Abstract
Background
Angiotensin-converting enzyme inhibitors (ACEI) have a well-established role in the prevention of cardiovascular events in hypertension, left ventricular dysfunction, and heart failure. More recently, ACEI have been shown to prevent cardiovascular events in individuals with increased cardiovascular risk, where hypertension, left ventricular dysfunction, or heart failure was not the primary indication for ACEI therapy.
Objective
To review studies of the effects of the ACEI perindopril on cardiovascular events.
Method
The EUROPA (European Trial on Reduction of Cardiac Events with Perindopril in Patients with Stable Coronary Artery Disease Study), PROGRESS (Perindopril Protection Against Recurrent Stroke Study), and ASCOT-BPLA (Anglo-Scandinavian Cardiac Outcomes Trial – Blood Pressure Lowering Arm) trials are reviewed.
Results
Perindopril alone reduced cardiovascular events in subjects with stable coronary heart disease. Perindopril in combination with indapamide reduced cardiovascular events in subjects with cerebrovascular disease. Perindopril in combination with amlodipine reduced cardiovascular events in subjects with hypertension.
Conclusion
Perindopril reduced cardiovascular events. The reduction of cardiovascular events by perindopril was in large part associated with reduction of blood pressure, and greater reduction in cardiovascular events was associated with greater reduction of blood pressure. Perindopril may need to be combined with other antihypertensive agents to maximize reduction of cardiovascular events.
Introduction
Angiotensin-converting enzyme inhibitors (ACEI) have a well established role in prevention of cardiovascular events in hypertension (CitationChobanian et al 2003; CitationBPLTTC 2005), left ventricular dysfunction (CitationFlather et al 2000), and heart failure (CitationFlather et al 2000; CitationRemme and Swedberg 2001; CitationHunt et al 2005). More recently, ACEI have been shown to prevent cardiovascular events in individuals with increased cardiovascular risk, where hypertension, left ventricular dysfunction, or heart failure was not the primary indication for ACEI therapy (CitationHOPE 2000; CitationPROGRESS 2001, Citation2003; CitationEUROPA 2003). This review will summarise and comment on three recent studies of the effects of the ACEI perindopril on cardiovascular events, the EUROPA (European Trial on Reduction of Cardiac Events with Perindopril in Patients with Stable Coronary Artery Disease Study) and PROGRESS (Perindopril Protection Against Recurrent Stroke Study) studies where the effects of perindopril were studied alone (CitationPROGRESS 2001, Citation2003; CitationEUROPA 2003), or in combination with the diuretic indapamide (CitationPROGRESS 2001, Citation2003), and the ASCOT-BPLA (Anglo-Scandinavian Cardiac Outcomes Trial – Blood Pressure Lowering Arm) study where perindopril was added to therapy with the calcium-channel blocker amlodipine (CitationDahlof et al 2005).
ASCOT-BPLA provides no direct evidence about the effects of perindopril on cardiovascular events (CitationDahlof et al 2005). However, it does provide limited evidence for the effect of perindopril in combination with amlodipine on cardiovascular events. The vast majority of subjects allocated to amlodipine-based therapy in ASCOT-BPLA required one or more additional antihypertensive agents which, for 59% of subjects, included perindopril. Thus, perindopril played an essential role in blood pressure (BP) reduction for most subjects allocated to the amlodipine-based regimen.
EUROPA
EUROPA was a randomized placebo-controlled, double-blind study of the effects of perindopril therapy on cardiovascular events in 12 218 subjects with previous myocardial infarction (MI), angiographic evidence of coronary heart disease (CHD), coronary revascularization, or a positive stress test () (CitationEUROPA 2003). Past history of heart failure was recorded in 1.3% of subjects, but none had clinical signs of heart failure, with 10% in New York Heart Association class I and none in class II or higher. Subjects were randomized to either 8 mg perindopril or placebo.
Table 1 Summary of EUROPA trial
It is notable that although only 27% of subjects had a diagnosis of hypertension (BP > 160/95 mm Hg or receiving antihypertensive treatment), the mean baseline systolic BP (SBP) was 137 mm Hg, with a standard deviation of 16 mm Hg, indicating that a sizable proportion were hypertensive (CitationChobanian et al 2003). In comparison with placebo, perindopril reduced BP by 5/2 mm Hg.
