200735624577117517853
- PerfettiRHuiHThe role of GLP-1 in the lifeand death of pancreatic beta cellsHorm Metab Res2004368041015655712
- PratleyREJauffret-KamelSTwelve-week monotherapy with the DPP-4 inhibitor vildagliptin improves glycemic control in subjects with type 2 diabetesHorm Metab Res20063874233816823726
- RazIHanefeldMXuLEfficacy and safety of the dipeptidyl peptidase-4 inhibitor sitagliptin as monotherapy in patients with type 2 diabetes mellitusDiabetologia20064925647117001471
- RisticSByiersSFoleyJImproved glycaemic control with dipeptidyl peptidase-4 inhibition in patients with type 2 diabetes: vildagliptin (LAF237) dose responseDiabet Obes Metab200576928
- RosenstockJBrazgRAndryukPJEfficacy and safety of the dipeptidyl peptidase-4 inhibitor sitagliptin added to ongoing pioglitazone therapy in patients with type 2 diabetes: a 24-week multicenter, randomized, double-blind, placebo-controlled, parallel-group studyClin Ther20062815566817157112
- RosenstockJBaronMACamisascaRPEfficacy and tolerability of initial combination therapy with vildagliptin and pioglitazone compared with component monotherapy in patients with type 2 diabetesDiabetes Obes Metab200791758517300593
- SchweizerACouturierAFoleyJEComparison between vildagliptin and metformin to sustain reductions in HbA1c over 1 year in drug-naïve patients with type 2 diabetesDiabet Med2007249556117509069
- ScottRWuMSanchezMEfficacy and tolerability of the dipeptidyl peptidase-4 inhibitor sitagliptin as monotherapy over 12 weeks in patients with type 2 diabetesInt J Clin Pract2007611718017156104
- SetterSMIltzJLThamsJMetformin hydrochloride in the treatment of type 2 diabetes mellitus: a clinical review with a focus on dual therapyClin Ther2003252991302614749143
- StrattonIMAdlerAINeilHAAssociation of glycaemia with macrovascular and microvascular complications of type 2 (UKPDS 35): prospective observational studyBr Med J20003214051210938048
- StumvollMNurjhanNPerrielloGMetabolic effects of metformin in non-insulin-dependent diabetes mellitusN Engl J Med199533355047623903
- UmpierrezGIssaMVlanjnicAGlimepiride versus pioglitazone combination therapy in subjects with type 2 diabetes inadequately controlled on metformin monotherapy: results of a randomized clinical trialCurr Med Res Opin200622751916684436
- VellaABockGGieslerPDEffects of dipeptidyl peptidase 4 inhibition on gastrointestinal function, meal appearance and glucose metabolism in type 2 diabetesDiabetes20075614758017303799
- VilsbøllTKrarupTMadsbadSDefective amplification of the late phase insulin response to glucose by GIP in obese type II diabetic patientsDiabetologia20024511111912189441