During a mean follow-up of 4.2 years, perindopril reduced the primary outcome (composite of cardiovascular death, non-fatal MI, cardiac arrest with successful resuscitation) from 9.9% to 8.0% (20% decrease, 95% confidence interval (CI) 9% to 29%; number needed to treat (NNT)=53). The main contributor to this reduction in the primary outcome was the reduction in non-fatal MI from 6.2% to 4.8% (22% decrease, 95% CI 10% to 33%; NNT=74); the reduction in cardiovascular mortality from 4.1% to 3.5% (14% decrease, 95% CI −3% to 28%) did not achieve statistical significance. The incidence of cardiac arrest was only 0.2% with placebo and 0.1% with perindopril (46% decrease, 95% CI −47% to 80%). Perindopril also reduced the incidence of heart failure requiring hospitalization from 1.7% to 1.0% (39% decrease, 95% CI 17% to 56%; NNT=153), but produced only a slight reduction in stroke from 1.7% to 1.6%. Perindopril produced similar benefits in both hypertensive (BP >160/95 mm Hg or receiving antihypertensive treatment on enrollment) and nonhypertensive subjects.
Perindopril produced similar effects in EUROPA participants with diabetes, although this substudy had insufficient power to show statistical significance (CitationDaly et al 2005).
PROGRESS
The PROGRESS study was a randomized placebocontrolled double-blind study of the effects of perindoprilbased therapy on stroke and other cardiovascular outcomes in 6105 subjects with a history of ischemic or hemorrhagic stroke, or transient ischemic attack within the previous 5 years () (CitationPROGRESS 2001, Citation2003). Active therapy was 4 mg perindopril, with the addition of 2.5 mg indapamide (2 mg in Japan) if the physician felt there was no contraindication to a diuretic. Those for whom their physician recommended single drug therapy were randomized to receive either perindopril or single placebo. Those for whom their physician recommended combination drug therapy were randomized to receive either perindopril plus indapamide or double placebo.
Table 2 Summary of PROGRESS trial
Whereas all PROGRESS participants had cerebro-vascular disease, only 16% had CHD (history of MI or coronary revascularization, or angina). While there were no BP entry criteria, it was recommended that subjects enrolled in PROGRESS have their hypertension controlled by medication other than ACEI and angiotensin type 1 receptor blocker (ARB) before enrolment. Despite this recommendation, the mean SBP on enrolment was 147 mm Hg, and 48% had SBP >160 mm Hg or diastolic BP (DBP) >90 mm Hg (CitationPROGRESS 2001, Citation2003). Heart failure was an exclusion criterion. In comparison with placebo, combination of perindopril and indapamide during the PROGRESS trial reduced BP by 12/5 mm Hg, whereas perindopril alone reduced BP by 5/3 mm Hg.
During a mean follow-up of 3.9 years, the combination of perindopril and indapamide reduced stroke incidence from 14.4% to 8.4% (43% decrease, 95% CI 30% to 54%; NNT=17), reduced major coronary events (non-fatal MI or death ascribed to CHD) from 5.7% to 3.9% (35% decrease, 95% CI 12% to 52%; NNT=51), and reduced heart failure incidence (hospitalization or requiring withdrawal of randomized therapy) from 4.6% to 3.1% (34% decrease, 95% CI 7% to 53%; NNT=66). Perindopril alone produced non-statistically significant reductions in stroke incidence from 12.9% to 12.3% (5% decrease, 95% CI −19% to 23%), major coronary events from 4.1% to 3.7% (7% decrease, 95% CI −37% to 38%) and heart failure incidence from 5.4% to 4.5% (16% decrease, 95% CI −19% to 41%). The effects of perindopril-based therapy were similar for both hypertensive (SBP ≥160 mm Hg or DBP ≥90 mm Hg on enrollment) and nonhypertensive subjects.
ASCOT-BPLA
ASCOT-BPLA was a prospective randomized comparison of amlodipine–perindopril and atenolol–bendro-flumethiazide antihypertensive regimens on non-fatal MI (including silent MI) and fatal CHD in 19 257 hypertensive subjects with at least three other cardiovascular risk factors () (CitationDahlof et al 2005). The amlodipine-based regimen was 5–10 mg amlodipine with addition of 4–8 mg perindopril as required. The atenolol-based regimen was 50–100 mg atenolol with addition of 1.25–2.5 mg bendro-flumethiazide and potassium as required. By the end of the study, most subjects were taking at least two antihypertensive agents, and only 15% and 9% were taking amlodipine and atenolol monotherapy, respectively. On average, of total time, 83% were taking amlodipine as allocated, 79% were taking atenolol, 59% were taking perindopril, and 66% were taking bendroflumethiazide. Overall, throughout the trial, a mean of 50% were taking the combination of amlodipine with perindopril as allocated, with or without other antihypertensive drugs. Compared with those allocated to the atenolol-based regimen, BP values were lower throughout the trial in those allocated to the amlodipine-based regimen. These differences were largest (5.9/2.4 mm Hg) at 3 months, and the average difference throughout the trial was 2.7/1.9 mm Hg.
Table 3 Summary of ASCOT-BLPA trial
ASCOT-BPLA was stopped prematurely after 5.5 years' median follow-up. Although the primary endpoint did not achieve statistical significance, compared with the atenolol–bendroflumethiazide regimen, individuals on the amlodipine–perindopril regimen had 10% (95% CI −2% to 21%) lower incidence of fatal CHD or non-fatal MI, 23% (95% CI 11% to 34%; NNT=101) lower incidence of fatal or non-fatal stroke, 16% (95% CI 10% to 22%; NNT=40) lower incidence of total cardiovascular events and procedures, and 11% (95% CI 1% to 19%; NNT=117) lower all-cause mortality. However, the reduction in fatal and non-fatal heart failure from 3.0% to 2.5% (16% decrease, 95% Perindopril and vcardiovascular events CI −5% to 34%) with the amlodipine–perindopril regimen did not achieve statistical significance.
Why does perindopril reduce cardiovascular events?
There is continuing debate about the role of BP reduction in the prevention of cardiovascular events by BP-lowering therapy. This debate is fuelled by studies showing decreases in cardiovascular event rate greater than can be accounted for by BP reduction (CitationLewis et al 1993; CitationHOPE 2000; CitationEUROPA 2003). This debate is based in part on the assumption that BP has a causal role in cardiovascular disease pathogenesis. This assumption may not, however, be correct, except in extreme situations such as flash pulmonary edema due to acute severe elevation of BP.
Rather than cause cardiovascular events, elevated BP may be the consequence of changes in the heart and vasculature that overlap those that lead to cardiovascular events (). BP is the product of cardiac output (CO) and systemic peripheral resistance (SVR). Thus, change in BP is necessarily dependent upon change in cardiac and vascular function that produces change in CO and/or SVR. Many candidate mechanisms for the pathogenesis of hypertension have been proposed (CitationGuyton et al 1995; CitationBeevers et al 2001; CitationJohnson et al 2002; CitationZandi-Nejad et al 2006), including the possible role of structural and functional changes in the vasculature (CitationMark 1984; CitationNoon et al 1997; CitationSimon 2004; CitationSkov and Mulvany 2004; CitationWong et al 2004; CitationSafar and Boudier 2005; CitationIkram et al 2006). Moreover, hypertension is associated with endothelial dysfunction and other risk factors for cardiovascular disease (CitationLip et al 1995, Citation1999; CitationLandray et al 2002; CitationKing et al 2004). Of particular interest is the possibility that angiotensin II may participate in the pathogenesis of both hypertension and cardiovascular disease (CitationSimon 2004).
Figure 1 Possible relationship between heart and blood vessel abnormalities that influence cardiac output (CO) and systemic vascular resistance (SVR), thereby influencing blood pressure (BP), and heart and blood vessel diseases that cause cardiovascular events.
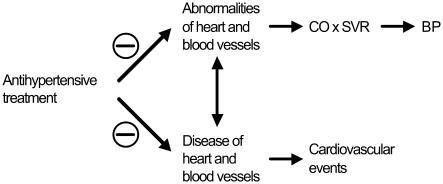
BP may therefore have little if any causal role in the pathogenesis cardiovascular events, and may show variable change in response to cardiovascular disease-reducing therapy. However, when this therapy does lower BP, even within the normal range, it can serve as a valuable marker of reduced cardiovascular risk. Most cardiovascular disease is associated with BP levels below the current definition of hypertension (CitationWHO 2002), and there is a continuous association between usual BP and cardiovascular event risk down to 115 mm Hg SBP and 75 mm Hg DBP (PSC 2000).
There is ample evidence that perindopril has actions on the heart and blood vessels that may reduce cardiovascular disease. In addition to many studies in animals, studies in humans show perindopril corrected endothelial dysfunction (CitationBijlstra et al 1995; CitationWatanabe et al 2005), and reduced ventricular remodelling following MI (CitationFerrari et al 2006). In addition, perindopril–indapamide improved arterial stiffness and wave reflection, and reduced left ventricular mass in hypertensive subjects (CitationAsmar et al 2001; Citationde Luca et al 2004), and reduced albuminuria in diabetic subjects (CitationMogensen et al 2003). Amlodipine–perindopril reduced central pulse pressure more than atenolol in a substudy of the ASCOT study, indicative of increased aortic compliance (CitationCAFE 2006).
The EUROPA investigators proposed the reduction in cardiovascular events by perindopril in the EUROPA study was greater than might be expected for the observed reduction in BP (mean 5/2 mm Hg), and may have been due to antiatherosclerotic effects of ACE inhibition. In contrast to the EUROPA study, BP reduction was a key indicator of reduced cardiovascular event rates in the PROGRESS study, given the greater reductions in BP and cardiovascular events seen with 4 mg perindopril in combination with indapamide, than with 4 mg perindopril alone. The EUROPA study suggests that 8 mg perindopril may have produced greater reduction in cardiovascular events than produced by 4 mg perindopril alone in the PROGRESS study. Conversely, the PROGRESS data raise the possibility that a greater reduction in cardiovascular events may have been seen in the EUROPA study if perindopril had been combined with a diuretic.
Whereas analyses by the Blood Pressure Treatment Trialists' Collaboration suggest the size of the absolute BP reduction is a more important indicator of the relative cardiovascular disease-prevention by antihypertensive drugs than is the antihypertensive drug choice, there are exceptions emerging (CitationBPLTT 2005). Thus, calcium channel blockers appear to be inferior to other antihypertensive agents for the prevention of heart failure (CitationBPLTT 2005). Moreover, data from the Losartan Intervention For Endpoint Reduction (LIFE) study suggest losartan may provide better protection from stroke than atenolol, although losartan- and atenolol-based therapies had similar effects on cardiac outcomes (CitationDahlof et al 2002). By contrast, the lower MI event rate with amlodipine than valsartan therapy in the Valsartan Antihypertensive Long-term Use Evaluation (VALUE) study was associated with a greater BP reduction by amlodipine (CitationJulius et al 2004; CitationWeber et al 2004).
Extensive analyses of the relationship between the benefits of therapy and BP lowering in the ASCOT-BPLA study provide indirect support for non-BP mechanisms in mediating the superior prevention of cardiovascular events by the amlodipine–perindopril regimen. Reduction in cardiovascular events by the amlodipine–perindopril regimen was associated not only with a greater reduction of BP, but also with a faster pulse, and beneficial alterations in body weight, serum high density lipoprotein (HDL) cholesterol, triglycerides, creatinine, and potassium, and fasting glucose levels (CitationPoulter et al 2005). All of these variables are independent risk factors for cardiovascular events. When each of these variables was analyzed separately for its effect on the difference between the cardiovascular event rates for the two treatment regimens, differences in HDL cholesterol had the biggest association with differences in coronary event rates, whereas only differences in BP were materially associated with the stroke event rate. The effects of the amlodipine–perindopril regimen, relative to the atenolol–bendrofluthiazide regimen, on cardiovascular events were attenuated, but remained statistically significant, when analyses were adjusted for BP alone. However, multivariate adjustment for all risk factors accounted for half of the difference in coronary events and for about 40% of the difference in stroke events between the amlodipine–perindopril and atenolol–bendrofluthiazide regimens, and the residual differences in event rates were no longer statistically significant (CitationPoulter et al 2005).
The EUROPA investigators argued that some of the benefits of lipophilic ACEI such as perindopril and ramipril may be due to increased tissue penetration (CitationEUROPA 2003). However, the effects of ACEI are dose-related (CitationCampbell et al 1994), and studies in man showed that although perindoprilat is more lipophilic, with more rapid and efficient myocardial uptake than enalaprilat, the two ACEI produced similar changes in angiotensin and bradykinin peptide levels in arterial and coronary sinus blood of humans with CHD (CitationZeitz et al 2003).
Should ACEI be given to all patients with CHD?
Discussion of the EUROPA study has emphasized that the benefits of perindopril were in addition to other preventive measures, including the relatively high use of platelet inhibitors (92%), β blockers (62%) and lipid lowering therapy (58%) (CitationEUROPA 2003). Nevertheless, the Prevention of Events with Angiotensin Converting Enzyme Inhibition (PEACE) trial suggests ACEI may have less benefit in CHD if other preventive measures are more effectively implemented (CitationPEACE 2004). The PEACE study was a randomized placebo-controlled double-blind study of the effects of 4 mg trandolapril on cardiovascular events in 8290 subjects with stable CHD and preserved left ventricular function (CitationPEACE 2004). During a median follow-up of 4.8 years, trandolapril produced non-statistically significant reductions in the primary endpoint (composite of cardiovascular death, MI, and coronary revascularization) from 22.5% to 21.9% (4% decrease, 95% CI −6% to 12%), and in cardiovascular death and non-fatal MI from 8.5% to 8.3% (3% decrease, 95% CI −12% to 17%), although trandolapril reduced hospitalization or death due to heart failure from 3.7% to 2.8% (25% decrease, 95% CI 5% to 41%; NNT=112). However, BP (an indicator of cardiovascular disease risk) at study baseline in PEACE participants (133/78 mm Hg) was lower than the baseline BP in the Heart Outcomes Prevention Evaluation (HOPE) and EUROPA studies, and was similar to the level achieved with ACEI therapy in HOPE and EUROPA. In addition, PEACE participants received more intensive management of risk factors than did those in the HOPE and EUROPA studies, with 70% of PEACE participants receiving lipid lowering therapy (29% in HOPE, 56% in EUROPA), and 72% had undergone coronary revascularization before enrollment (40% in HOPE, 54% in EUROPA). Thus, PEACE participants had an event rate similar to that of the general population (1.6% annualized rate of death), and the more aggressive management of their risk factors may have negated any potential benefit from ACEI therapy (CitationPEACE 2004). CitationPitt (2004) suggested that the lack of benefit from trandolapril in the PEACE study may have been due to lower low density lipoprotein (LDL) cholesterol levels in PEACE participants. The Ischemia Management with Accupril post bypass Graft via Inhibition of angiotensin converting enzyme (IMAGINE) study similarly showed a lack of benefit from 40 mg quinapril in optimally treated low-risk patients after coronary artery bypass grafting (CitationKeuper and Verheugt 2005). The PEACE and IMAGINE studies emphasize the importance of addressing modifiable risk factors and incorporating an assessment of individual risks and benefits in making decisions about ACEI therapy in low risk patients with CHD and preserved left ventricular function.
Another important benefit of ACEI and ARB therapy is reduction of diabetes incidence (CitationHansson et al 1999; CitationHOPE 2000; CitationDahlof et al 2002; CitationPEACE 2004). Whether perindopril reduces diabetes incidence is unknown, and combination with indapamide may compromise any antidiabetic action of perindopril. Current trials are of too short duration to reveal the cardiovascular impact of diabetes prevention by ACEI and ARB therapy. Given the increasing incidence of diabetes and its contribution to cardiovascular disease, prevention of diabetes may become one of the main contributors to long-term cardiovascular benefit from ACEI and ARB therapy in the future.
Conclusions
Perindopril reduces cardiovascular events. The reduction of cardiovascular events by perindopril was in large part associated with reduction of BP, and greater reduction of BP was associated with greater reduction in cardiovascular events. Perindopril may need to be combined with other antihypertensive agents to maximize reduction of cardiovascular events.
Disclosures
Duncan J Campbell is recipient of a Career Development Fellowship (Award CR 02M 0829) from the National Heart Foundation of Australia. Duncan J Campbell has had research contracts with Solvay Pharmaceutical Company and Novartis in the last 5 years, and has been a member of an advisory board for Novartis.
References
- AsmarRGLondonGMO'RourkeMEImprovement in blood pressure, arterial stiffness and wave reflections with a very-low-dose perindopril/indapamide combination in hypertensive patient: a comparison with atenololHypertension200138922611641310
- BeeversGLipGYO'BrienEABC of hypertension: The pathophysiology of hypertensionBr Med J20013229121611302910
- BijlstraPJSmitsPLuttermanJAEffect of long-term angiotensin-converting enzyme inhibition on endothelial function in patients with the insulin-resistance syndromeJ Cardiovasc Pharmacol199525658647596136
- [BPLTT] Blood Pressure Lowering Treatment Trialists' CollaborationEffects of different blood pressure-lowering regimens on major cardiovascular events in individuals with and without diabetes mellitus: results of prospectively designed overviews of randomized trialsArch Intern Med200516514101915983291
- [CAFE] The CAFE Investigators; for the Anglo-Scandinavian Cardiac Outcomes Trial (ASCOT) investigatorsDifferential impact of blood pressure-lowering drugs on central aortic pressure and clinical outcomes: principal results of the Conduit Artery Function Evaluation (CAFE) studyCirculation200611312132516476843
- CampbellDJKladisADuncanAMEffects of converting enzyme inhibitors on angiotensin and bradykinin peptidesHypertension199423439498144213
- ChobanianAVBakrisGLBlackHRSeventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood PressureHypertension20034212065214656957
- DahlofBDevereuxRBKjeldsenSECardiovascular morbidity and mortality in the Losartan Intervention For Endpoint reduction in hypertension study (LIFE): a randomised trial against atenololLancet2002359995100311937178
- DahlofBSeverPSPoulterNRPrevention of cardiovascular events with an antihypertensive regimen of amlodipine adding perindopril as required versus atenolol adding bendroflumethiazide as required, in the Anglo-Scandinavian Cardiac Outcomes Trial-Blood Pressure Lowering Arm (ASCOT-BPLA): a multicentre randomised controlled trialLancet200536689590616154016
- DalyCAFoxKMRemmeWJThe effect of perindopril on cardiovascular morbidity and mortality in patients with diabetes in the EUROPA study: results from the PERSUADE substudyEur Heart J20052613697815860521
- de LucaNMallionJMO'RourkeMFRegression of left ventricular mass in hypertensive patients treated with perindopril/indapamide as a first-line combination: the REASON echocardiography studyAm J Hypertens200417660715323062
- [EUROPA] European Trial on Reduction of Cardiac Events with Perindopril in Stable Coronary Artery Disease InvestigatorsEfficacy of perindopril in reduction of cardiovascular events among patients with stable coronary artery disease: randomised, double-blind, placebo-controlled, multicentre trial (the EUROPA study)Lancet2003362782813678872
- FerrariRPerindopril and Remodeling in Elderly with Acute Myocardial Infarction InvestigatorsEffects of angiotensin-converting enzyme inhibition with perindopril on left vascular remodeling and clinical outcome: results of the randomized Perindopril and Remodelling in Elderly with Acute Myocardial Infarction (PREAMI) studyArch Intern Med20061666596616567606
- FlatherMDYusufSKoberLLong-term ACE-inhibitor therapy in patients with heart failure or left-ventricular dysfunction: a systematic overview of data from individual patientsLancet200035515758110821360
- GuytonACHallJEColemanTGLaraghJHBrennerBMThe dominant role of the kidneys in long term arterial pressure regulation in normal and hypertensive statesHypertension: pathophysiology, diagnosis, and management1995New YorkRaven Pr Ltd131126
- HanssonLLindholmLHNiskanenLEffect of angiotensinconverting-enzyme inhibition compared with conventional therapy on cardiovascular morbidity and mortality in hypertension: the Captopril Prevention Project (CAPPP) randomised trialLancet19993536111610030325
- [HOPE] Heart Outcomes Prevention Evaluation Study InvestigatorsEffects of an angiotensin-converting-enzyme inhibitor, ramipril, on cardiovascular events in high-risk patientsN Engl J Med20003421455310639539
- HuntSAAbrahamWTChinMHACC/AHA 2005 Guideline update for the diagnosis and management of chronic heart failure in the adult – summary article: a report of the American College of Cardiology/American Heart Association task force on practice guidelines (Writing Committee to Update the 2001 Guidelines for the Evaluation and Management of Heart Failure): developed in collaboration with the American College of Chest Physicians and the International Society for Heart and Lung Transplantation: Endorsed by the Heart Rhythm SocietyCirculation2005112182552
- IkramMKWittemanJCMVingerlingJRRetinal vessel diameters and risk of hypertension: the Rotterdam studyHypertension2006471899416380526
- JohnsonRJHerrera-AcostaJSchreinerGFSubtle acquired renal injury as a mechanism of salt-sensitive hypertensionN Engl J Med20023469132311907292
- JuliusSKjeldsenSEWeberMOutcomes in hypertensive patients at high cardiovascular risk treated with regimens based on valsartan or amlodipine: the VALUE randomised trialLancet200436320223115207952
- KeuperWVerheugtFWHotline sessions of the 27th European congress of cardiologyEur Heart J2005262596916246833
- KingDEEganBMMainousAG3rdElevation of C-reactive protein in people with prehypertensionJ Clin Hypertens (Greenwich)20046562815470285
- LandrayMJEdmundsELi-Saw-HeeFLAbnormal lowdensity lipoprotein subfraction profile in patients with untreated hypertensionQjm2002951657111865172
- LewisEJHunsickerLGBainRPThe effect of angiotensinconverting-enzyme inhibition on diabetic nephropathyN Engl J Med19933291456628413456
- LipGYBlannADBeeversDGProthrombotic factors, endothelial function and left ventricular hypertrophy in isolated systolic hypertension compared with systolic-diastolic hypertensionJ Hypertens1999171203710466477
- LipGYBlannADZarifisJSoluble adhesion molecule Pselectin and endothelial dysfunction in essential hypertension: implications for atherogenesis? A preliminary reportJ Hypertens199513167488903631
- MarkALStructural changes in resistance and capacitance vessels in borderline hypertensionHypertension19846Suppl IIIIII-69III-736394493
- MogensenCEVibertiGHalimiSEffect of low-dose perindopril/indapamide on albuminuria in diabetes: preterax in albuminuria regression: PREMIERHypertension20034110637112654706
- NoonJPWalkerBRWebbDJImpaired microvascular dilatation and capillary rarefaction in young adults with a predisposition to high blood pressureJ Clin Invest199799187399109431
- [PEACE] PEACE Trial InvestigatorsAngiotensin-convertingenzyme inhibition in stable coronary artery diseaseN Engl J Med200435120586815531767
- PittBACE inhibitors for patients with vascular disease without left ventricular dysfunction—may they rest in PEACE?N Engl J Med200435121151715531768
- PoulterNRWedelHDahlofBRole of blood pressure and other variables in the differential cardiovascular event rates noted in the Anglo-Scandinavian Cardiac Outcomes Trial-Blood Pressure Lowering Arm (ASCOT-BPLA)Lancet20053669071316154017
- [PROGRESS] PROGRESS Collaborative GroupRandomised trial of a perindopril-based blood-pressure-lowering regimen among 6,105 individuals with previous stroke or transient ischaemic attackLancet200135810334111589932
- [PROGRESS] PROGRESS Collaborative GroupEffects of a perindopril-based blood pressure lowering regimen on cardiac outcomes among patients with cerebro-vascular diseaseEur Heart J2003244758412633548
- [PSC] Prospective Studies CollaborationAge-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studiesLancet200236019031312493255
- RemmeWJSwedbergKGuidelines for the diagnosis and treatment of chronic heart failureEur Heart J20012215276011492984
- SafarMEBoudierHSVascular development, pulse pressure, and the mechanisms of hypertensionHypertension200546205915911744
- SimonGPathogenesis of structural vascular changes in hypertensionJ Hypertens20042231015106784
- SkovKMulvanyMJStructure of renal afferent arterioles in the pathogenesis of hypertensionActa Physiol Scand200418139740515283751
- WatanabeSTagawaTYamakawaKInhibition of the reninangiotensin system prevents free fatty acid-induced acute endothelial dysfunction in humansArterioscler Thromb Vasc Biol20052523768016179595
- WeberMAJuliusSKjeldsenSEBlood pressure dependent and independent effects of antihypertensive treatment on clinical events in the VALUE TrialLancet200436320495115207957
- [WHO] World Health OrganizationWorld Health Report 2002: reducing risks, promoting healthy life2002GenevaWHO
- WongTYShankarAKleinRProspective cohort study of retinal vessel diameters and risk of hypertensionBr Med J20043297915175230
- Zandi-NejadKLuyckxVABrennerBMAdult hypertension and kidney disease. The role of fetal programmingHypertension200647502816415374
- ZeitzCJCampbellDJHorowitzJDMyocardial uptake and biochemical and hemodynamic effects of ACE inhibitors in humansHypertension200341482712623947